Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- CAREER FEATURE
- 04 December 2020
- Correction 09 December 2020

How to write a superb literature review
Andy Tay is a freelance writer based in Singapore.
You can also search for this author in PubMed Google Scholar
Literature reviews are important resources for scientists. They provide historical context for a field while offering opinions on its future trajectory. Creating them can provide inspiration for one’s own research, as well as some practice in writing. But few scientists are trained in how to write a review — or in what constitutes an excellent one. Even picking the appropriate software to use can be an involved decision (see ‘Tools and techniques’). So Nature asked editors and working scientists with well-cited reviews for their tips.
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 51 print issues and online access
$199.00 per year
only $3.90 per issue
Rent or buy this article
Prices vary by article type
Prices may be subject to local taxes which are calculated during checkout
doi: https://doi.org/10.1038/d41586-020-03422-x
Interviews have been edited for length and clarity.
Updates & Corrections
Correction 09 December 2020 : An earlier version of the tables in this article included some incorrect details about the programs Zotero, Endnote and Manubot. These have now been corrected.
Hsing, I.-M., Xu, Y. & Zhao, W. Electroanalysis 19 , 755–768 (2007).
Article Google Scholar
Ledesma, H. A. et al. Nature Nanotechnol. 14 , 645–657 (2019).
Article PubMed Google Scholar
Brahlek, M., Koirala, N., Bansal, N. & Oh, S. Solid State Commun. 215–216 , 54–62 (2015).
Choi, Y. & Lee, S. Y. Nature Rev. Chem . https://doi.org/10.1038/s41570-020-00221-w (2020).
Download references
Related Articles

- Research management

My PI yelled at me and I’m devastated. What do I do?
Career Feature 02 MAY 24

How I’m supporting other researchers who have moved to Lithuania
Spotlight 01 MAY 24

I fell out of love with the lab, and in love with business

Plagiarism in peer-review reports could be the ‘tip of the iceberg’
Nature Index 01 MAY 24

Why it’s essential to study sex and gender, even as tensions rise
Editorial 01 MAY 24

How reliable is this research? Tool flags papers discussed on PubPeer
News 29 APR 24

Algorithm ranks peer reviewers by reputation — but critics warn of bias
Nature Index 25 APR 24
W2 Professorship with tenure track to W3 in Animal Husbandry (f/m/d)
The Faculty of Agricultural Sciences at the University of Göttingen invites applications for a temporary professorship with civil servant status (g...
Göttingen (Stadt), Niedersachsen (DE)
Georg-August-Universität Göttingen
Postdoctoral Associate- Cardiovascular Research
Houston, Texas (US)
Baylor College of Medicine (BCM)
Faculty Positions & Postdocs at Institute of Physics (IOP), Chinese Academy of Sciences
IOP is the leading research institute in China in condensed matter physics and related fields. Through the steadfast efforts of generations of scie...
Beijing, China
Institute of Physics (IOP), Chinese Academy of Sciences (CAS)
Director, NLM
Vacancy Announcement Department of Health and Human Services National Institutes of Health DIRECTOR, NATIONAL LIBRARY OF MEDICINE THE POSITION:...
Bethesda, Maryland
National Library of Medicine - Office of the Director
Call for postdoctoral fellows in Molecular Medicine, Nordic EMBL Partnership for Molecular Medicine
The Nordic EMBL Partnership is seeking postdoctoral fellows for collaborative projects in molecular medicine through the first NORPOD call.
Helsinki, Finland
Nordic EMBL Partnership for Molecular Medicine
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
- UConn Library
- Literature Review: The What, Why and How-to Guide
- Introduction
Literature Review: The What, Why and How-to Guide — Introduction
- Getting Started
- How to Pick a Topic
- Strategies to Find Sources
- Evaluating Sources & Lit. Reviews
- Tips for Writing Literature Reviews
- Writing Literature Review: Useful Sites
- Citation Resources
- Other Academic Writings
What are Literature Reviews?
So, what is a literature review? "A literature review is an account of what has been published on a topic by accredited scholars and researchers. In writing the literature review, your purpose is to convey to your reader what knowledge and ideas have been established on a topic, and what their strengths and weaknesses are. As a piece of writing, the literature review must be defined by a guiding concept (e.g., your research objective, the problem or issue you are discussing, or your argumentative thesis). It is not just a descriptive list of the material available, or a set of summaries." Taylor, D. The literature review: A few tips on conducting it . University of Toronto Health Sciences Writing Centre.
Goals of Literature Reviews
What are the goals of creating a Literature Review? A literature could be written to accomplish different aims:
- To develop a theory or evaluate an existing theory
- To summarize the historical or existing state of a research topic
- Identify a problem in a field of research
Baumeister, R. F., & Leary, M. R. (1997). Writing narrative literature reviews . Review of General Psychology , 1 (3), 311-320.
What kinds of sources require a Literature Review?
- A research paper assigned in a course
- A thesis or dissertation
- A grant proposal
- An article intended for publication in a journal
All these instances require you to collect what has been written about your research topic so that you can demonstrate how your own research sheds new light on the topic.
Types of Literature Reviews
What kinds of literature reviews are written?
Narrative review: The purpose of this type of review is to describe the current state of the research on a specific topic/research and to offer a critical analysis of the literature reviewed. Studies are grouped by research/theoretical categories, and themes and trends, strengths and weakness, and gaps are identified. The review ends with a conclusion section which summarizes the findings regarding the state of the research of the specific study, the gaps identify and if applicable, explains how the author's research will address gaps identify in the review and expand the knowledge on the topic reviewed.
- Example : Predictors and Outcomes of U.S. Quality Maternity Leave: A Review and Conceptual Framework: 10.1177/08948453211037398
Systematic review : "The authors of a systematic review use a specific procedure to search the research literature, select the studies to include in their review, and critically evaluate the studies they find." (p. 139). Nelson, L. K. (2013). Research in Communication Sciences and Disorders . Plural Publishing.
- Example : The effect of leave policies on increasing fertility: a systematic review: 10.1057/s41599-022-01270-w
Meta-analysis : "Meta-analysis is a method of reviewing research findings in a quantitative fashion by transforming the data from individual studies into what is called an effect size and then pooling and analyzing this information. The basic goal in meta-analysis is to explain why different outcomes have occurred in different studies." (p. 197). Roberts, M. C., & Ilardi, S. S. (2003). Handbook of Research Methods in Clinical Psychology . Blackwell Publishing.
- Example : Employment Instability and Fertility in Europe: A Meta-Analysis: 10.1215/00703370-9164737
Meta-synthesis : "Qualitative meta-synthesis is a type of qualitative study that uses as data the findings from other qualitative studies linked by the same or related topic." (p.312). Zimmer, L. (2006). Qualitative meta-synthesis: A question of dialoguing with texts . Journal of Advanced Nursing , 53 (3), 311-318.
- Example : Women’s perspectives on career successes and barriers: A qualitative meta-synthesis: 10.1177/05390184221113735
Literature Reviews in the Health Sciences
- UConn Health subject guide on systematic reviews Explanation of the different review types used in health sciences literature as well as tools to help you find the right review type
- << Previous: Getting Started
- Next: How to Pick a Topic >>
- Last Updated: Sep 21, 2022 2:16 PM
- URL: https://guides.lib.uconn.edu/literaturereview
Purdue Online Writing Lab Purdue OWL® College of Liberal Arts
Writing a Literature Review

Welcome to the Purdue OWL
This page is brought to you by the OWL at Purdue University. When printing this page, you must include the entire legal notice.
Copyright ©1995-2018 by The Writing Lab & The OWL at Purdue and Purdue University. All rights reserved. This material may not be published, reproduced, broadcast, rewritten, or redistributed without permission. Use of this site constitutes acceptance of our terms and conditions of fair use.
A literature review is a document or section of a document that collects key sources on a topic and discusses those sources in conversation with each other (also called synthesis ). The lit review is an important genre in many disciplines, not just literature (i.e., the study of works of literature such as novels and plays). When we say “literature review” or refer to “the literature,” we are talking about the research ( scholarship ) in a given field. You will often see the terms “the research,” “the scholarship,” and “the literature” used mostly interchangeably.
Where, when, and why would I write a lit review?
There are a number of different situations where you might write a literature review, each with slightly different expectations; different disciplines, too, have field-specific expectations for what a literature review is and does. For instance, in the humanities, authors might include more overt argumentation and interpretation of source material in their literature reviews, whereas in the sciences, authors are more likely to report study designs and results in their literature reviews; these differences reflect these disciplines’ purposes and conventions in scholarship. You should always look at examples from your own discipline and talk to professors or mentors in your field to be sure you understand your discipline’s conventions, for literature reviews as well as for any other genre.
A literature review can be a part of a research paper or scholarly article, usually falling after the introduction and before the research methods sections. In these cases, the lit review just needs to cover scholarship that is important to the issue you are writing about; sometimes it will also cover key sources that informed your research methodology.
Lit reviews can also be standalone pieces, either as assignments in a class or as publications. In a class, a lit review may be assigned to help students familiarize themselves with a topic and with scholarship in their field, get an idea of the other researchers working on the topic they’re interested in, find gaps in existing research in order to propose new projects, and/or develop a theoretical framework and methodology for later research. As a publication, a lit review usually is meant to help make other scholars’ lives easier by collecting and summarizing, synthesizing, and analyzing existing research on a topic. This can be especially helpful for students or scholars getting into a new research area, or for directing an entire community of scholars toward questions that have not yet been answered.
What are the parts of a lit review?
Most lit reviews use a basic introduction-body-conclusion structure; if your lit review is part of a larger paper, the introduction and conclusion pieces may be just a few sentences while you focus most of your attention on the body. If your lit review is a standalone piece, the introduction and conclusion take up more space and give you a place to discuss your goals, research methods, and conclusions separately from where you discuss the literature itself.
Introduction:
- An introductory paragraph that explains what your working topic and thesis is
- A forecast of key topics or texts that will appear in the review
- Potentially, a description of how you found sources and how you analyzed them for inclusion and discussion in the review (more often found in published, standalone literature reviews than in lit review sections in an article or research paper)
- Summarize and synthesize: Give an overview of the main points of each source and combine them into a coherent whole
- Analyze and interpret: Don’t just paraphrase other researchers – add your own interpretations where possible, discussing the significance of findings in relation to the literature as a whole
- Critically Evaluate: Mention the strengths and weaknesses of your sources
- Write in well-structured paragraphs: Use transition words and topic sentence to draw connections, comparisons, and contrasts.
Conclusion:
- Summarize the key findings you have taken from the literature and emphasize their significance
- Connect it back to your primary research question
How should I organize my lit review?
Lit reviews can take many different organizational patterns depending on what you are trying to accomplish with the review. Here are some examples:
- Chronological : The simplest approach is to trace the development of the topic over time, which helps familiarize the audience with the topic (for instance if you are introducing something that is not commonly known in your field). If you choose this strategy, be careful to avoid simply listing and summarizing sources in order. Try to analyze the patterns, turning points, and key debates that have shaped the direction of the field. Give your interpretation of how and why certain developments occurred (as mentioned previously, this may not be appropriate in your discipline — check with a teacher or mentor if you’re unsure).
- Thematic : If you have found some recurring central themes that you will continue working with throughout your piece, you can organize your literature review into subsections that address different aspects of the topic. For example, if you are reviewing literature about women and religion, key themes can include the role of women in churches and the religious attitude towards women.
- Qualitative versus quantitative research
- Empirical versus theoretical scholarship
- Divide the research by sociological, historical, or cultural sources
- Theoretical : In many humanities articles, the literature review is the foundation for the theoretical framework. You can use it to discuss various theories, models, and definitions of key concepts. You can argue for the relevance of a specific theoretical approach or combine various theorical concepts to create a framework for your research.
What are some strategies or tips I can use while writing my lit review?
Any lit review is only as good as the research it discusses; make sure your sources are well-chosen and your research is thorough. Don’t be afraid to do more research if you discover a new thread as you’re writing. More info on the research process is available in our "Conducting Research" resources .
As you’re doing your research, create an annotated bibliography ( see our page on the this type of document ). Much of the information used in an annotated bibliography can be used also in a literature review, so you’ll be not only partially drafting your lit review as you research, but also developing your sense of the larger conversation going on among scholars, professionals, and any other stakeholders in your topic.
Usually you will need to synthesize research rather than just summarizing it. This means drawing connections between sources to create a picture of the scholarly conversation on a topic over time. Many student writers struggle to synthesize because they feel they don’t have anything to add to the scholars they are citing; here are some strategies to help you:
- It often helps to remember that the point of these kinds of syntheses is to show your readers how you understand your research, to help them read the rest of your paper.
- Writing teachers often say synthesis is like hosting a dinner party: imagine all your sources are together in a room, discussing your topic. What are they saying to each other?
- Look at the in-text citations in each paragraph. Are you citing just one source for each paragraph? This usually indicates summary only. When you have multiple sources cited in a paragraph, you are more likely to be synthesizing them (not always, but often
- Read more about synthesis here.
The most interesting literature reviews are often written as arguments (again, as mentioned at the beginning of the page, this is discipline-specific and doesn’t work for all situations). Often, the literature review is where you can establish your research as filling a particular gap or as relevant in a particular way. You have some chance to do this in your introduction in an article, but the literature review section gives a more extended opportunity to establish the conversation in the way you would like your readers to see it. You can choose the intellectual lineage you would like to be part of and whose definitions matter most to your thinking (mostly humanities-specific, but this goes for sciences as well). In addressing these points, you argue for your place in the conversation, which tends to make the lit review more compelling than a simple reporting of other sources.
- UNC Libraries
- HSL Academic Process
- Systematic Reviews
- Step 6: Assess Quality of Included Studies
Systematic Reviews: Step 6: Assess Quality of Included Studies
Created by health science librarians.
- Step 1: Complete Pre-Review Tasks
- Step 2: Develop a Protocol
- Step 3: Conduct Literature Searches
- Step 4: Manage Citations
- Step 5: Screen Citations
Assess studies for quality and bias
Critically appraise included studies, select a quality assessment tool, a closer look at popular tools, use covidence for quality assessment.
- Quality Assessment FAQs
- Step 7: Extract Data from Included Studies
- Step 8: Write the Review
Check our FAQ's
Email us
Chat with us (during business hours)
Call (919) 962-0800
Make an appointment with a librarian
Request a systematic or scoping review consultation
About Step 6: Assess Quality of Included Studies
In step 6 you will evaluate the articles you included in your review for quality and bias. To do so, you will:
- Use quality assessment tools to grade each article.
- Create a summary of the quality of literature included in your review.
This page has links to quality assessment tools you can use to evaluate different study types. Librarians can help you find widely used tools to evaluate the articles in your review.
Reporting your review with PRISMA
If you reach the quality assessment step and choose to exclude articles for any reason, update the number of included and excluded studies in your PRISMA flow diagram.
Managing your review with Covidence
Covidence includes the Cochrane Risk of Bias 2.0 quality assessment template, but you can also create your own custom quality assessment template.
How a librarian can help with Step 6
- What the quality assessment or risk of bias stage of the review entails
- How to choose an appropriate quality assessment tool
- Best practices for reporting quality assessment results in your review
After the screening process is complete, the systematic review team must assess each article for quality and bias. There are various types of bias, some of which are outlined in the table below from the Cochrane Handbook.
The most important thing to remember when choosing a quality assessment tool is to pick one that was created and validated to assess the study design(s) of your included articles.
For example, if one item in the inclusion criteria of your systematic review is to only include randomized controlled trials (RCTs), then you need to pick a quality assessment tool specifically designed for RCTs (for example, the Cochrane Risk of Bias tool)
Once you have gathered your included studies, you will need to appraise the evidence for its relevance, reliability, validity, and applicability.
Ask questions like:
Relevance: .
- Is the research method/study design appropriate for answering the research question?
- Are specific inclusion / exclusion criteria used?
Reliability:
- Is the effect size practically relevant? How precise is the estimate of the effect? Were confidence intervals given?
Validity:
- Were there enough subjects in the study to establish that the findings did not occur by chance?
- Were subjects randomly allocated? Were the groups comparable? If not, could this have introduced bias?
- Are the measurements/ tools validated by other studies?
- Could there be confounding factors?
Applicability:
- Can the results be applied to my organization and my patient?
What are Quality Assessment tools?
Quality Assessment tools are questionnaires created to help you assess the quality of a variety of study designs. Depending on the types of studies you are analyzing, the questionnaire will be tailored to ask specific questions about the methodology of the study. There are appraisal tools for most kinds of study designs. You should choose a Quality Assessment tool that matches the types of studies you expect to see in your results. If you have multiple types of study designs, you may wish to use several tools from one organization, such as the CASP or LEGEND tools, as they have a range of assessment tools for many study designs.
Click on a study design below to see some examples of quality assessment tools for that type of study.
Randomized Controlled Trials (RCTs)
- Cochrane Risk of Bias (ROB) 2.0 Tool Templates are tailored to randomized parallel-group trials, cluster-randomized parallel-group trails (including stepped-wedge designs), and randomized cross-over trails and other matched designs.
- CASP- Randomized Controlled Trial Appraisal Tool A checklist for RCTs created by the Critical Appraisal Skills Program (CASP)
- The Jadad Scale A scale that assesses the quality of published clinical trials based methods relevant to random assignment, double blinding, and the flow of patients
- CEBM-RCT A critical appraisal tool for RCTs from the Centre for Evidence Based Medicine (CEBM)
- Checklist for Randomized Controlled Trials (JBI) A critical appraisal checklist from the Joanna Briggs Institute (JBI)
- Scottish Intercollegiate Guidelines Network (SIGN) Checklists for quality assessment
- LEGEND Evidence Evaluation Tools A series of critical appraisal tools from the Cincinnati Children's Hospital. Contains tools for a wide variety of study designs, including prospective, retrospective, qualitative, and quantitative designs.
Cohort Studies
- CASP- Cohort Studies A checklist created by the Critical Appraisal Skills Programme (CASP) to assess key criteria relevant to cohort studies
- Checklist for Cohort Studies (JBI) A checklist for cohort studies from the Joanna Briggs Institute
- The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses A validated tool for assessing case-control and cohort studies
- STROBE Checklist A checklist for quality assessment of case-control, cohort, and cross-sectional studies
Case-Control Studies
- CASP- Case Control Study A checklist created by the Critical Appraisal Skills Programme (CASP) to assess key criteria relevant to case-control studies
- Tool to Assess Risk of Bias in Case Control Studies by the CLARITY Group at McMaster University A quality assessment tool for case-control studies from the CLARITY Group at McMaster University
- JBI Checklist for Case-Control Studies A checklist created by the Joanna Briggs Institute
Cross-Sectional Studies
Diagnostic studies.
- CASP- Diagnostic Studies A checklist for diagnostic studies created by the Critical Appraisal Skills Program (CASP)
- QUADAS-2 A quality assessment tool developed by a team at the Bristol Medical School: Population Health Sciences at the University of Bristol
- Critical Appraisal Checklist for Diagnostic Test Accuracy Studies (JBI) A checklist for quality assessment of diagnostic studies developed by the Joanna Briggs Institute
Economic Studies
- Consensus Health Economic Criteria (CHEC) List 19 yes-or-no questions, one for each category to assess economic evaluations
- CASP- Economic Evaluation A checklist for quality assessment of economic studies by the Critical Appraisal Skills Programme
Mixed Methods
- McGill Mixed Methods Appraisal Tool (MMAT) 2018 User Guide See full site for additional information, including FAQ's, references and resources, earlier versions, and more
Qualitative Studies
- CASP- Qualitative Studies 10 questions to help assess qualitative research from the Critical Appraisal Skills Programme
Systematic Reviews and Meta-Analyses
- JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses An 11-item checklist for evaluating systematic reviews
- AMSTAR Checklist A 16-question measurement tool to assess systematic reviews
- AHRQ Methods Guide for Effectiveness and Comparative Effectiveness Reviews A guide to selecting eligibility criteria, searching the literature, extracting data, assessing quality, and completing other steps in the creation of a systematic review
- CASP - Systematic Review A checklist for quality assessment of systematic review from the Critical Appraisal Skills Programme
Clinical Practice Guidelines
- National Guideline Clearinghouse Extent of Adherence to Trustworthy Standards (NEATS) Instrument A 15-item instrument using a scale of 1-5 to evaluate a guideline's adherence to the Institute of Medicine's standard for trust worth guidelines
- AGREE-II Appraisal of Guidelines for Research and Evaluation The Appraisal of Guidelines for Research and Evaluation (AGREE) Instrument evaluates the process of practice guideline development and the quality of reporting
Other Study Designs
- NTACT Quality Checklists Quality indicator checklists for correlational studies, group experimental studies, single case research studies, and qualitative studies developed by the National Technical Assistance Center on Transition (NTACT). (Users must make an account.)
Below, you will find a sample of four popular quality assessment tools and some basic information about each. For more quality assessment tools, please view the blue tabs in the boxes above, organized by study design.
Covidence uses Cochrane Risk of Bias (which is designed for rating RCTs and cannot be used for other study types) as the default tool for quality assessment of included studies. You can opt to manually customize the quality assessment template and use a different tool better suited to your review. More information about quality assessment using Covidence, including how to customize the quality assessment template, can be found below. If you decide to customize the quality assessment template, you cannot switch back to using the Cochrane Risk of Bias template.
More Information
- Quality Assessment on the Covidence Guide
- Covidence FAQs on Quality Assessment Commonly asked questions about quality assessment using Covidence
- Covidence YouTube Channel A collection of Covidence-created videos
- << Previous: Step 5: Screen Citations
- Next: Step 7: Extract Data from Included Studies >>
- Last Updated: Apr 24, 2024 2:00 PM
- URL: https://guides.lib.unc.edu/systematic-reviews
Search & Find
- E-Research by Discipline
- More Search & Find
Places & Spaces
- Places to Study
- Book a Study Room
- Printers, Scanners, & Computers
- More Places & Spaces
- Borrowing & Circulation
- Request a Title for Purchase
- Schedule Instruction Session
- More Services
Support & Guides
- Course Reserves
- Research Guides
- Citing & Writing
- More Support & Guides
- Mission Statement
- Diversity Statement
- Staff Directory
- Job Opportunities
- Give to the Libraries
- News & Exhibits
- Reckoning Initiative
- More About Us
- Search This Site
- Privacy Policy
- Accessibility
- Give Us Your Feedback
- 208 Raleigh Street CB #3916
- Chapel Hill, NC 27515-8890
- 919-962-1053

Literature Reviews
What this handout is about.
This handout will explain what literature reviews are and offer insights into the form and construction of literature reviews in the humanities, social sciences, and sciences.
Introduction
OK. You’ve got to write a literature review. You dust off a novel and a book of poetry, settle down in your chair, and get ready to issue a “thumbs up” or “thumbs down” as you leaf through the pages. “Literature review” done. Right?
Wrong! The “literature” of a literature review refers to any collection of materials on a topic, not necessarily the great literary texts of the world. “Literature” could be anything from a set of government pamphlets on British colonial methods in Africa to scholarly articles on the treatment of a torn ACL. And a review does not necessarily mean that your reader wants you to give your personal opinion on whether or not you liked these sources.
What is a literature review, then?
A literature review discusses published information in a particular subject area, and sometimes information in a particular subject area within a certain time period.
A literature review can be just a simple summary of the sources, but it usually has an organizational pattern and combines both summary and synthesis. A summary is a recap of the important information of the source, but a synthesis is a re-organization, or a reshuffling, of that information. It might give a new interpretation of old material or combine new with old interpretations. Or it might trace the intellectual progression of the field, including major debates. And depending on the situation, the literature review may evaluate the sources and advise the reader on the most pertinent or relevant.
But how is a literature review different from an academic research paper?
The main focus of an academic research paper is to develop a new argument, and a research paper is likely to contain a literature review as one of its parts. In a research paper, you use the literature as a foundation and as support for a new insight that you contribute. The focus of a literature review, however, is to summarize and synthesize the arguments and ideas of others without adding new contributions.
Why do we write literature reviews?
Literature reviews provide you with a handy guide to a particular topic. If you have limited time to conduct research, literature reviews can give you an overview or act as a stepping stone. For professionals, they are useful reports that keep them up to date with what is current in the field. For scholars, the depth and breadth of the literature review emphasizes the credibility of the writer in his or her field. Literature reviews also provide a solid background for a research paper’s investigation. Comprehensive knowledge of the literature of the field is essential to most research papers.
Who writes these things, anyway?
Literature reviews are written occasionally in the humanities, but mostly in the sciences and social sciences; in experiment and lab reports, they constitute a section of the paper. Sometimes a literature review is written as a paper in itself.
Let’s get to it! What should I do before writing the literature review?
If your assignment is not very specific, seek clarification from your instructor:
- Roughly how many sources should you include?
- What types of sources (books, journal articles, websites)?
- Should you summarize, synthesize, or critique your sources by discussing a common theme or issue?
- Should you evaluate your sources?
- Should you provide subheadings and other background information, such as definitions and/or a history?
Find models
Look for other literature reviews in your area of interest or in the discipline and read them to get a sense of the types of themes you might want to look for in your own research or ways to organize your final review. You can simply put the word “review” in your search engine along with your other topic terms to find articles of this type on the Internet or in an electronic database. The bibliography or reference section of sources you’ve already read are also excellent entry points into your own research.
Narrow your topic
There are hundreds or even thousands of articles and books on most areas of study. The narrower your topic, the easier it will be to limit the number of sources you need to read in order to get a good survey of the material. Your instructor will probably not expect you to read everything that’s out there on the topic, but you’ll make your job easier if you first limit your scope.
Keep in mind that UNC Libraries have research guides and to databases relevant to many fields of study. You can reach out to the subject librarian for a consultation: https://library.unc.edu/support/consultations/ .
And don’t forget to tap into your professor’s (or other professors’) knowledge in the field. Ask your professor questions such as: “If you had to read only one book from the 90’s on topic X, what would it be?” Questions such as this help you to find and determine quickly the most seminal pieces in the field.
Consider whether your sources are current
Some disciplines require that you use information that is as current as possible. In the sciences, for instance, treatments for medical problems are constantly changing according to the latest studies. Information even two years old could be obsolete. However, if you are writing a review in the humanities, history, or social sciences, a survey of the history of the literature may be what is needed, because what is important is how perspectives have changed through the years or within a certain time period. Try sorting through some other current bibliographies or literature reviews in the field to get a sense of what your discipline expects. You can also use this method to consider what is currently of interest to scholars in this field and what is not.
Strategies for writing the literature review
Find a focus.
A literature review, like a term paper, is usually organized around ideas, not the sources themselves as an annotated bibliography would be organized. This means that you will not just simply list your sources and go into detail about each one of them, one at a time. No. As you read widely but selectively in your topic area, consider instead what themes or issues connect your sources together. Do they present one or different solutions? Is there an aspect of the field that is missing? How well do they present the material and do they portray it according to an appropriate theory? Do they reveal a trend in the field? A raging debate? Pick one of these themes to focus the organization of your review.
Convey it to your reader
A literature review may not have a traditional thesis statement (one that makes an argument), but you do need to tell readers what to expect. Try writing a simple statement that lets the reader know what is your main organizing principle. Here are a couple of examples:
The current trend in treatment for congestive heart failure combines surgery and medicine. More and more cultural studies scholars are accepting popular media as a subject worthy of academic consideration.
Consider organization
You’ve got a focus, and you’ve stated it clearly and directly. Now what is the most effective way of presenting the information? What are the most important topics, subtopics, etc., that your review needs to include? And in what order should you present them? Develop an organization for your review at both a global and local level:
First, cover the basic categories
Just like most academic papers, literature reviews also must contain at least three basic elements: an introduction or background information section; the body of the review containing the discussion of sources; and, finally, a conclusion and/or recommendations section to end the paper. The following provides a brief description of the content of each:
- Introduction: Gives a quick idea of the topic of the literature review, such as the central theme or organizational pattern.
- Body: Contains your discussion of sources and is organized either chronologically, thematically, or methodologically (see below for more information on each).
- Conclusions/Recommendations: Discuss what you have drawn from reviewing literature so far. Where might the discussion proceed?
Organizing the body
Once you have the basic categories in place, then you must consider how you will present the sources themselves within the body of your paper. Create an organizational method to focus this section even further.
To help you come up with an overall organizational framework for your review, consider the following scenario:
You’ve decided to focus your literature review on materials dealing with sperm whales. This is because you’ve just finished reading Moby Dick, and you wonder if that whale’s portrayal is really real. You start with some articles about the physiology of sperm whales in biology journals written in the 1980’s. But these articles refer to some British biological studies performed on whales in the early 18th century. So you check those out. Then you look up a book written in 1968 with information on how sperm whales have been portrayed in other forms of art, such as in Alaskan poetry, in French painting, or on whale bone, as the whale hunters in the late 19th century used to do. This makes you wonder about American whaling methods during the time portrayed in Moby Dick, so you find some academic articles published in the last five years on how accurately Herman Melville portrayed the whaling scene in his novel.
Now consider some typical ways of organizing the sources into a review:
- Chronological: If your review follows the chronological method, you could write about the materials above according to when they were published. For instance, first you would talk about the British biological studies of the 18th century, then about Moby Dick, published in 1851, then the book on sperm whales in other art (1968), and finally the biology articles (1980s) and the recent articles on American whaling of the 19th century. But there is relatively no continuity among subjects here. And notice that even though the sources on sperm whales in other art and on American whaling are written recently, they are about other subjects/objects that were created much earlier. Thus, the review loses its chronological focus.
- By publication: Order your sources by publication chronology, then, only if the order demonstrates a more important trend. For instance, you could order a review of literature on biological studies of sperm whales if the progression revealed a change in dissection practices of the researchers who wrote and/or conducted the studies.
- By trend: A better way to organize the above sources chronologically is to examine the sources under another trend, such as the history of whaling. Then your review would have subsections according to eras within this period. For instance, the review might examine whaling from pre-1600-1699, 1700-1799, and 1800-1899. Under this method, you would combine the recent studies on American whaling in the 19th century with Moby Dick itself in the 1800-1899 category, even though the authors wrote a century apart.
- Thematic: Thematic reviews of literature are organized around a topic or issue, rather than the progression of time. However, progression of time may still be an important factor in a thematic review. For instance, the sperm whale review could focus on the development of the harpoon for whale hunting. While the study focuses on one topic, harpoon technology, it will still be organized chronologically. The only difference here between a “chronological” and a “thematic” approach is what is emphasized the most: the development of the harpoon or the harpoon technology.But more authentic thematic reviews tend to break away from chronological order. For instance, a thematic review of material on sperm whales might examine how they are portrayed as “evil” in cultural documents. The subsections might include how they are personified, how their proportions are exaggerated, and their behaviors misunderstood. A review organized in this manner would shift between time periods within each section according to the point made.
- Methodological: A methodological approach differs from the two above in that the focusing factor usually does not have to do with the content of the material. Instead, it focuses on the “methods” of the researcher or writer. For the sperm whale project, one methodological approach would be to look at cultural differences between the portrayal of whales in American, British, and French art work. Or the review might focus on the economic impact of whaling on a community. A methodological scope will influence either the types of documents in the review or the way in which these documents are discussed. Once you’ve decided on the organizational method for the body of the review, the sections you need to include in the paper should be easy to figure out. They should arise out of your organizational strategy. In other words, a chronological review would have subsections for each vital time period. A thematic review would have subtopics based upon factors that relate to the theme or issue.
Sometimes, though, you might need to add additional sections that are necessary for your study, but do not fit in the organizational strategy of the body. What other sections you include in the body is up to you. Put in only what is necessary. Here are a few other sections you might want to consider:
- Current Situation: Information necessary to understand the topic or focus of the literature review.
- History: The chronological progression of the field, the literature, or an idea that is necessary to understand the literature review, if the body of the literature review is not already a chronology.
- Methods and/or Standards: The criteria you used to select the sources in your literature review or the way in which you present your information. For instance, you might explain that your review includes only peer-reviewed articles and journals.
Questions for Further Research: What questions about the field has the review sparked? How will you further your research as a result of the review?
Begin composing
Once you’ve settled on a general pattern of organization, you’re ready to write each section. There are a few guidelines you should follow during the writing stage as well. Here is a sample paragraph from a literature review about sexism and language to illuminate the following discussion:
However, other studies have shown that even gender-neutral antecedents are more likely to produce masculine images than feminine ones (Gastil, 1990). Hamilton (1988) asked students to complete sentences that required them to fill in pronouns that agreed with gender-neutral antecedents such as “writer,” “pedestrian,” and “persons.” The students were asked to describe any image they had when writing the sentence. Hamilton found that people imagined 3.3 men to each woman in the masculine “generic” condition and 1.5 men per woman in the unbiased condition. Thus, while ambient sexism accounted for some of the masculine bias, sexist language amplified the effect. (Source: Erika Falk and Jordan Mills, “Why Sexist Language Affects Persuasion: The Role of Homophily, Intended Audience, and Offense,” Women and Language19:2).
Use evidence
In the example above, the writers refer to several other sources when making their point. A literature review in this sense is just like any other academic research paper. Your interpretation of the available sources must be backed up with evidence to show that what you are saying is valid.
Be selective
Select only the most important points in each source to highlight in the review. The type of information you choose to mention should relate directly to the review’s focus, whether it is thematic, methodological, or chronological.
Use quotes sparingly
Falk and Mills do not use any direct quotes. That is because the survey nature of the literature review does not allow for in-depth discussion or detailed quotes from the text. Some short quotes here and there are okay, though, if you want to emphasize a point, or if what the author said just cannot be rewritten in your own words. Notice that Falk and Mills do quote certain terms that were coined by the author, not common knowledge, or taken directly from the study. But if you find yourself wanting to put in more quotes, check with your instructor.
Summarize and synthesize
Remember to summarize and synthesize your sources within each paragraph as well as throughout the review. The authors here recapitulate important features of Hamilton’s study, but then synthesize it by rephrasing the study’s significance and relating it to their own work.
Keep your own voice
While the literature review presents others’ ideas, your voice (the writer’s) should remain front and center. Notice that Falk and Mills weave references to other sources into their own text, but they still maintain their own voice by starting and ending the paragraph with their own ideas and their own words. The sources support what Falk and Mills are saying.
Use caution when paraphrasing
When paraphrasing a source that is not your own, be sure to represent the author’s information or opinions accurately and in your own words. In the preceding example, Falk and Mills either directly refer in the text to the author of their source, such as Hamilton, or they provide ample notation in the text when the ideas they are mentioning are not their own, for example, Gastil’s. For more information, please see our handout on plagiarism .
Revise, revise, revise
Draft in hand? Now you’re ready to revise. Spending a lot of time revising is a wise idea, because your main objective is to present the material, not the argument. So check over your review again to make sure it follows the assignment and/or your outline. Then, just as you would for most other academic forms of writing, rewrite or rework the language of your review so that you’ve presented your information in the most concise manner possible. Be sure to use terminology familiar to your audience; get rid of unnecessary jargon or slang. Finally, double check that you’ve documented your sources and formatted the review appropriately for your discipline. For tips on the revising and editing process, see our handout on revising drafts .
Works consulted
We consulted these works while writing this handout. This is not a comprehensive list of resources on the handout’s topic, and we encourage you to do your own research to find additional publications. Please do not use this list as a model for the format of your own reference list, as it may not match the citation style you are using. For guidance on formatting citations, please see the UNC Libraries citation tutorial . We revise these tips periodically and welcome feedback.
Anson, Chris M., and Robert A. Schwegler. 2010. The Longman Handbook for Writers and Readers , 6th ed. New York: Longman.
Jones, Robert, Patrick Bizzaro, and Cynthia Selfe. 1997. The Harcourt Brace Guide to Writing in the Disciplines . New York: Harcourt Brace.
Lamb, Sandra E. 1998. How to Write It: A Complete Guide to Everything You’ll Ever Write . Berkeley: Ten Speed Press.
Rosen, Leonard J., and Laurence Behrens. 2003. The Allyn & Bacon Handbook , 5th ed. New York: Longman.
Troyka, Lynn Quittman, and Doug Hesse. 2016. Simon and Schuster Handbook for Writers , 11th ed. London: Pearson.
You may reproduce it for non-commercial use if you use the entire handout and attribute the source: The Writing Center, University of North Carolina at Chapel Hill
Make a Gift

- Harvard Library
- Research Guides
- Harvard Graduate School of Design - Frances Loeb Library
Write and Cite
- Literature Review
- Academic Integrity
- Citing Sources
- Fair Use, Permissions, and Copyright
- Writing Resources
- Grants and Fellowships
- Last Updated: Apr 30, 2024 4:28 PM
- URL: https://guides.library.harvard.edu/gsd/write
Harvard University Digital Accessibility Policy
A systematic literature review on the health-related quality of life and economic burden of Fabry disease
Affiliations.
- 1 The Mark Holland Metabolic Unit, Northern Care Alliance NHS Foundation Trust, Salford, UK.
- 2 Centre for Cardiovascular Science, Queen's Medical Research Institute, University of Edinburgh, Edinburgh, UK.
- 3 Takeda Development Center Americas, Cambridge, MA, USA.
- 4 Parexel, Mohali, India.
- 5 Takeda UK Ltd, London, UK.
- 6 Takeda Development Center Americas, Cambridge, MA, USA. [email protected].
- PMID: 38689282
- DOI: 10.1186/s13023-024-03131-y
Background: Fabry disease (FD) is a rare lysosomal storage disease associated with glycolipid accumulation that impacts multiple physiological systems. We conducted a systematic literature review (SLR) to characterize the humanistic (quality of life [QoL]) and economic burden of FD.
Methods: Searches were conducted in the Embase, MEDLINE ® , and MEDLINE ® In-Process databases from inception to January 19, 2022. Conference abstracts of specified congresses were manually searched. Additional searches were performed in the Cochrane and ProQuest databases for the humanistic SLR and the National Health Service Economic Evaluations Database for the economic SLR. Studies of patients with FD of any sex, race, and age, and published in the English language were included. There was no restriction on intervention or comparator. For the humanistic SLR, studies that reported utility data, database/registry-based studies, questionnaires/surveys, and cohort studies were included. For the economic SLR, studies reporting economic evaluations or assessing the cost of illness and resource use were included.
Results: Of the 1363 records identified in the humanistic search, 36 studies were included. The most commonly used QoL assessments were the 36-item Short-Form Health Survey (n = 16), EQ-5D questionnaire descriptive system or visual analog scale (n = 9), and the Brief Pain Inventory (n = 8). Reduced QoL was reported in patients with FD compared with healthy populations across multiple domains, including pain, physical functioning, and depressive symptoms. Multiple variables-including sex, age, disease severity, and treatment status-impacted QoL. Of the 711 records identified in the economic burden search, 18 studies were included. FD was associated with high cost and healthcare resource use. Contributors to the cost burden included enzyme replacement therapy, healthcare, and social care. In the seven studies that reported health utility values, lower utility scores were generally associated with more complications (including cardiac, renal, and cerebrovascular morbidities) and with classical disease in males.
Conclusion: FD remains associated with a high cost and healthcare resource use burden, and reduced QoL compared with healthy populations. Integrating information from QoL and economic assessments may help to identify interventions that are likely to be of most value to patients with FD.
Keywords: Agalsidase alfa; Agalsidase beta; Cost burden; EQ-5D; Fabry disease; Health state utility values; Health-related quality of life; Lysosomal storage disease; Migalastat; Resource utilization; SF-36.
© 2024. The Author(s).
Publication types
- Systematic Review
- Research Support, Non-U.S. Gov't
- Cost of Illness*
- Fabry Disease* / economics
- Quality of Life*
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 33, Issue 5
- Equitable and accessible informed healthcare consent process for people with intellectual disability: a systematic literature review
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0002-8498-7329 Manjekah Dunn 1 , 2 ,
- Iva Strnadová 3 , 4 , 5 ,
- Jackie Leach Scully 4 ,
- Jennifer Hansen 3 ,
- Julie Loblinzk 3 , 5 ,
- Skie Sarfaraz 5 ,
- Chloe Molnar 1 ,
- Elizabeth Emma Palmer 1 , 2
- 1 Faculty of Medicine & Health , University of New South Wales , Sydney , New South Wales , Australia
- 2 The Sydney Children's Hospitals Network , Sydney , New South Wales , Australia
- 3 School of Education , University of New South Wales , Sydney , New South Wales , Australia
- 4 Disability Innovation Institute , University of New South Wales , Sydney , New South Wales , Australia
- 5 Self Advocacy Sydney , Sydney , New South Wales , Australia
- Correspondence to Dr Manjekah Dunn, Paediatrics & Child Health, University of New South Wales Medicine & Health, Sydney, New South Wales, Australia; manjekah.dunn{at}unsw.edu.au
Objective To identify factors acting as barriers or enablers to the process of healthcare consent for people with intellectual disability and to understand how to make this process equitable and accessible.
Data sources Databases: Embase, MEDLINE, PsychINFO, PubMed, SCOPUS, Web of Science and CINAHL. Additional articles were obtained from an ancestral search and hand-searching three journals.
Eligibility criteria Peer-reviewed original research about the consent process for healthcare interventions, published after 1990, involving adult participants with intellectual disability.
Synthesis of results Inductive thematic analysis was used to identify factors affecting informed consent. The findings were reviewed by co-researchers with intellectual disability to ensure they reflected lived experiences, and an easy read summary was created.
Results Twenty-three studies were included (1999 to 2020), with a mix of qualitative (n=14), quantitative (n=6) and mixed-methods (n=3) studies. Participant numbers ranged from 9 to 604 people (median 21) and included people with intellectual disability, health professionals, carers and support people, and others working with people with intellectual disability. Six themes were identified: (1) health professionals’ attitudes and lack of education, (2) inadequate accessible health information, (3) involvement of support people, (4) systemic constraints, (5) person-centred informed consent and (6) effective communication between health professionals and patients. Themes were barriers (themes 1, 2 and 4), enablers (themes 5 and 6) or both (theme 3).
Conclusions Multiple reasons contribute to poor consent practices for people with intellectual disability in current health systems. Recommendations include addressing health professionals’ attitudes and lack of education in informed consent with clinician training, the co-production of accessible information resources and further inclusive research into informed consent for people with intellectual disability.
PROSPERO registration CRD42021290548.
- Decision making
- Healthcare quality improvement
- Patient-centred care
- Quality improvement
- Standards of care
Data availability statement
Data are available upon reasonable request. Additional data and materials such as data collection forms, data extraction and analysis templates and QualSyst assessment data can be obtained by contacting the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bmjqs-2023-016113
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
What is already known on this topic
People with intellectual disability are frequently excluded from decision-making processes and not provided equal opportunity for informed consent, despite protections outlined in the United Nations Convention on the Rights of Persons with Disabilities.
People with intellectual disability have the capacity and desire to make informed medical decisions, which can improve their well-being, health satisfaction and health outcomes.
What this review study adds
Health professionals lack adequate training in valid informed consent and making reasonable adjustments for people with intellectual disability, and continue to perpetuate assumptions of incapacity.
Health information provided to people with intellectual disability is often inaccessible and insufficient for them to make informed decisions about healthcare.
The role of support people, systemic constraints, a person-centred approach and ineffective healthcare communication also affect informed consent.
How this review might affect research, practice or policy
Health professionals need additional training on how to provide a valid informed consent process for people with intellectual disability, specifically in using accessible health information, making reasonable adjustments (e.g., longer/multiple appointments, options of a support person attending or not, using plain English), involving the individual in discussions, and communicating effectively with them.
Inclusive research is needed to hear the voices and opinions of people with intellectual disability about healthcare decision-making and about informed consent practices in specific healthcare settings.
Introduction
Approximately 1% of the world’s population have intellectual disability. 1 Intellectual disability is medically defined as a group of neurodevelopmental conditions beginning in childhood, with below average cognitive functioning and adaptive behaviour, including limitations in conceptual, social and practical skills. 2 People with intellectual disability prefer an alternative strength-based definition, reflected in the comment by Robert Strike OAM (Order of Australia Medal): ‘We can learn if the way of teaching matches how the person learns’, 3 reinforcing the importance of providing information tailored to the needs of a person with intellectual disability. A diagnosis of intellectual disability is associated with significant disparities in health outcomes. 4–7 Person-centred decision-making and better communication have been shown to improve patient satisfaction, 8 9 the physician–patient relationship 10 and overall health outcomes 11 for the wider population. Ensuring people with intellectual disability experience informed decision-making and accessible healthcare can help address the ongoing health disparities and facilitate equal access to healthcare.
Bodily autonomy is an individual’s power and agency to make decisions about their own body. 12 Informed consent for healthcare enables a person to practice bodily autonomy and is protected, for example, by the National Safety and Quality Health Service Standards (Australia), 13 Mental Capacity Act (UK) 14 and the Joint Commission Standards (USA). 15 In this article, we define informed consent according to three requirements: (1) the person is provided with information they understand, (2) the decision is free of coercion and (3) the person must have capacity. 16 For informed consent to be valid, this process must be suited to the individual’s needs so that they can understand and communicate effectively. Capacity is the ability to give informed consent for a medical intervention, 17 18 and the Mental Capacity Act outlines that ‘a person must be assumed to have capacity unless it is established that he lacks capacity’ and that incapacity can only be established if ‘all practicable steps’ to support capacity have been attempted without success. 14 These assumptions of capacity are also decision-specific, meaning an individual’s ability to consent can change depending on the situation, the choice itself and other factors. 17
Systemic issues with healthcare delivery systems have resulted in access barriers for people with intellectual disability, 19 despite the disability discrimination legislation in many countries who are signatories to the United Nations (UN) Convention on the Rights of Persons with Disabilities. 20 Patients with intellectual disability are not provided the reasonable adjustments that would enable them to give informed consent for medical procedures or interventions, 21 22 despite evidence that many people with intellectual disability have both the capacity and the desire to make their own healthcare decisions. 21 23
To support people with intellectual disability to make independent health decisions, an equitable and accessible informed consent process is needed. 24 However, current health systems have consistently failed to provide this. 21 25 To address this gap, we must first understand the factors that contribute to inequitable and inaccessible consent. To the best of our knowledge, the only current review of informed consent for people with intellectual disability is an integrative review by Goldsmith et al . 26 Many of the included articles focused on assessment of capacity 27–29 and research consent. 30–32 The review’s conclusion supported the functional approach to assess capacity, with minimal focus on how the informed consent processes can be improved. More recently, there has been a move towards ensuring that the consent process is accessible for all individuals, including elderly patients 33 and people with aphasia. 34 However, there remains a paucity of literature about the informed consent process for people with intellectual disability, with no systematic reviews summarising the factors influencing the healthcare consent process for people with intellectual disability.
To identify barriers to and enablers of the informed healthcare consent process for people with intellectual disability, and to understand how this can be made equitable and accessible.
A systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) systematic literature review protocol. 35 The PRISMA 2020 checklist 36 and ENhancing Transparency in REporting the synthesis of Qualitative research (ENTREQ) reporting guidelines were also followed. 37 The full study protocol is included in online supplemental appendix 1 .
Supplemental material
No patients or members of the public were involved in this research for this manuscript.
Search strategy
A search strategy was developed to identify articles about intellectual disability, consent and healthcare interventions, described in online supplemental appendix 2 . Multiple databases were searched for articles published between January 1990 to January 2022 (Embase, MEDLINE, PsychINFO, PubMed, SCOPUS, Web of Science and CINAHL). These databases include healthcare and psychology databases that best capture relevant literature on this topic, including medical, nursing, social sciences and bioethical literature. The search was limited to studies published from 1990 as understandings of consent have changed since then. 38 39 This yielded 4853 unique papers which were imported into Covidence, a specialised programme for conducting systematic reviews. 40
Study selection
Citation screening by abstract and titles was completed by two independent researchers (MD and EEP). Included articles had to:
Examine the informed consent process for a healthcare intervention for people with intellectual disability.
Have collected more than 50% of its data from relevant stakeholders, including adults with intellectual disability, families or carers of a person with intellectual disability, and professionals who engage with people with intellectual disability.
Report empirical data from primary research methodology.
Be published in a peer-reviewed journal after January 1990.
Be available in English.
Full text screening was completed by two independent researchers (MD and EEP). Articles were excluded if consent was only briefly discussed or if it focused on consent for research, capacity assessment, or participant knowledge or comprehension. Any conflicts were resolved through discussion with an independent third researcher (IS).
Additional studies were identified through an ancestral search and by hand-searching three major journals relevant to intellectual disability research. Journals were selected if they had published more than one included article for this review or in previous literature reviews conducted by the research team.
Quality assessment
Two independent researchers (MD and IS) assessed study quality with the QualSyst tool, 41 which can assess both qualitative and quantitative research papers. After evaluating the distribution of scores, a threshold value of 55% was used, as suggested by QualSyst 41 to exclude poor-quality studies but capture enough studies overall. Any conflicts between the quality assessment scores were resolved by a third researcher (EEP). For mixed-method studies, both qualitative and quantitative quality scores were calculated, and the higher value used.
Data collection
Two independent researchers (MD and JH) reviewed each study and extracted relevant details, including study size, participant demographics, year, country of publication, study design, data analysis and major outcomes reported. Researchers used standardised data collection forms designed, with input from senior researchers with expertise in qualitative research (IS and EEP), to extract data relevant to the review’s research aims. The form was piloted on one study, and a second iteration made based on feedback. These forms captured data on study design, methods, participants, any factors affecting the process of informed consent and study limitations. Data included descriptions and paragraphs outlining key findings, the healthcare context, verbatim participant quotes and any quantitative analyses or statistics. Missing or unclear data were noted.
Data analysis
A pilot literature search showed significant heterogeneity in methodology of studies, limiting the applicability of traditional quantitative analysis (ie, meta-analysis). Instead, inductive thematic analysis was chosen as an alternative methodology 42 43 that has been used in recent systematic reviews examining barriers and enablers of other health processes. 44 45 The six-phase approach described by Braun and Clarke was used. 46 47 A researcher (MD) independently coded the extracted data of each study line-by-line, with subsequent data grouped into pre-existing codes or new concepts when necessary. Codes were reviewed iteratively and grouped into categories, subthemes and themes framed around the research question. Another independent researcher (JH) collated and analysed the data on study demographics, methods and limitations. The themes were reviewed by two senior researchers (EEP and IS).
Qualitative methods of effect size calculations have been described in the literature, 48 49 which was captured in this review by the number of studies that identified each subtheme, with an assigned frequency rating to compare their relative significance. Subthemes were given a frequency rating of A, B, C or D if they were identified by >10, 7–9, 4–6 or <3 articles, respectively. The overall significance of each theme was estimated by the number of studies that mentioned it and the GRADE framework, a stepwise approach to quality assessment using a four-tier rating system. Each study was evaluated for risk of bias, inconsistency, indirectness, imprecision and publication bias. 50 51 Study sensitivity was assessed by counting the number of distinct subthemes included. 52 The quality of findings was designated high, moderate or low depending on the frequency ratings, the QualSyst score and the GRADE scores of studies supporting the finding. Finally, the relative contributions of each study were evaluated by the number of subthemes described, guided by previously reported methods for qualitative reviews. 52
Co-research
The findings were reviewed by two co-researchers with intellectual disability (JL and SS), with over 30 years combined experience as members and employees of a self-advocacy organisation. Guidance on the findings and an easy read summary was produced in line with best-practice inclusive research 53 54 over multiple discussions. Input from two health professional researchers (MD and EEP) provided data triangulation and sense-checking of findings.
Twenty-three articles were identified ( figure 1 ): 14 qualitative, 6 quantitative and 3 mixed-methods. Two papers included the same population of study participants: McCarthy 55 and McCarthy, 56 but had different research questions. Fovargue et al 57 was excluded due to a quality score of 35%. Common quality limitations were a lack of verification procedures to establish credibility and limited researcher reflexivity. No studies were excluded due to language requirements (as all were in English) or age restrictions (all studies had majority adult participants).
- Download figure
- Open in new tab
- Download powerpoint
PRISMA 2020 flowchart for the systematic review. 36
Studies were published from 1999 to 2020 and involved participant populations from the UK (n=18), USA (n=3), Sweden (n=1) and Ireland (n=1). Participant numbers ranged from 9 to 604 (median 21), and participants included people with intellectual disability (n=817), health professionals (n=272), carers and support people (n=48), and other professionals that work with people with intellectual disability (n=137, community service agency directors, social workers, administrative staff and care home staff). Ages of participants ranged from 8 to 84 years, though only Aman et al 58 included participants <18 years of age. This study was included as the article states very few children were included. Studies examined consent in different contexts, including contraception and sexual health (6/23 articles), 58–60 medications (5/23 articles), 58–62 emergency healthcare, 63 cervical screening, 64 community referrals, 58–61 65 mental health, 66 hydrotherapy, 64 blood collection 67 and broad decision-making consent without a specific context. 65 68–71 A detailed breakdown of each study is included in online supplemental appendix 3 .
Six major themes were identified from the studies, summarised in figure 2 . An overview of included studies showing study sensitivity, effect size, QualSyst and GRADE scores is given in online supplemental appendix 4 . Studies with higher QualSyst and GRADE scores contributed more to this review’s findings and tended to include more subthemes; specifically, Rogers et al , 66 Sowney and Barr, 63 Höglund and Larsson, 72 and McCarthy 55 and McCarthy. 56 Figure 3 gives the easy read version of theme 1, with the full easy read summary in online supplemental appendix 5 .
Summary of the identified six themes and subthemes.
Theme 1 of the easy read summary.
Theme 1—Health professionals’ attitudes and lack of education about informed consent
Health professionals’ attitudes and practices were frequently (18/21) identified as factors affecting the informed consent process, with substantial evidence supporting this theme. Studies noted the lack of training for health professionals in supporting informed consent for people with intellectual disability, their desire for further education, and stereotypes and discrimination perpetuated by health professionals.
Lack of health professional education on informed consent and disability discrimination legislation
Multiple studies reported inconsistent informed consent practices, for various reasons: some reported that health professionals ‘forgot’ to or ‘did not realise consent was necessary’, 63 73 but inconsistent consent practices were also attributed to healthcare providers’ unfamiliarity with consent guidelines and poor education on this topic. Carlson et al 73 reported that only 44% of general practitioners (GPs) were aware of consent guidelines, and there was the misconception that consent was unnecessary for people with intellectual disability. Similarly, studies of psychologists 66 and nurses 63 found that many were unfamiliar with their obligations to obtain consent, despite the existence of anti-discrimination legislation. People with intellectual disability describe feeling discriminated against by health professionals, reflected in comments such as ‘I can tell, my doctor just thinks I’m stupid – I'm nothing to him’. 74 Poor consent practices by health professionals were observed in Goldsmith et al , 67 while health professionals surveyed by McCarthy 56 were unaware of their responsibility to provide accessible health information to women with intellectual disability. Improving health professional education and training was suggested by multiple studies as a way to remove this barrier. 63 65–67 69 73
Lack of training on best practices for health professions caring for people with intellectual disability
A lack of training in caring for and communicating with people with intellectual disability was also described by midwives, 72 psychologists, 66 nurses, 63 pharmacists 61 and GPs. 56 72 75 Health professionals lacked knowledge about best practice approaches to providing equitable healthcare consent processes through reasonable adjustments such as accessible health information, 56 60 66 longer appointments times, 60 72 simple English 62 67 and flexible approaches to patient needs. 63 72
Health professionals’ stereotyping and assumptions of incapacity
Underlying stereotypes contributed to some health professionals’ (including nurses, 63 GPs 56 and physiotherapists 64 ) belief that people with intellectual disability lack capacity and therefore, do not require opportunities for informed consent. 56 64 In a survey of professionals referring people with intellectual disability to a disability service, the second most common reason for not obtaining consent was ‘patient unable to understand’. 73
Proxy consent as an inappropriate alternative
People with intellectual disability are rarely the final decision-maker in their medical choices, with many health providers seeking proxy consent from carers, support workers and family members, despite its legal invalidity. In McCarthy’s study (2010), 18/23 women with intellectual disability said the decision to start contraception was made by someone else. Many GPs appeared unaware that proxy consent is invalid in the UK. 56 Similar reports came from people with intellectual disability, 55 56 60 64 69 76 health professionals (nurses, doctors, allied health, psychologists), 56 63 64 66 77 support people 64 77 and non-medical professionals, 65 73 and capacity was rarely documented. 56 62 77
Exclusion of people with intellectual disability from decision-making discussions
Studies described instances where health professionals made decisions for their patients with intellectual disability or coerced patients into a choice. 55 72 74 76 77 In Ledger et al 77 , only 62% of women with intellectual disability were involved in the discussion about contraception, and only 38% made the final decision, and others stated in Wiseman and Ferrie 74 : ‘I was not given the opportunity to explore the different options. I was told what one I should take’. Three papers outlined instances where the choices of people with intellectual disability were ignored despite possessing capacity 65 66 69 and when a procedure continued despite them withdrawing consent. 69
Theme 2—Inadequate accessible health information
Lack of accessible health information.
The lack of accessible health information was the most frequently identified subtheme (16/23 studies). Some studies reported that health professionals provided information to carers instead, 60 avoided providing easy read information due to concerns about ‘offending’ patients 75 or only provided verbal information. 56 67 Informed consent was supported when health professionals recognised the importance of providing medical information 64 and when it was provided in an accessible format. 60 Alternative approaches to health information were explored, including virtual reality 68 and in-person education sessions, 59 with varying results. Overall, the need to provide information in different formats tailored to an individual’s communication needs, rather than a ‘one size fits all’ approach, was emphasised by both people with intellectual disability 60 and health professionals. 66
Insufficient information provided
Studies described situations where insufficient information was provided to people with intellectual disability to make informed decisions. For example, some people felt the information from their GP was often too basic to be helpful (Fish et al 60 ) and wanted additional information on consent forms (Rose et al 78 ).
Theme 3—The involvement of support people
Support people (including carers, family members and group home staff) were identified in 11 articles as both enablers of and barriers to informed consent. The antagonistic nature of these findings and lower frequency of subthemes are reflected in the lower quality assessments of evidence.
Support people facilitated communication with health professionals
Some studies reported carers bridging communication barriers with health to support informed consent. 63 64 McCarthy 56 found 21/23 of women with intellectual disability preferred to see doctors with a support person due to perceived benefits: ‘Sometimes I don’t understand it, so they have to explain it to my carer, so they can explain it to me easier’. Most GPs in this study (93%) also agreed that support people aided communication.
Support people helped people with intellectual disability make decisions
By advocating for people with intellectual disability, carers encouraged decision-making, 64 74 provided health information, 74 77 emotional support 76 and assisted with reading or remembering health information. 55 58 76 Some people with intellectual disability explicitly appreciated their support person’s involvement, 60 such as in McCarthy’s 55 study where 18/23 participants felt supported and safer when a support person was involved.
Support people impeded individual autonomy
The study by Wiseman and Ferrie 74 found that while younger participants with intellectual disability felt family members empowered their decision-making, older women felt family members impaired their ability to give informed consent. This was reflected in interviews with carers who questioned the capacity of the person with intellectual disability they supported and stated they would guide them to pick the ‘best choice’ or even over-ride their choices. 64 Studies of psychologists and community service directors described instances where the decision of family or carers was prioritised over the wishes of the person with intellectual disability. 65 66 Some women with intellectual disability in McCarthy’s studies (2010, 2009) 55 56 appeared to have been coerced into using contraception by parental pressures or fear of losing group home support.
Theme 4—Systemic constraints within healthcare systems
Time restraints affect informed consent and accessible healthcare.
Resource limitations create time constraints that impair the consent process and have been identified as a barrier by psychologists, 66 GPs, 56 hospital nurses 63 and community disability workers. 73 Rogers et al 66 highlighted that a personalised approach that could improve informed decision-making is restricted by inflexible medical models. Only two studies described flexible patient-centred approaches to consent. 60 72 A survey of primary care practices in 2007 reported that most did not modify their cervical screening information for patients with intellectual disability because it was not practical. 75
Inflexible models of consent
Both people with intellectual disability 76 and health professionals 66 recognised that consent is traditionally obtained through one-off interactions prior to an intervention. Yet, for people with intellectual disability, consent should ideally be an ongoing process that begins before an appointment and continues between subsequent ones. Other studies have tended to describe one-off interactions where decision-making was not revisited at subsequent appointments. 56 60 72 76
Lack of systemic supports
In one survey, self-advocates highlighted a lack of information on medication for people with intellectual disability and suggested a telephone helpline and a centralised source of information to support consent. 60 Health professionals also want greater systemic support, such as a health professional specialised in intellectual disability care to support other staff, 72 or a pharmacist specifically to help patients with intellectual disability. 61 Studies highlighted a lack of guidelines about healthcare needs of people with intellectual disabilities such as contraceptive counselling 72 or primary care. 75
Theme 5—Person-centred informed consent
Ten studies identified factors related to a person-centred approach to informed consent, grouped below into three subthemes. Health professionals should tailor their practice when obtaining informed consent from people with intellectual disability by considering how these subthemes relate to the individual. Each subtheme was described five times in the literature with a relative frequency rating of ‘C’, contributing to overall lower quality scores.
Previous experience with decision-making
Arscott et al 71 found that the ability of people with intellectual disability to consent changed with their verbal and memory skills and in different clinical vignettes, supporting the view of ‘functional’ capacity specific to the context of the medical decision. Although previous experiences with decision-making did not influence informed consent in this paper, other studies suggest that people with intellectual disability accustomed to independent decision-making were more able to make informed medical decisions, 66 70 and those who live independently were more likely to make independent healthcare decisions. 56 Health professionals should be aware that their patients with intellectual disability will have variable experience with decision-making and provide individualised support to meet their needs.
Variable awareness about healthcare rights
Consent processes should be tailored to the health literacy of patients, including emphasising available choices and the option to refuse treatment. In some studies, medical decisions were not presented to people with intellectual disability as a choice, 64 and people with intellectual disability were not informed of their legal right to accessible health information. 56
Power differences and acquiescence
Acquiescence by people with intellectual disability due to common and repeated experiences of trauma—that is, their tendency to agree with suggestions made by carers and health professionals, often to avoid upsetting others—was identified as an ongoing barrier. In McCarthy’s (2009) interviews with women with intellectual disability, some participants implicitly rejected the idea that they might make their own healthcare decisions: ‘They’re the carers, they have responsibility for me’. Others appeared to have made decisions to appease their carers: ‘I have the jab (contraceptive injection) so I can’t be blamed for getting pregnant’. 55 Two studies highlighted that health professionals need to be mindful of power imbalances when discussing consent with people with intellectual disability to ensure the choices are truly autonomous. 61 66
Theme 6—Effective communication between health professionals and patients
Implementation of reasonable adjustments for verbal and written information.
Simple language was always preferred by people with intellectual disability. 60 67 Other communication aids used in decision-making included repetition, short sentences, models, pictures and easy read brochures. 72 Another reasonable adjustment is providing the opportunity to ask questions, which women with intellectual disability in McCarthy’s (2009) study reported did not occur. 55
Tailored communication methods including non-verbal communication
Midwives noted that continuity of care allows them to develop rapport and understand the communication preferences of people with intellectual disability. 72 This is not always possible; for emergency nurses, the lack of background information about patients with intellectual disability made it challenging to understand their communication preferences. 63 The use of non-verbal communication, such as body language, was noted as underutilised 62 66 and people with intellectual disability supported the use of hearing loops, braille and sign language. 60
To the best of our knowledge, this is the first systematic review investigating the barriers and enablers of the informed consent process for healthcare procedures for people with intellectual disability. The integrative review by Goldsmith et al 26 examined capacity assessment and shares only three articles with this systematic review. 69 71 73 Since the 2000s, there has been a paradigm shift in which capacity is no longer considered a fixed ability that only some individuals possess 38 39 but instead as ‘functional’: a flexible ability that changes over time and in different contexts, 79 reflected in Goldsmith’s review. An individual’s capacity can be supported through various measures, including how information is communicated and how the decision-making process is approached. 18 80 By recognising the barriers and enablers identified in this review, physicians can help ensure the consent process for their patients with intellectual disability is both valid and truly informed. This review has highlighted the problems of inaccessible health information, insufficient clinical education on how to make reasonable adjustments and lack of person-centred trauma-informed care.
Recommendations
Health professionals require training in the informed consent process for people with intellectual disability, particularly in effective and respectful communication, reasonable adjustments and trauma-informed care. Reasonable adjustments include offering longer or multiple appointments, using accessible resources (such as easy read information or shared decision-making tools) and allowing patient choices (such as to record a consultation or involve a support person). Co-researchers reported that many people with intellectual disability prefer to go without a support person because they find it difficult to challenge their decisions and feel ignored if the health professional only talks to the support person. People with intellectual disability also feel they cannot seek second opinions before making medical decisions or feel pressured to provide consent, raising the possibility of coercion. These experiences contribute to healthcare trauma. Co-researchers raised the importance of building rapport with the person with intellectual disability and of making reasonable adjustments, such as actively advocating for the person’s autonomy, clearly stating all options including the choice to refuse treatment, providing opportunities to contribute to discussions and multiple appointments to ask questions and understand information. They felt that without these efforts to support consent, health professionals can reinforce traumatic healthcare experiences for people with intellectual disability. Co-researchers noted instances where choices were made by doctors without discussion and where they were only given a choice after requesting one and expressed concern that these barriers are greater for those with higher support needs.
Co-researchers showed how these experiences contributed to mistrust of health professionals and poorer health outcomes. In one situation, a co-researcher was not informed of a medication’s withdrawal effects, resulting in significant side-effects when it was ceased. Many people with intellectual disability describe a poor relationship with their health professionals, finding it difficult to trust health information provided due to previous traumatic experiences of disrespect, coercion, lack of choice and inadequate support. Many feel they cannot speak up due to the power imbalance and fear of retaliation. Poor consent practices and lack of reasonable adjustments directly harm therapeutic alliances by reducing trust, contribute to healthcare trauma and lead to poorer health outcomes for people with intellectual disability.
Additional education and training for health professionals is urgently needed in the areas of informed consent, reasonable adjustments and effective communication with people with intellectual disability. The experiences of health professionals within the research team confirmed that there is limited training in providing high-quality healthcare for people with intellectual disability, including reasonable adjustments and accessible health information. Co-researchers also suggested that education should be provided to carers and support people to help them better advocate for people with intellectual disability.
Health information should be provided in a multimodal format, including written easy read information. Many countries have regulation protecting the right to accessible health information and communication support to make an informed choice, such as UK’s Accessible Information Standard, 81 and Australia’s Charter of Health Care Rights, 24 yet these are rarely observed. Steps to facilitate this include routinely asking patients about information requirements, system alerts for an individual’s needs or routinely providing reasonable adjustments. 82 Co-researchers agreed that there is a lack of accessible health information, particularly about medications, and that diagrams and illustrations are underutilised. There is a critical need for more inclusive and accessible resources to help health professionals support informed consent in a safe and high-quality health system. These resources should be created through methods of inclusive research, such as co-production, actively involving people with intellectual disability in the planning, creation, and feedback process. 53
Strengths and limitations
This systematic review involved two co-researchers with intellectual disability in sense-checking findings and co-creating the easy read summary. Two co-authors who are health professionals provided additional sense-checking of findings from a different stakeholder perspective. In future research, this could be extended by involving people with intellectual disability in the design and planning of the study as per recommendations for best-practice inclusive research. 53 83
The current literature is limited by low use of inclusive research practices in research involving people with intellectual disability, increasing vulnerability to external biases (eg, inaccessible questionnaires, involvement of carers in data collection, overcompliance or acquiescence and absence of researcher reflexivity). Advisory groups or co-research with people with intellectual disability were only used in five studies. 58 60 68 74 76 Other limitations include unclear selection criteria, low sample sizes, missing data, using gatekeepers in patient selection and predominance of UK-based studies—increasing the risk of bias and reducing transferability. Nine studies (out of 15 involving people with intellectual disability) explicitly excluded those with severe or profound intellectual disability, reflecting a selection bias; only one study specifically focused on people with intellectual disability with higher support needs. Studies were limited to a few healthcare contexts, with a focus on consent about sexual health, contraception and medications.
The heterogeneity and qualitative nature of studies made it challenging to apply traditional meta-analysis. However, to promote consistency in qualitative research, the PRISMA and ENTREQ guidelines were followed. 36 37 Although no meta-analyses occurred, the duplication of study populations in McCarthy 2009 and 2010 likely contributed to increased significance of findings reported in both studies. Most included studies (13/23) were published over 10 years ago, reducing the current relevance of this review’s findings. Nonetheless, the major findings reflect underlying systemic issues within the health system, which are unlikely to have been resolved since the articles were published, as the just-released final report of the Australian Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability highlights. 84 There is an urgent need for more inclusive studies to explore the recommendations and preferences of people with intellectual disability about healthcare choices.
Informed consent processes for people with intellectual disability should include accessible information and reasonable adjustments, be tailored to individuals’ needs and comply with consent and disability legislation. Resources, guidelines and healthcare education are needed and should cover how to involve carers and support people, address systemic healthcare problems, promote a person-centred approach and ensure effective communication. These resources and future research must use principles of inclusive co-production—involving people with intellectual disability at all stages. Additionally, research is needed on people with higher support needs and in specific contexts where informed consent is vital but under-researched, such as cancer screening, palliative care, prenatal and newborn screening, surgical procedures, genetic medicine and advanced therapeutics such as gene-based therapies.
Ethics statements
Patient consent for publication.
Not applicable.
Ethics approval
- Maulik PK ,
- Mascarenhas MN ,
- Mathers CD , et al
- World Health Organisation
- Council for Intellectual Disability
- Emerson E ,
- Shogren KA ,
- Wehmeyer ML ,
- Reese RM , et al
- Cordasco KM
- Hallock JL ,
- Jordens CFC ,
- McGrath C , et al
- Brenner LH ,
- Brenner AT ,
- United Nations Population Fund
- Australian Commission on Safety and Quality in Health Care
- The Joint Commission
- Beauchamp TL ,
- Childress JF
- New South Wales Attorney General
- United Nations General Assembly
- Strnadová I ,
- Loblinzk J ,
- Scully JL , et al
- MacPhail C ,
- McKay K , et al
- Keywood K ,
- Fovargue S ,
- Goldsmith L ,
- Skirton H ,
- Cash J , et al
- Morris CD ,
- Niederbuhl JM ,
- Arscott K ,
- Fisher CB ,
- Davidson PW , et al
- Giampieri M
- Shamseer L ,
- Clarke M , et al
- McKenzie JE ,
- Bossuyt PM , et al
- Flemming K ,
- McInnes E , et al
- Appelbaum PS
- ↵ Covidence systematic review software . Melbourne, Australia ,
- Proudfoot K
- Papadopoulos I ,
- Koulouglioti C ,
- Lazzarino R , et al
- Onwuegbuzie AJ
- BMJ Best Practice
- Guyatt GH ,
- Vist GE , et al
- Garcia-Lee B
- Brimblecombe J , et al
- Benson BA ,
- Farmer CA , et al
- Ferguson L ,
- Graham YNH ,
- Gerrard D ,
- Laight S , et al
- Huneke NTM ,
- Halder N , et al
- Ferguson M ,
- Jarrett D ,
- McGuire BE , et al
- Woodward V ,
- Jackson L , et al
- Conboy-Hill S ,
- Leafman J ,
- Nehrenz GM , et al
- Höglund B ,
- Carlson T ,
- English S , et al
- Wiseman P ,
- Walmsley J ,
- Tilley E , et al
- Khatkar HS , et al
- Holland AJ , et al
- Beauchamp TL
- England National Health Service
- National Health Service England
- Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability
Supplementary materials
Supplementary data.
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
- Data supplement 2
- Data supplement 3
- Data supplement 4
- Data supplement 5
Contributors MD, EEP and IS conceived the idea for the systematic review. MD drafted the search strategy which was refined by EEP and IS. MD and EEP completed article screening. MD and IS completed quality assessments of included articles. MD and JH completed data extraction. MD drafted the original manuscript. JL and SS were co-researchers who sense-checked findings and were consulted to formulate dissemination plans. JL and SS co-produced the easy read summary with MD, CM, JH, EEP and IS. MD, JLS, EEP and IS reviewed manuscript wording. All authors critically reviewed the manuscript and approved it for publication. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. MD is the guarantor responsible for the overall content of this manuscript.
Funding This systematic literature review was funded by the National Health & Medical Research Council (NHMRC), Targeted Call for Research (TCR) into Improving health of people with intellectual disability. Research grant title "GeneEQUAL: equitable and accessible genomic healthcare for people with intellectual disability". NHMRC application ID: 2022/GNT2015753.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Editorial It is up to healthcare professionals to talk to us in a way that we can understand: informed consent processes in people with an intellectual disability Jonathon Ding Richard Keagan-Bull Irene Tuffrey-Wijne BMJ Quality & Safety 2024; 33 277-279 Published Online First: 30 Jan 2024. doi: 10.1136/bmjqs-2023-016830
Read the full text or download the PDF:
Artificial intelligence for Quality of Life study: A Systematic Literature Review
Ieee account.
- Change Username/Password
- Update Address
Purchase Details
- Payment Options
- Order History
- View Purchased Documents
Profile Information
- Communications Preferences
- Profession and Education
- Technical Interests
- US & Canada: +1 800 678 4333
- Worldwide: +1 732 981 0060
- Contact & Support
- About IEEE Xplore
- Accessibility
- Terms of Use
- Nondiscrimination Policy
- Privacy & Opting Out of Cookies
A not-for-profit organization, IEEE is the world's largest technical professional organization dedicated to advancing technology for the benefit of humanity. © Copyright 2024 IEEE - All rights reserved. Use of this web site signifies your agreement to the terms and conditions.

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Lau F, Kuziemsky C, editors. Handbook of eHealth Evaluation: An Evidence-based Approach [Internet]. Victoria (BC): University of Victoria; 2017 Feb 27.

Handbook of eHealth Evaluation: An Evidence-based Approach [Internet].
Chapter 9 methods for literature reviews.
Guy Paré and Spyros Kitsiou .
9.1. Introduction
Literature reviews play a critical role in scholarship because science remains, first and foremost, a cumulative endeavour ( vom Brocke et al., 2009 ). As in any academic discipline, rigorous knowledge syntheses are becoming indispensable in keeping up with an exponentially growing eHealth literature, assisting practitioners, academics, and graduate students in finding, evaluating, and synthesizing the contents of many empirical and conceptual papers. Among other methods, literature reviews are essential for: (a) identifying what has been written on a subject or topic; (b) determining the extent to which a specific research area reveals any interpretable trends or patterns; (c) aggregating empirical findings related to a narrow research question to support evidence-based practice; (d) generating new frameworks and theories; and (e) identifying topics or questions requiring more investigation ( Paré, Trudel, Jaana, & Kitsiou, 2015 ).
Literature reviews can take two major forms. The most prevalent one is the “literature review” or “background” section within a journal paper or a chapter in a graduate thesis. This section synthesizes the extant literature and usually identifies the gaps in knowledge that the empirical study addresses ( Sylvester, Tate, & Johnstone, 2013 ). It may also provide a theoretical foundation for the proposed study, substantiate the presence of the research problem, justify the research as one that contributes something new to the cumulated knowledge, or validate the methods and approaches for the proposed study ( Hart, 1998 ; Levy & Ellis, 2006 ).
The second form of literature review, which is the focus of this chapter, constitutes an original and valuable work of research in and of itself ( Paré et al., 2015 ). Rather than providing a base for a researcher’s own work, it creates a solid starting point for all members of the community interested in a particular area or topic ( Mulrow, 1987 ). The so-called “review article” is a journal-length paper which has an overarching purpose to synthesize the literature in a field, without collecting or analyzing any primary data ( Green, Johnson, & Adams, 2006 ).
When appropriately conducted, review articles represent powerful information sources for practitioners looking for state-of-the art evidence to guide their decision-making and work practices ( Paré et al., 2015 ). Further, high-quality reviews become frequently cited pieces of work which researchers seek out as a first clear outline of the literature when undertaking empirical studies ( Cooper, 1988 ; Rowe, 2014 ). Scholars who track and gauge the impact of articles have found that review papers are cited and downloaded more often than any other type of published article ( Cronin, Ryan, & Coughlan, 2008 ; Montori, Wilczynski, Morgan, Haynes, & Hedges, 2003 ; Patsopoulos, Analatos, & Ioannidis, 2005 ). The reason for their popularity may be the fact that reading the review enables one to have an overview, if not a detailed knowledge of the area in question, as well as references to the most useful primary sources ( Cronin et al., 2008 ). Although they are not easy to conduct, the commitment to complete a review article provides a tremendous service to one’s academic community ( Paré et al., 2015 ; Petticrew & Roberts, 2006 ). Most, if not all, peer-reviewed journals in the fields of medical informatics publish review articles of some type.
The main objectives of this chapter are fourfold: (a) to provide an overview of the major steps and activities involved in conducting a stand-alone literature review; (b) to describe and contrast the different types of review articles that can contribute to the eHealth knowledge base; (c) to illustrate each review type with one or two examples from the eHealth literature; and (d) to provide a series of recommendations for prospective authors of review articles in this domain.
9.2. Overview of the Literature Review Process and Steps
As explained in Templier and Paré (2015) , there are six generic steps involved in conducting a review article:
- formulating the research question(s) and objective(s),
- searching the extant literature,
- screening for inclusion,
- assessing the quality of primary studies,
- extracting data, and
- analyzing data.
Although these steps are presented here in sequential order, one must keep in mind that the review process can be iterative and that many activities can be initiated during the planning stage and later refined during subsequent phases ( Finfgeld-Connett & Johnson, 2013 ; Kitchenham & Charters, 2007 ).
Formulating the research question(s) and objective(s): As a first step, members of the review team must appropriately justify the need for the review itself ( Petticrew & Roberts, 2006 ), identify the review’s main objective(s) ( Okoli & Schabram, 2010 ), and define the concepts or variables at the heart of their synthesis ( Cooper & Hedges, 2009 ; Webster & Watson, 2002 ). Importantly, they also need to articulate the research question(s) they propose to investigate ( Kitchenham & Charters, 2007 ). In this regard, we concur with Jesson, Matheson, and Lacey (2011) that clearly articulated research questions are key ingredients that guide the entire review methodology; they underscore the type of information that is needed, inform the search for and selection of relevant literature, and guide or orient the subsequent analysis. Searching the extant literature: The next step consists of searching the literature and making decisions about the suitability of material to be considered in the review ( Cooper, 1988 ). There exist three main coverage strategies. First, exhaustive coverage means an effort is made to be as comprehensive as possible in order to ensure that all relevant studies, published and unpublished, are included in the review and, thus, conclusions are based on this all-inclusive knowledge base. The second type of coverage consists of presenting materials that are representative of most other works in a given field or area. Often authors who adopt this strategy will search for relevant articles in a small number of top-tier journals in a field ( Paré et al., 2015 ). In the third strategy, the review team concentrates on prior works that have been central or pivotal to a particular topic. This may include empirical studies or conceptual papers that initiated a line of investigation, changed how problems or questions were framed, introduced new methods or concepts, or engendered important debate ( Cooper, 1988 ). Screening for inclusion: The following step consists of evaluating the applicability of the material identified in the preceding step ( Levy & Ellis, 2006 ; vom Brocke et al., 2009 ). Once a group of potential studies has been identified, members of the review team must screen them to determine their relevance ( Petticrew & Roberts, 2006 ). A set of predetermined rules provides a basis for including or excluding certain studies. This exercise requires a significant investment on the part of researchers, who must ensure enhanced objectivity and avoid biases or mistakes. As discussed later in this chapter, for certain types of reviews there must be at least two independent reviewers involved in the screening process and a procedure to resolve disagreements must also be in place ( Liberati et al., 2009 ; Shea et al., 2009 ). Assessing the quality of primary studies: In addition to screening material for inclusion, members of the review team may need to assess the scientific quality of the selected studies, that is, appraise the rigour of the research design and methods. Such formal assessment, which is usually conducted independently by at least two coders, helps members of the review team refine which studies to include in the final sample, determine whether or not the differences in quality may affect their conclusions, or guide how they analyze the data and interpret the findings ( Petticrew & Roberts, 2006 ). Ascribing quality scores to each primary study or considering through domain-based evaluations which study components have or have not been designed and executed appropriately makes it possible to reflect on the extent to which the selected study addresses possible biases and maximizes validity ( Shea et al., 2009 ). Extracting data: The following step involves gathering or extracting applicable information from each primary study included in the sample and deciding what is relevant to the problem of interest ( Cooper & Hedges, 2009 ). Indeed, the type of data that should be recorded mainly depends on the initial research questions ( Okoli & Schabram, 2010 ). However, important information may also be gathered about how, when, where and by whom the primary study was conducted, the research design and methods, or qualitative/quantitative results ( Cooper & Hedges, 2009 ). Analyzing and synthesizing data : As a final step, members of the review team must collate, summarize, aggregate, organize, and compare the evidence extracted from the included studies. The extracted data must be presented in a meaningful way that suggests a new contribution to the extant literature ( Jesson et al., 2011 ). Webster and Watson (2002) warn researchers that literature reviews should be much more than lists of papers and should provide a coherent lens to make sense of extant knowledge on a given topic. There exist several methods and techniques for synthesizing quantitative (e.g., frequency analysis, meta-analysis) and qualitative (e.g., grounded theory, narrative analysis, meta-ethnography) evidence ( Dixon-Woods, Agarwal, Jones, Young, & Sutton, 2005 ; Thomas & Harden, 2008 ).
9.3. Types of Review Articles and Brief Illustrations
EHealth researchers have at their disposal a number of approaches and methods for making sense out of existing literature, all with the purpose of casting current research findings into historical contexts or explaining contradictions that might exist among a set of primary research studies conducted on a particular topic. Our classification scheme is largely inspired from Paré and colleagues’ (2015) typology. Below we present and illustrate those review types that we feel are central to the growth and development of the eHealth domain.
9.3.1. Narrative Reviews
The narrative review is the “traditional” way of reviewing the extant literature and is skewed towards a qualitative interpretation of prior knowledge ( Sylvester et al., 2013 ). Put simply, a narrative review attempts to summarize or synthesize what has been written on a particular topic but does not seek generalization or cumulative knowledge from what is reviewed ( Davies, 2000 ; Green et al., 2006 ). Instead, the review team often undertakes the task of accumulating and synthesizing the literature to demonstrate the value of a particular point of view ( Baumeister & Leary, 1997 ). As such, reviewers may selectively ignore or limit the attention paid to certain studies in order to make a point. In this rather unsystematic approach, the selection of information from primary articles is subjective, lacks explicit criteria for inclusion and can lead to biased interpretations or inferences ( Green et al., 2006 ). There are several narrative reviews in the particular eHealth domain, as in all fields, which follow such an unstructured approach ( Silva et al., 2015 ; Paul et al., 2015 ).
Despite these criticisms, this type of review can be very useful in gathering together a volume of literature in a specific subject area and synthesizing it. As mentioned above, its primary purpose is to provide the reader with a comprehensive background for understanding current knowledge and highlighting the significance of new research ( Cronin et al., 2008 ). Faculty like to use narrative reviews in the classroom because they are often more up to date than textbooks, provide a single source for students to reference, and expose students to peer-reviewed literature ( Green et al., 2006 ). For researchers, narrative reviews can inspire research ideas by identifying gaps or inconsistencies in a body of knowledge, thus helping researchers to determine research questions or formulate hypotheses. Importantly, narrative reviews can also be used as educational articles to bring practitioners up to date with certain topics of issues ( Green et al., 2006 ).
Recently, there have been several efforts to introduce more rigour in narrative reviews that will elucidate common pitfalls and bring changes into their publication standards. Information systems researchers, among others, have contributed to advancing knowledge on how to structure a “traditional” review. For instance, Levy and Ellis (2006) proposed a generic framework for conducting such reviews. Their model follows the systematic data processing approach comprised of three steps, namely: (a) literature search and screening; (b) data extraction and analysis; and (c) writing the literature review. They provide detailed and very helpful instructions on how to conduct each step of the review process. As another methodological contribution, vom Brocke et al. (2009) offered a series of guidelines for conducting literature reviews, with a particular focus on how to search and extract the relevant body of knowledge. Last, Bandara, Miskon, and Fielt (2011) proposed a structured, predefined and tool-supported method to identify primary studies within a feasible scope, extract relevant content from identified articles, synthesize and analyze the findings, and effectively write and present the results of the literature review. We highly recommend that prospective authors of narrative reviews consult these useful sources before embarking on their work.
Darlow and Wen (2015) provide a good example of a highly structured narrative review in the eHealth field. These authors synthesized published articles that describe the development process of mobile health ( m-health ) interventions for patients’ cancer care self-management. As in most narrative reviews, the scope of the research questions being investigated is broad: (a) how development of these systems are carried out; (b) which methods are used to investigate these systems; and (c) what conclusions can be drawn as a result of the development of these systems. To provide clear answers to these questions, a literature search was conducted on six electronic databases and Google Scholar . The search was performed using several terms and free text words, combining them in an appropriate manner. Four inclusion and three exclusion criteria were utilized during the screening process. Both authors independently reviewed each of the identified articles to determine eligibility and extract study information. A flow diagram shows the number of studies identified, screened, and included or excluded at each stage of study selection. In terms of contributions, this review provides a series of practical recommendations for m-health intervention development.
9.3.2. Descriptive or Mapping Reviews
The primary goal of a descriptive review is to determine the extent to which a body of knowledge in a particular research topic reveals any interpretable pattern or trend with respect to pre-existing propositions, theories, methodologies or findings ( King & He, 2005 ; Paré et al., 2015 ). In contrast with narrative reviews, descriptive reviews follow a systematic and transparent procedure, including searching, screening and classifying studies ( Petersen, Vakkalanka, & Kuzniarz, 2015 ). Indeed, structured search methods are used to form a representative sample of a larger group of published works ( Paré et al., 2015 ). Further, authors of descriptive reviews extract from each study certain characteristics of interest, such as publication year, research methods, data collection techniques, and direction or strength of research outcomes (e.g., positive, negative, or non-significant) in the form of frequency analysis to produce quantitative results ( Sylvester et al., 2013 ). In essence, each study included in a descriptive review is treated as the unit of analysis and the published literature as a whole provides a database from which the authors attempt to identify any interpretable trends or draw overall conclusions about the merits of existing conceptualizations, propositions, methods or findings ( Paré et al., 2015 ). In doing so, a descriptive review may claim that its findings represent the state of the art in a particular domain ( King & He, 2005 ).
In the fields of health sciences and medical informatics, reviews that focus on examining the range, nature and evolution of a topic area are described by Anderson, Allen, Peckham, and Goodwin (2008) as mapping reviews . Like descriptive reviews, the research questions are generic and usually relate to publication patterns and trends. There is no preconceived plan to systematically review all of the literature although this can be done. Instead, researchers often present studies that are representative of most works published in a particular area and they consider a specific time frame to be mapped.
An example of this approach in the eHealth domain is offered by DeShazo, Lavallie, and Wolf (2009). The purpose of this descriptive or mapping review was to characterize publication trends in the medical informatics literature over a 20-year period (1987 to 2006). To achieve this ambitious objective, the authors performed a bibliometric analysis of medical informatics citations indexed in medline using publication trends, journal frequencies, impact factors, Medical Subject Headings (MeSH) term frequencies, and characteristics of citations. Findings revealed that there were over 77,000 medical informatics articles published during the covered period in numerous journals and that the average annual growth rate was 12%. The MeSH term analysis also suggested a strong interdisciplinary trend. Finally, average impact scores increased over time with two notable growth periods. Overall, patterns in research outputs that seem to characterize the historic trends and current components of the field of medical informatics suggest it may be a maturing discipline (DeShazo et al., 2009).
9.3.3. Scoping Reviews
Scoping reviews attempt to provide an initial indication of the potential size and nature of the extant literature on an emergent topic (Arksey & O’Malley, 2005; Daudt, van Mossel, & Scott, 2013 ; Levac, Colquhoun, & O’Brien, 2010). A scoping review may be conducted to examine the extent, range and nature of research activities in a particular area, determine the value of undertaking a full systematic review (discussed next), or identify research gaps in the extant literature ( Paré et al., 2015 ). In line with their main objective, scoping reviews usually conclude with the presentation of a detailed research agenda for future works along with potential implications for both practice and research.
Unlike narrative and descriptive reviews, the whole point of scoping the field is to be as comprehensive as possible, including grey literature (Arksey & O’Malley, 2005). Inclusion and exclusion criteria must be established to help researchers eliminate studies that are not aligned with the research questions. It is also recommended that at least two independent coders review abstracts yielded from the search strategy and then the full articles for study selection ( Daudt et al., 2013 ). The synthesized evidence from content or thematic analysis is relatively easy to present in tabular form (Arksey & O’Malley, 2005; Thomas & Harden, 2008 ).
One of the most highly cited scoping reviews in the eHealth domain was published by Archer, Fevrier-Thomas, Lokker, McKibbon, and Straus (2011) . These authors reviewed the existing literature on personal health record ( phr ) systems including design, functionality, implementation, applications, outcomes, and benefits. Seven databases were searched from 1985 to March 2010. Several search terms relating to phr s were used during this process. Two authors independently screened titles and abstracts to determine inclusion status. A second screen of full-text articles, again by two independent members of the research team, ensured that the studies described phr s. All in all, 130 articles met the criteria and their data were extracted manually into a database. The authors concluded that although there is a large amount of survey, observational, cohort/panel, and anecdotal evidence of phr benefits and satisfaction for patients, more research is needed to evaluate the results of phr implementations. Their in-depth analysis of the literature signalled that there is little solid evidence from randomized controlled trials or other studies through the use of phr s. Hence, they suggested that more research is needed that addresses the current lack of understanding of optimal functionality and usability of these systems, and how they can play a beneficial role in supporting patient self-management ( Archer et al., 2011 ).
9.3.4. Forms of Aggregative Reviews
Healthcare providers, practitioners, and policy-makers are nowadays overwhelmed with large volumes of information, including research-based evidence from numerous clinical trials and evaluation studies, assessing the effectiveness of health information technologies and interventions ( Ammenwerth & de Keizer, 2004 ; Deshazo et al., 2009 ). It is unrealistic to expect that all these disparate actors will have the time, skills, and necessary resources to identify the available evidence in the area of their expertise and consider it when making decisions. Systematic reviews that involve the rigorous application of scientific strategies aimed at limiting subjectivity and bias (i.e., systematic and random errors) can respond to this challenge.
Systematic reviews attempt to aggregate, appraise, and synthesize in a single source all empirical evidence that meet a set of previously specified eligibility criteria in order to answer a clearly formulated and often narrow research question on a particular topic of interest to support evidence-based practice ( Liberati et al., 2009 ). They adhere closely to explicit scientific principles ( Liberati et al., 2009 ) and rigorous methodological guidelines (Higgins & Green, 2008) aimed at reducing random and systematic errors that can lead to deviations from the truth in results or inferences. The use of explicit methods allows systematic reviews to aggregate a large body of research evidence, assess whether effects or relationships are in the same direction and of the same general magnitude, explain possible inconsistencies between study results, and determine the strength of the overall evidence for every outcome of interest based on the quality of included studies and the general consistency among them ( Cook, Mulrow, & Haynes, 1997 ). The main procedures of a systematic review involve:
- Formulating a review question and developing a search strategy based on explicit inclusion criteria for the identification of eligible studies (usually described in the context of a detailed review protocol).
- Searching for eligible studies using multiple databases and information sources, including grey literature sources, without any language restrictions.
- Selecting studies, extracting data, and assessing risk of bias in a duplicate manner using two independent reviewers to avoid random or systematic errors in the process.
- Analyzing data using quantitative or qualitative methods.
- Presenting results in summary of findings tables.
- Interpreting results and drawing conclusions.
Many systematic reviews, but not all, use statistical methods to combine the results of independent studies into a single quantitative estimate or summary effect size. Known as meta-analyses , these reviews use specific data extraction and statistical techniques (e.g., network, frequentist, or Bayesian meta-analyses) to calculate from each study by outcome of interest an effect size along with a confidence interval that reflects the degree of uncertainty behind the point estimate of effect ( Borenstein, Hedges, Higgins, & Rothstein, 2009 ; Deeks, Higgins, & Altman, 2008 ). Subsequently, they use fixed or random-effects analysis models to combine the results of the included studies, assess statistical heterogeneity, and calculate a weighted average of the effect estimates from the different studies, taking into account their sample sizes. The summary effect size is a value that reflects the average magnitude of the intervention effect for a particular outcome of interest or, more generally, the strength of a relationship between two variables across all studies included in the systematic review. By statistically combining data from multiple studies, meta-analyses can create more precise and reliable estimates of intervention effects than those derived from individual studies alone, when these are examined independently as discrete sources of information.
The review by Gurol-Urganci, de Jongh, Vodopivec-Jamsek, Atun, and Car (2013) on the effects of mobile phone messaging reminders for attendance at healthcare appointments is an illustrative example of a high-quality systematic review with meta-analysis. Missed appointments are a major cause of inefficiency in healthcare delivery with substantial monetary costs to health systems. These authors sought to assess whether mobile phone-based appointment reminders delivered through Short Message Service ( sms ) or Multimedia Messaging Service ( mms ) are effective in improving rates of patient attendance and reducing overall costs. To this end, they conducted a comprehensive search on multiple databases using highly sensitive search strategies without language or publication-type restrictions to identify all rct s that are eligible for inclusion. In order to minimize the risk of omitting eligible studies not captured by the original search, they supplemented all electronic searches with manual screening of trial registers and references contained in the included studies. Study selection, data extraction, and risk of bias assessments were performed independently by two coders using standardized methods to ensure consistency and to eliminate potential errors. Findings from eight rct s involving 6,615 participants were pooled into meta-analyses to calculate the magnitude of effects that mobile text message reminders have on the rate of attendance at healthcare appointments compared to no reminders and phone call reminders.
Meta-analyses are regarded as powerful tools for deriving meaningful conclusions. However, there are situations in which it is neither reasonable nor appropriate to pool studies together using meta-analytic methods simply because there is extensive clinical heterogeneity between the included studies or variation in measurement tools, comparisons, or outcomes of interest. In these cases, systematic reviews can use qualitative synthesis methods such as vote counting, content analysis, classification schemes and tabulations, as an alternative approach to narratively synthesize the results of the independent studies included in the review. This form of review is known as qualitative systematic review.
A rigorous example of one such review in the eHealth domain is presented by Mickan, Atherton, Roberts, Heneghan, and Tilson (2014) on the use of handheld computers by healthcare professionals and their impact on access to information and clinical decision-making. In line with the methodological guidelines for systematic reviews, these authors: (a) developed and registered with prospero ( www.crd.york.ac.uk/ prospero / ) an a priori review protocol; (b) conducted comprehensive searches for eligible studies using multiple databases and other supplementary strategies (e.g., forward searches); and (c) subsequently carried out study selection, data extraction, and risk of bias assessments in a duplicate manner to eliminate potential errors in the review process. Heterogeneity between the included studies in terms of reported outcomes and measures precluded the use of meta-analytic methods. To this end, the authors resorted to using narrative analysis and synthesis to describe the effectiveness of handheld computers on accessing information for clinical knowledge, adherence to safety and clinical quality guidelines, and diagnostic decision-making.
In recent years, the number of systematic reviews in the field of health informatics has increased considerably. Systematic reviews with discordant findings can cause great confusion and make it difficult for decision-makers to interpret the review-level evidence ( Moher, 2013 ). Therefore, there is a growing need for appraisal and synthesis of prior systematic reviews to ensure that decision-making is constantly informed by the best available accumulated evidence. Umbrella reviews , also known as overviews of systematic reviews, are tertiary types of evidence synthesis that aim to accomplish this; that is, they aim to compare and contrast findings from multiple systematic reviews and meta-analyses ( Becker & Oxman, 2008 ). Umbrella reviews generally adhere to the same principles and rigorous methodological guidelines used in systematic reviews. However, the unit of analysis in umbrella reviews is the systematic review rather than the primary study ( Becker & Oxman, 2008 ). Unlike systematic reviews that have a narrow focus of inquiry, umbrella reviews focus on broader research topics for which there are several potential interventions ( Smith, Devane, Begley, & Clarke, 2011 ). A recent umbrella review on the effects of home telemonitoring interventions for patients with heart failure critically appraised, compared, and synthesized evidence from 15 systematic reviews to investigate which types of home telemonitoring technologies and forms of interventions are more effective in reducing mortality and hospital admissions ( Kitsiou, Paré, & Jaana, 2015 ).
9.3.5. Realist Reviews
Realist reviews are theory-driven interpretative reviews developed to inform, enhance, or supplement conventional systematic reviews by making sense of heterogeneous evidence about complex interventions applied in diverse contexts in a way that informs policy decision-making ( Greenhalgh, Wong, Westhorp, & Pawson, 2011 ). They originated from criticisms of positivist systematic reviews which centre on their “simplistic” underlying assumptions ( Oates, 2011 ). As explained above, systematic reviews seek to identify causation. Such logic is appropriate for fields like medicine and education where findings of randomized controlled trials can be aggregated to see whether a new treatment or intervention does improve outcomes. However, many argue that it is not possible to establish such direct causal links between interventions and outcomes in fields such as social policy, management, and information systems where for any intervention there is unlikely to be a regular or consistent outcome ( Oates, 2011 ; Pawson, 2006 ; Rousseau, Manning, & Denyer, 2008 ).
To circumvent these limitations, Pawson, Greenhalgh, Harvey, and Walshe (2005) have proposed a new approach for synthesizing knowledge that seeks to unpack the mechanism of how “complex interventions” work in particular contexts. The basic research question — what works? — which is usually associated with systematic reviews changes to: what is it about this intervention that works, for whom, in what circumstances, in what respects and why? Realist reviews have no particular preference for either quantitative or qualitative evidence. As a theory-building approach, a realist review usually starts by articulating likely underlying mechanisms and then scrutinizes available evidence to find out whether and where these mechanisms are applicable ( Shepperd et al., 2009 ). Primary studies found in the extant literature are viewed as case studies which can test and modify the initial theories ( Rousseau et al., 2008 ).
The main objective pursued in the realist review conducted by Otte-Trojel, de Bont, Rundall, and van de Klundert (2014) was to examine how patient portals contribute to health service delivery and patient outcomes. The specific goals were to investigate how outcomes are produced and, most importantly, how variations in outcomes can be explained. The research team started with an exploratory review of background documents and research studies to identify ways in which patient portals may contribute to health service delivery and patient outcomes. The authors identified six main ways which represent “educated guesses” to be tested against the data in the evaluation studies. These studies were identified through a formal and systematic search in four databases between 2003 and 2013. Two members of the research team selected the articles using a pre-established list of inclusion and exclusion criteria and following a two-step procedure. The authors then extracted data from the selected articles and created several tables, one for each outcome category. They organized information to bring forward those mechanisms where patient portals contribute to outcomes and the variation in outcomes across different contexts.
9.3.6. Critical Reviews
Lastly, critical reviews aim to provide a critical evaluation and interpretive analysis of existing literature on a particular topic of interest to reveal strengths, weaknesses, contradictions, controversies, inconsistencies, and/or other important issues with respect to theories, hypotheses, research methods or results ( Baumeister & Leary, 1997 ; Kirkevold, 1997 ). Unlike other review types, critical reviews attempt to take a reflective account of the research that has been done in a particular area of interest, and assess its credibility by using appraisal instruments or critical interpretive methods. In this way, critical reviews attempt to constructively inform other scholars about the weaknesses of prior research and strengthen knowledge development by giving focus and direction to studies for further improvement ( Kirkevold, 1997 ).
Kitsiou, Paré, and Jaana (2013) provide an example of a critical review that assessed the methodological quality of prior systematic reviews of home telemonitoring studies for chronic patients. The authors conducted a comprehensive search on multiple databases to identify eligible reviews and subsequently used a validated instrument to conduct an in-depth quality appraisal. Results indicate that the majority of systematic reviews in this particular area suffer from important methodological flaws and biases that impair their internal validity and limit their usefulness for clinical and decision-making purposes. To this end, they provide a number of recommendations to strengthen knowledge development towards improving the design and execution of future reviews on home telemonitoring.
9.4. Summary
Table 9.1 outlines the main types of literature reviews that were described in the previous sub-sections and summarizes the main characteristics that distinguish one review type from another. It also includes key references to methodological guidelines and useful sources that can be used by eHealth scholars and researchers for planning and developing reviews.
Typology of Literature Reviews (adapted from Paré et al., 2015).
As shown in Table 9.1 , each review type addresses different kinds of research questions or objectives, which subsequently define and dictate the methods and approaches that need to be used to achieve the overarching goal(s) of the review. For example, in the case of narrative reviews, there is greater flexibility in searching and synthesizing articles ( Green et al., 2006 ). Researchers are often relatively free to use a diversity of approaches to search, identify, and select relevant scientific articles, describe their operational characteristics, present how the individual studies fit together, and formulate conclusions. On the other hand, systematic reviews are characterized by their high level of systematicity, rigour, and use of explicit methods, based on an “a priori” review plan that aims to minimize bias in the analysis and synthesis process (Higgins & Green, 2008). Some reviews are exploratory in nature (e.g., scoping/mapping reviews), whereas others may be conducted to discover patterns (e.g., descriptive reviews) or involve a synthesis approach that may include the critical analysis of prior research ( Paré et al., 2015 ). Hence, in order to select the most appropriate type of review, it is critical to know before embarking on a review project, why the research synthesis is conducted and what type of methods are best aligned with the pursued goals.
9.5. Concluding Remarks
In light of the increased use of evidence-based practice and research generating stronger evidence ( Grady et al., 2011 ; Lyden et al., 2013 ), review articles have become essential tools for summarizing, synthesizing, integrating or critically appraising prior knowledge in the eHealth field. As mentioned earlier, when rigorously conducted review articles represent powerful information sources for eHealth scholars and practitioners looking for state-of-the-art evidence. The typology of literature reviews we used herein will allow eHealth researchers, graduate students and practitioners to gain a better understanding of the similarities and differences between review types.
We must stress that this classification scheme does not privilege any specific type of review as being of higher quality than another ( Paré et al., 2015 ). As explained above, each type of review has its own strengths and limitations. Having said that, we realize that the methodological rigour of any review — be it qualitative, quantitative or mixed — is a critical aspect that should be considered seriously by prospective authors. In the present context, the notion of rigour refers to the reliability and validity of the review process described in section 9.2. For one thing, reliability is related to the reproducibility of the review process and steps, which is facilitated by a comprehensive documentation of the literature search process, extraction, coding and analysis performed in the review. Whether the search is comprehensive or not, whether it involves a methodical approach for data extraction and synthesis or not, it is important that the review documents in an explicit and transparent manner the steps and approach that were used in the process of its development. Next, validity characterizes the degree to which the review process was conducted appropriately. It goes beyond documentation and reflects decisions related to the selection of the sources, the search terms used, the period of time covered, the articles selected in the search, and the application of backward and forward searches ( vom Brocke et al., 2009 ). In short, the rigour of any review article is reflected by the explicitness of its methods (i.e., transparency) and the soundness of the approach used. We refer those interested in the concepts of rigour and quality to the work of Templier and Paré (2015) which offers a detailed set of methodological guidelines for conducting and evaluating various types of review articles.
To conclude, our main objective in this chapter was to demystify the various types of literature reviews that are central to the continuous development of the eHealth field. It is our hope that our descriptive account will serve as a valuable source for those conducting, evaluating or using reviews in this important and growing domain.
- Ammenwerth E., de Keizer N. An inventory of evaluation studies of information technology in health care. Trends in evaluation research, 1982-2002. International Journal of Medical Informatics. 2004; 44 (1):44–56. [ PubMed : 15778794 ]
- Anderson S., Allen P., Peckham S., Goodwin N. Asking the right questions: scoping studies in the commissioning of research on the organisation and delivery of health services. Health Research Policy and Systems. 2008; 6 (7):1–12. [ PMC free article : PMC2500008 ] [ PubMed : 18613961 ] [ CrossRef ]
- Archer N., Fevrier-Thomas U., Lokker C., McKibbon K. A., Straus S.E. Personal health records: a scoping review. Journal of American Medical Informatics Association. 2011; 18 (4):515–522. [ PMC free article : PMC3128401 ] [ PubMed : 21672914 ]
- Arksey H., O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005; 8 (1):19–32.
- A systematic, tool-supported method for conducting literature reviews in information systems. Paper presented at the Proceedings of the 19th European Conference on Information Systems ( ecis 2011); June 9 to 11; Helsinki, Finland. 2011.
- Baumeister R. F., Leary M.R. Writing narrative literature reviews. Review of General Psychology. 1997; 1 (3):311–320.
- Becker L. A., Oxman A.D. In: Cochrane handbook for systematic reviews of interventions. Higgins J. P. T., Green S., editors. Hoboken, nj : John Wiley & Sons, Ltd; 2008. Overviews of reviews; pp. 607–631.
- Borenstein M., Hedges L., Higgins J., Rothstein H. Introduction to meta-analysis. Hoboken, nj : John Wiley & Sons Inc; 2009.
- Cook D. J., Mulrow C. D., Haynes B. Systematic reviews: Synthesis of best evidence for clinical decisions. Annals of Internal Medicine. 1997; 126 (5):376–380. [ PubMed : 9054282 ]
- Cooper H., Hedges L.V. In: The handbook of research synthesis and meta-analysis. 2nd ed. Cooper H., Hedges L. V., Valentine J. C., editors. New York: Russell Sage Foundation; 2009. Research synthesis as a scientific process; pp. 3–17.
- Cooper H. M. Organizing knowledge syntheses: A taxonomy of literature reviews. Knowledge in Society. 1988; 1 (1):104–126.
- Cronin P., Ryan F., Coughlan M. Undertaking a literature review: a step-by-step approach. British Journal of Nursing. 2008; 17 (1):38–43. [ PubMed : 18399395 ]
- Darlow S., Wen K.Y. Development testing of mobile health interventions for cancer patient self-management: A review. Health Informatics Journal. 2015 (online before print). [ PubMed : 25916831 ] [ CrossRef ]
- Daudt H. M., van Mossel C., Scott S.J. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. bmc Medical Research Methodology. 2013; 13 :48. [ PMC free article : PMC3614526 ] [ PubMed : 23522333 ] [ CrossRef ]
- Davies P. The relevance of systematic reviews to educational policy and practice. Oxford Review of Education. 2000; 26 (3-4):365–378.
- Deeks J. J., Higgins J. P. T., Altman D.G. In: Cochrane handbook for systematic reviews of interventions. Higgins J. P. T., Green S., editors. Hoboken, nj : John Wiley & Sons, Ltd; 2008. Analysing data and undertaking meta-analyses; pp. 243–296.
- Deshazo J. P., Lavallie D. L., Wolf F.M. Publication trends in the medical informatics literature: 20 years of “Medical Informatics” in mesh . bmc Medical Informatics and Decision Making. 2009; 9 :7. [ PMC free article : PMC2652453 ] [ PubMed : 19159472 ] [ CrossRef ]
- Dixon-Woods M., Agarwal S., Jones D., Young B., Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. Journal of Health Services Research and Policy. 2005; 10 (1):45–53. [ PubMed : 15667704 ]
- Finfgeld-Connett D., Johnson E.D. Literature search strategies for conducting knowledge-building and theory-generating qualitative systematic reviews. Journal of Advanced Nursing. 2013; 69 (1):194–204. [ PMC free article : PMC3424349 ] [ PubMed : 22591030 ]
- Grady B., Myers K. M., Nelson E. L., Belz N., Bennett L., Carnahan L. … Guidelines Working Group. Evidence-based practice for telemental health. Telemedicine Journal and E Health. 2011; 17 (2):131–148. [ PubMed : 21385026 ]
- Green B. N., Johnson C. D., Adams A. Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. Journal of Chiropractic Medicine. 2006; 5 (3):101–117. [ PMC free article : PMC2647067 ] [ PubMed : 19674681 ]
- Greenhalgh T., Wong G., Westhorp G., Pawson R. Protocol–realist and meta-narrative evidence synthesis: evolving standards ( rameses ). bmc Medical Research Methodology. 2011; 11 :115. [ PMC free article : PMC3173389 ] [ PubMed : 21843376 ]
- Gurol-Urganci I., de Jongh T., Vodopivec-Jamsek V., Atun R., Car J. Mobile phone messaging reminders for attendance at healthcare appointments. Cochrane Database System Review. 2013; 12 cd 007458. [ PMC free article : PMC6485985 ] [ PubMed : 24310741 ] [ CrossRef ]
- Hart C. Doing a literature review: Releasing the social science research imagination. London: SAGE Publications; 1998.
- Higgins J. P. T., Green S., editors. Cochrane handbook for systematic reviews of interventions: Cochrane book series. Hoboken, nj : Wiley-Blackwell; 2008.
- Jesson J., Matheson L., Lacey F.M. Doing your literature review: traditional and systematic techniques. Los Angeles & London: SAGE Publications; 2011.
- King W. R., He J. Understanding the role and methods of meta-analysis in IS research. Communications of the Association for Information Systems. 2005; 16 :1.
- Kirkevold M. Integrative nursing research — an important strategy to further the development of nursing science and nursing practice. Journal of Advanced Nursing. 1997; 25 (5):977–984. [ PubMed : 9147203 ]
- Kitchenham B., Charters S. ebse Technical Report Version 2.3. Keele & Durham. uk : Keele University & University of Durham; 2007. Guidelines for performing systematic literature reviews in software engineering.
- Kitsiou S., Paré G., Jaana M. Systematic reviews and meta-analyses of home telemonitoring interventions for patients with chronic diseases: a critical assessment of their methodological quality. Journal of Medical Internet Research. 2013; 15 (7):e150. [ PMC free article : PMC3785977 ] [ PubMed : 23880072 ]
- Kitsiou S., Paré G., Jaana M. Effects of home telemonitoring interventions on patients with chronic heart failure: an overview of systematic reviews. Journal of Medical Internet Research. 2015; 17 (3):e63. [ PMC free article : PMC4376138 ] [ PubMed : 25768664 ]
- Levac D., Colquhoun H., O’Brien K. K. Scoping studies: advancing the methodology. Implementation Science. 2010; 5 (1):69. [ PMC free article : PMC2954944 ] [ PubMed : 20854677 ]
- Levy Y., Ellis T.J. A systems approach to conduct an effective literature review in support of information systems research. Informing Science. 2006; 9 :181–211.
- Liberati A., Altman D. G., Tetzlaff J., Mulrow C., Gøtzsche P. C., Ioannidis J. P. A. et al. Moher D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Annals of Internal Medicine. 2009; 151 (4):W-65. [ PubMed : 19622512 ]
- Lyden J. R., Zickmund S. L., Bhargava T. D., Bryce C. L., Conroy M. B., Fischer G. S. et al. McTigue K. M. Implementing health information technology in a patient-centered manner: Patient experiences with an online evidence-based lifestyle intervention. Journal for Healthcare Quality. 2013; 35 (5):47–57. [ PubMed : 24004039 ]
- Mickan S., Atherton H., Roberts N. W., Heneghan C., Tilson J.K. Use of handheld computers in clinical practice: a systematic review. bmc Medical Informatics and Decision Making. 2014; 14 :56. [ PMC free article : PMC4099138 ] [ PubMed : 24998515 ]
- Moher D. The problem of duplicate systematic reviews. British Medical Journal. 2013; 347 (5040) [ PubMed : 23945367 ] [ CrossRef ]
- Montori V. M., Wilczynski N. L., Morgan D., Haynes R. B., Hedges T. Systematic reviews: a cross-sectional study of location and citation counts. bmc Medicine. 2003; 1 :2. [ PMC free article : PMC281591 ] [ PubMed : 14633274 ]
- Mulrow C. D. The medical review article: state of the science. Annals of Internal Medicine. 1987; 106 (3):485–488. [ PubMed : 3813259 ] [ CrossRef ]
- Evidence-based information systems: A decade later. Proceedings of the European Conference on Information Systems ; 2011. Retrieved from http://aisel .aisnet.org/cgi/viewcontent .cgi?article =1221&context =ecis2011 .
- Okoli C., Schabram K. A guide to conducting a systematic literature review of information systems research. ssrn Electronic Journal. 2010
- Otte-Trojel T., de Bont A., Rundall T. G., van de Klundert J. How outcomes are achieved through patient portals: a realist review. Journal of American Medical Informatics Association. 2014; 21 (4):751–757. [ PMC free article : PMC4078283 ] [ PubMed : 24503882 ]
- Paré G., Trudel M.-C., Jaana M., Kitsiou S. Synthesizing information systems knowledge: A typology of literature reviews. Information & Management. 2015; 52 (2):183–199.
- Patsopoulos N. A., Analatos A. A., Ioannidis J.P. A. Relative citation impact of various study designs in the health sciences. Journal of the American Medical Association. 2005; 293 (19):2362–2366. [ PubMed : 15900006 ]
- Paul M. M., Greene C. M., Newton-Dame R., Thorpe L. E., Perlman S. E., McVeigh K. H., Gourevitch M.N. The state of population health surveillance using electronic health records: A narrative review. Population Health Management. 2015; 18 (3):209–216. [ PubMed : 25608033 ]
- Pawson R. Evidence-based policy: a realist perspective. London: SAGE Publications; 2006.
- Pawson R., Greenhalgh T., Harvey G., Walshe K. Realist review—a new method of systematic review designed for complex policy interventions. Journal of Health Services Research & Policy. 2005; 10 (Suppl 1):21–34. [ PubMed : 16053581 ]
- Petersen K., Vakkalanka S., Kuzniarz L. Guidelines for conducting systematic mapping studies in software engineering: An update. Information and Software Technology. 2015; 64 :1–18.
- Petticrew M., Roberts H. Systematic reviews in the social sciences: A practical guide. Malden, ma : Blackwell Publishing Co; 2006.
- Rousseau D. M., Manning J., Denyer D. Evidence in management and organizational science: Assembling the field’s full weight of scientific knowledge through syntheses. The Academy of Management Annals. 2008; 2 (1):475–515.
- Rowe F. What literature review is not: diversity, boundaries and recommendations. European Journal of Information Systems. 2014; 23 (3):241–255.
- Shea B. J., Hamel C., Wells G. A., Bouter L. M., Kristjansson E., Grimshaw J. et al. Boers M. amstar is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. Journal of Clinical Epidemiology. 2009; 62 (10):1013–1020. [ PubMed : 19230606 ]
- Shepperd S., Lewin S., Straus S., Clarke M., Eccles M. P., Fitzpatrick R. et al. Sheikh A. Can we systematically review studies that evaluate complex interventions? PLoS Medicine. 2009; 6 (8):e1000086. [ PMC free article : PMC2717209 ] [ PubMed : 19668360 ]
- Silva B. M., Rodrigues J. J., de la Torre Díez I., López-Coronado M., Saleem K. Mobile-health: A review of current state in 2015. Journal of Biomedical Informatics. 2015; 56 :265–272. [ PubMed : 26071682 ]
- Smith V., Devane D., Begley C., Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. bmc Medical Research Methodology. 2011; 11 (1):15. [ PMC free article : PMC3039637 ] [ PubMed : 21291558 ]
- Sylvester A., Tate M., Johnstone D. Beyond synthesis: re-presenting heterogeneous research literature. Behaviour & Information Technology. 2013; 32 (12):1199–1215.
- Templier M., Paré G. A framework for guiding and evaluating literature reviews. Communications of the Association for Information Systems. 2015; 37 (6):112–137.
- Thomas J., Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. bmc Medical Research Methodology. 2008; 8 (1):45. [ PMC free article : PMC2478656 ] [ PubMed : 18616818 ]
- Reconstructing the giant: on the importance of rigour in documenting the literature search process. Paper presented at the Proceedings of the 17th European Conference on Information Systems ( ecis 2009); Verona, Italy. 2009.
- Webster J., Watson R.T. Analyzing the past to prepare for the future: Writing a literature review. Management Information Systems Quarterly. 2002; 26 (2):11.
- Whitlock E. P., Lin J. S., Chou R., Shekelle P., Robinson K.A. Using existing systematic reviews in complex systematic reviews. Annals of Internal Medicine. 2008; 148 (10):776–782. [ PubMed : 18490690 ]
This publication is licensed under a Creative Commons License, Attribution-Noncommercial 4.0 International License (CC BY-NC 4.0): see https://creativecommons.org/licenses/by-nc/4.0/
- Cite this Page Paré G, Kitsiou S. Chapter 9 Methods for Literature Reviews. In: Lau F, Kuziemsky C, editors. Handbook of eHealth Evaluation: An Evidence-based Approach [Internet]. Victoria (BC): University of Victoria; 2017 Feb 27.
- PDF version of this title (4.5M)
- Disable Glossary Links
In this Page
- Introduction
- Overview of the Literature Review Process and Steps
- Types of Review Articles and Brief Illustrations
- Concluding Remarks
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Chapter 9 Methods for Literature Reviews - Handbook of eHealth Evaluation: An Ev... Chapter 9 Methods for Literature Reviews - Handbook of eHealth Evaluation: An Evidence-based Approach
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- Instructions for Authors
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 14, Issue e1
- Impact of dementia on informal care: a systematic review of family caregivers’ perceptions
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- Patrícia Lindeza 1 ,
- Mário Rodrigues 2 ,
- João Costa 3 ,
- Manuela Guerreiro 2 and
- http://orcid.org/0000-0003-3158-2106 Mario Miguel Rosa 4
- 1 ISAMB , Universidade de Lisboa Instituto de Saude Ambiental , Lisboa , Lisboa , Portugal
- 2 Instituto de Medicina Molecular , Lisboa , Lisboa , Portugal
- 3 Universidade de Lisboa Centro de Estudos de Medicina Baseada na Evidência , Lisboa , Lisboa , Portugal
- 4 Lab Farmacologia Clínica , Universidade de Lisboa Faculdade de Medicina , Lisboa , Portugal
- Correspondence to Dr Mario Miguel Rosa, Lab Farmacologia Clínica, Universidade de Lisboa Faculdade de Medicina, Lisboa 1649-028, Portugal; mrosa{at}medicina.ulisboa.pt
Introduction Caregivers play a major role in providing all the support and care in daily activities for their relatives with dementia. To fully describe the influence of dementia caregiving on family caregivers’ life, we conducted a systematic review including caregivers’ perceptions about the positive and negative aspects of caring and the expressed factors.
Materials and methods We conducted a systematic review including articles from January 1998 to July 2020. Qualitative studies reporting family caregivers’ perceptions about their experiences and the effects/impact of dementia caregiving were eligible. Two authors extracted the data independently, and the analysis focused on the positive and negative aspects of dementia caregiving in caregivers’ life.
Results Eighty-one studies with 3347 participants were included in this review. The positive aspects of caregiving in caregivers’ life encompass personal accomplishment and strengthening relationships, which were enhanced by good medical counselling/formal care support and family/friends support. The negative aspects included emotional and social aspects experienced by caregivers. Other factors such as inappropriate medical/formal care support, illness progression and the costs of dementia contributed to negative appraisal.
Discussion and implications The findings provide insights into the holistic experience of caring for a person with dementia revelling the major positive and negative aspects underlying the caregiver role. The evidence emphasises the need ‘to focus on positive aspects’ and targeted interventions aimed at reducing the negative impact of caregiving, which has serious consequences on caregivers’ quality of life. A multicomplex intervention for dementia informal caregiving should be developed, committing the society to promote mental health, address these community needs and improve the quality of life of the person with dementia and their family caregivers.
- quality of life
- family management
- supportive care
- end of life care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bmjspcare-2020-002242
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Introduction
Dementia is a clinical syndrome characterised by a cluster of symptoms manifested by difficulties in memory, disturbances in language and cognitive functions, changes in behaviours, and impairments in activities of daily living, and includes a range of neurological disorders characterised by memory loss and cognitive impairment. 1 2 With the growth in ageing populations, the number of persons with dementia is increasing, with no sign of a cure for the disease. It is probably underdiagnosed, with an estimated half of primary care patients aged over 65 years not diagnosed by their primary care physicians. 3 4 The most common form of dementia is Alzheimer’s disease (AD), accounting for 50%–70% of dementia cases. Prevalence has undergone a huge increase in recent years, and it has become one of the greatest healthcare challenges of the 21st century due to the high demand for medical, social and institutional care. 5 6
Before institutional care, family caregivers play an important role for people with dementia, helping them in their daily activities, whose dependence increases with severity of the disease. 5 7 8 Taking care of a person with dementia demands several logistic tasks, including personal care, housekeeping, administration of medication, processing financial transactions and other activities and with disease progression caregiving for the patient’s well-being becomes more important. 1 9
The task of caregiving is complex and can lead to physical, mental and financial stress for caregivers. Emotions such as guilt, resentment, sadness and the effort expended, as well as the anticipated loss of the relative, emerge. 9 As a result, informal caregivers suffer significantly higher levels of psychological morbidity, depression, stress and burden. 10–12 The uncertainty about the future may create an ambiguous situation for family members and increase the burden on the caregiver. 13 Despite these, some caregivers see their role as an opportunity to strengthen the relationship with their relatives.
Healthcare professionals have an important role in providing support to caregivers. They may refer caregivers for counselling, which has been shown to reduce caregiver distress, assist patients to stay at home longer, and inform caregivers about support organisations. 5 There is evidence suggesting that caregiver needs are not being met by healthcare professionals, which leads to the decline in their physical and mental health. 14 15 Caregivers’ perspectives are of high importance as these help to better describe caregivers’ role and identify potential ways to improve daily tasks, resulting in a more positive experience.
A large proportion of studies discuss the positive and negative influences of caregiving on particular aspects such as gender, nature of the relationship or caregivers’ age. 7 16 17 To describe the task of caregiving, it is important to approach this as a global phenomenon, that is, understanding the caregiver’s needs and perceptions that positively or negatively contribute to their quality of life and their provision of daily support as caregivers. We conducted a systematic review of qualitative studies to understand the holistic experience of caring for a person with dementia, including not only the positive and negative aspects of caregiving through caregivers’ perspectives, but also the expressed factors that affect those experiences.
Materials and methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 18 and was performed to identify and summarise the impact of caring for persons with AD/dementia on family caregivers’ life through their own perceptions.
Search strategy and inclusion criteria
Two authors (PL, MR) performed electronic searches for relevant sources in OVID Medline, EMBASE, Web of Science, Scopus and PsycINFO. These databases were selected due to the high relevance of their indexed articles to this study’s topic. The results of this search were supplemented by hand-searching of the reference lists of the retrieved articles. Languages included were English, French and Spanish, with publication dates restricted to January 1998–July 2020. The start date of the review was the time when symptomatic treatment for AD was marketed, and the inclusion criteria for pivotal efficacy trials better discriminated AD from other dementias, namely vascular dementia. 19 The studies published after 1998 were more consistent with our disease criteria and were therefore selected for this review.
The full search strategy and the inclusion/exclusion criteria are available in Box 1 (see additional file 1 of the online supplemental material for more details). Studies including a mix of participants (caregivers, care recipients and/or healthcare professionals) were included in the content analysis, but the perspectives of healthcare professionals and care recipients were excluded.
Supplemental material
Systematic review of literature: search terms, inclusion/exclusion criteria and information extraction.
Search terms.
Alzheimer disease OR mild cognitive impairment OR cognitive dysfunction OR dement*.
Interviews OR interview* OR surveys and questionnaires OR survey* OR questionnair* OR focus groups OR geriatric assessment OR health impact assessment.
Caregivers OR caregiv* OR carer OR family OR famil* OR patient care.
Illness behaviour OR cost of illness OR activities of daily living OR quality of life OR self concept OR stress, psychological OR sick role OR outcome assessment health care OR health expenditures OR health care costs OR self-perception.
Cohort studies OR longitudinal studies OR follow-up studies OR prospective studies OR retrospective studies OR cohort OR longitudinal OR prospective OR retrospective.
1 AND 2 AND 3 AND 4 AND 5.
Limit 6 to year of publication: January 1998–July 2020.
Inclusion criteria.
Original qualitative empirical data.
Paper in English, French or Spanish.
Including family or informal caregivers of people with dementia and/or Alzheimer’s disease and/or mild cognitive impairment.
Methods including focus groups and/or survey/questionnaire and/or interviews.
Exclusion criteria.
Quantitative studies, reviews of literature, opinion-based studies and protocol studies.
Studies before 1998.
Not addressing caregivers’ perceptions.
Studies where caregivers’ perceptions were related to the results of intervention programmes.
Addressing other conditions than dementia and/or Alzheimer’s disease and/or mild cognitive impairment.
Addressing outcomes other than caregivers’ perceptions about caregiving daily life.
Information extracted from included papers.
Study description, setting and population.
Sampling criteria, number of participants and response scores (when presented).
Study methodologies and limitations, and methods of data analysis.
Outcome measures.
Key findings/themes/results and main conclusions.
Implications for policy and practice and suggested future research.
Bibliographic details.
We downloaded all articles into Mendeley and deleted the duplicates. The abstracts and full-text copies were scrutinised by two independent reviewers (PL, MR), who applied the predefined inclusion/exclusion criteria (see box 1 ), with disagreements resolved through discussion or via a third reviewer (MMR), with a presumption of inclusion in cases of doubt.
Data extraction
Two authors (PL, MR) extracted the data independently from each study: information related to authors, publication year, study aims, theoretical/conceptual frameworks, sampling/sample characteristics, analytical approach, summary and outcomes. The selected studies were analysed in order to explore the positive and negative aspects experienced by caregivers while caring for their relative and the expressed factors that contributed to these positive and negative appraisals. With regard to data extraction, divergences were solved between authors, and 100% consensus regarding data extraction was reached.
Quality appraisal
Two authors (PL, MR) independently assessed the quality of each study using the Critical Appraisal Skills Programme (CASP). 20 We assigned yes/no to eight questions related to the study methodology, as listed in CASP: clear statement of the study aims, appropriateness of the qualitative methodology, research design, recruitment strategy, data collection, considerations of the relationship between the researcher and the participants, ethical issues and rigour of data analysis (see box 1 in the online supplemental material ). We did not exclude any study during the quality appraisal as they might generate new insights.
Data analysis
Narrative review was selected as the method for data synthesis since the included papers were qualitative studies. 21 Selected papers were carefully read by the authors (PL, MR). Data findings from the primary studies were independently coded and organised (keywords, short sentences and so on) into positive or negative aspects of caregiving or the expressed factors contributing to positive or negative appraisal. Two authors independently performed the data analysis and consulted a third researcher (MMR) when required. Finally, the two authors worked together to re-examine significant statements and identify excerpts and/or original quotations from the studies that could best illustrate the themes selected for this study.
Type and quality of the results
The search strategy yielded 2376 publications, of which 118 were selected for full-text review, with 81 studies finally included in this systematic review ( figure 1 ). The studies were analysed to identify informal caregivers’ perceptions about the positive and negative aspects of caregiving and the factors that contribute to those experiences ( table 1 ). The characteristics of the included studies are presented in the online supplemental material, table 2 . With regard to methods, 52 studies used focus groups; other methods included interviews, questionnaires and mixed methods (see the online supplemental material, table 3 ). A total of 3347 participants were included; 82.1% were family caregivers. Qualitative methods to identify the experiences/perceptions of family caregivers were found in all studies; a few studies also presented the views of patients with mild cognitive impairment, patients with dementia and former caregivers (these perceptions were not included in this review).
- Download figure
- Open in new tab
- Download powerpoint
Study flow chart. AD, Alzheimer’s disease; MCI, mild cognitive impairment.
- View inline
Examples of studies that included positive, negative or combined aspects of caregiving role (N=81)
Study quality
The quality of the included studies was assessed using CASP 20 (see online supplemental material, table 1 ). Most studies used convenience samples, while some evaluated the representativeness of participants; however, all studies clearly reported the aims, design and sampling. Data analysis was fully described in 35 studies and partly described in 46 studies, while data collection was fully described only in 9 studies. All studies either fully or partly explicitly stated the ethical issues, but only one described the relationship between the interviewer and the participants.
Caregivers’ perceptions of the effects of caring for a person with dementia
Caregiving was described as a big life change: “It effectively changes your life. Your priorities change. Your lifestyle changes. Your attitude to the person you are giving care to changes. Your role changes.” 22 Analysis of the included studies revealed positive remarks about the caregiving role, which were present in a small number of studies (18 studies), while negative aspects were present in 76 studies, including studies that combined both aspects. Examples of each and combined aspects are presented in table 1 (for all studies that encompass positive and negative aspects of caregiving, see online supplemental material, table 2 ).
The positive aspects found were presented as personal aspects experienced by caregivers that can be enhanced by good medical counselling and formal care support and family/friends support. Negative aspects were particularly related to emotional and social aspects of caregiving, and factors such as inappropriate medical and care support, illness progression and costs related to dementia (eg, formal care costs, medications costs and so on) enhanced negative appraisal (see table 2 ).
Main positive and negative aspects and related factors influencing caregivers’ role (N=81)
Positive aspects and the expressed related factors of caregiving according to caregivers’ perceptions
Providing support for the relative and having “made a difference” to their family’s life were considered to have positive effects on caregivers’ life and were a relief for caregivers, as they were able to fulfil their obligations as son/wife/daughter or others:
(…) What I am looking to do is just staying home and watch my husband. That’s what I have to do. And if that’s what I have to do, I don’t mind doing that. It gives me great joy to give back to my mom and…I tease her…uh…on a good day, and I say “Aren’t you glad you took good care of me, because you set that example?” And she’ll laugh and I’ll laugh and…and it gives me great joy, because she…uh…was/is a great mother. And uh…and…and now, it’s my turn to be a great daughter. 23–26
For some family caregivers, the chance of doing meaningful activities together and be able to return the favour to their parents/family members was indicated as being grateful: “I enjoy the time with my mother…I love to hear her laugh…We talk all the time in the car; we pray together, watch TV.” 26 27 Respect for the individuality of the person with dementia was reported as crucial to caregivers, who were grateful to know that the individuality of their family members was being respected in the nursing home:
I think their individuality and their dignity is vital. They have all got their own (personal) things (in the nursing home). 28
By having their own things, patient well-being and dignity appears to guarantee to turn initialization into a more personal experience.
The main expressed factors that contributed to the positive aspects of caregiving were related to good medical counselling and formal care support, as well as family and friends support ( table 2 ). Access to useful information about the disease and its evolution was considered essential to caregivers. Acquiring knowledge helps caregivers to better assume caregiving role and prepare them to prevent and deal with specific situations: “I would like to know. I mean I am worried about the future…Because I don’t know anything!” 29
Appropriate medical counselling, formal support and healthcare professionals support for patients were found to be good resources to overcome caregiving challenges and decision-making processes that rely on caregivers: “Well, for me, what would improve my quality of life mostly is to have better support from healthcare professionals, (…) just keeping him clean is extremely challenging (…).” 30 Caregivers considered good aspects of formal care when the staff “have the knowledge and techniques on how to handle the residents and their behaviours” and “That it was good to see their relatives in a safe, secure and loving environment.” 31 Caregivers also benefit from medical and psychological support where the disease can be acknowledged and where they can be understood: “The regular visits to the psychologist were very helpful. It is really important you have someone to talk to during the dementia process who understands you.” 32
The need for an early diagnosis of dementia was quite evident, mainly due to the bad experiences and endless diagnostic procedures previously experienced, but also due to the relief felt after the diagnosis: “I felt very relieved when we finally got the diagnosis…I just felt validated that finally someone knew what we knew.” 33 Through caregivers’ perception, early diagnosis has the positive effects of relief and care improvement, thus allowing for a more effective caring process for their families afterwards:
Well, if I had known that the man was sick, first of all, he wouldn’t have been left alone as long as he was. Second of all, I wouldn’t have blamed him for his actions. I would have known it was the disease. We did a lot of damage emotionally to him as well as to ourselves, and there’s a lot of guilt associated with what we had done, so I think diagnosis as early on as possible is the best possible thing that can happen . 33
Family and friend support was another factor that positively enhanced the experience of caring. The value of old friendships that remains after diagnosis helped reduce caregivers’ feeling of loneliness: “(…) Many of our friends, if anything, they’ve stepped up and they helped us.” 34 35 Family support is particularly important when it provides free time for the principal caregiver to do his own activities: “She would stay with my sister for approximately three months.” 36 This aspect was regarded by caregivers as very positive to their quality of life. Unfortunately, most admitted to be single caregivers for their relative and have no spare time for themselves or other activities besides caring. 34 35
Negative aspects and expressed related factors of caregiving according to caregivers’ perceptions
Caregivers’ perceptions about the negative aspects of caregiving comprise emotional and social aspects, such as fear, worry, stress, sadness, social isolation and problems accepting their relatives’ diagnosis. Additionally, caregivers experienced concerns about the future since they do not know what to expect and for how long they can ensure the emotional and economic support for themselves and their relatives’ well-being.
Mental, emotional and physical efforts are seen as requirements to deal with patient sleep disorders—“I can’t handle this anymore; I’m absolutely buggered from no sleep at all night” 37 —and behavioural changes (which in some cases lead to physical/verbal aggressions), with some caregivers declaring their own need for therapy:
In fact, I do need therapy, too. I mean if there are not two or three people to care for the patients, you are psychologically affected. I am a prisoner at home. For a couple of times I cried. They say boys do not cry, but I did…. I sometimes have nervousness, anger and crying attacks. (…) I used to be full of life; I used to like visiting and having holidays. I can say that I cannot bear this situation anymore. 38
The caregiver role demands too many hours for care, with no time for personal life, which is reflected in caregivers’ difficulties in maintaining their professional and social life, and their responsibilities as parents:
I can’t leave him. For 24/7 I’m with John. 39 I would say if you’re going to be a caregiver it’s a full-time job. You don’t have time to do anything else if you’re going to do it right. 40 (…) I think that there’s such isolation for the caregiver because you often don’t have someone to talk to unless you have a large family. I tend to not have friends that, they don’t want to hear anything that you are doing this. 41 I live a little way away and I’ve got four children; and that’s hard in itself. I have to look after her as well. Some days, I might be having a crisis before I have even seen her. 42
For caregivers, there was a permanent concern about their relatives’ well-being and the capacity to provide safe and effective care which could prevent the possibility of serious injuries to occur, particularly fractures due to falls. The comorbidities that persons with dementia usually have, also increase the need for adaptation of care required, including special food intake.:
(…) He cannot swallow and coughs each time he swallows and it blocks his throat. My mom was a diabetic for 40 years. If she didn’t eat in the morning, hypoglycemia was inevitable. Whenever my mother would refuse eating breakfast, I would become angry and mom would also fight and insist on not eating. 38 43
Food was an important aspect for some caregivers, since the high level of calories needed to support their relatives has consequences on their own weight and health. Also, for many of the male caregivers, the concern with the process of feeding their relatives was new, leaving the need to learn new things, besides their relatives’ condition. 44
For some caregivers, the time of diagnosis brought great frustration due to inexistent communication with health services, constant change in formal care providers and lack of information: “I don’t think that any of the doctors that we were involved with ever offered any help as far as what to do next.” 33 45 46 The process of dealing with health and social care services for the person with dementia was described as a “battle” or “fight”. 47 After the diagnosis, the uncertainty about the future and the inability to accept their relatives’ condition led to stress, frustration and sadness. 35 48 49 For caregivers, it was difficult to deal with the fact that they were not recognised by their relative with dementia: “And I think that the dementia would then progress rapidly to a stage where she no longer recognises anybody.” 24 Some caregivers admitted to start grieving the loss during the course of the disease:
I have been grieving losses over the whole period of illness; there was a loss of person before a loss of body. 50 I started grieving years ago when mother didn’t recognize us…That’s when I lost my mother…When she physically died I felt like I lost my baby. 51 It may be a bad thing to say but I’m hoping before she starts really seriously deteriorating she’ll pass on. 35 50
The social isolation due to the loss of old friendships and the lack of family support seem to have a huge negative impact on caregivers’ personal and social life. 52 Over time, caregivers tried to adapt to the circumstances and sought professional help, aiming to deal with their exhaustion and emotional problems:
I am having emotional problems from the stress and sadness of seeing such a low quality of life in my mother. Dementia is an emotional process which you enter together. Eventually you reach your limit (…). 32 I did not get enough emotional support. I needed more emotional support from friends and community. 36
For some participants, caregiving was considered an obligation that results in a higher emotional impact: “I hardly cry, I have almost never cried. I got distressed and felt ill. I tried to manage it by myself. I was obliged to accept it when nobody gave me a hand.” 38
The inappropriate medical and formal care support, the daily perception of disease progression, and the high costs of illness were the main expressed factors that contributed to the negative aspects of caregiving ( table 2 ).
Formal care services were largely associated with patient isolation and superficial or poor care:
In an ideal world one would not allow the patients to sleep all day. 28 We had home care [for mother] until they [home care staff] got accused of stealing, got fired, got thrown out …. 53
The lack of formal support made caregivers feel they are left alone: “I just don’t understand why they [home care staff] are so unhelpful…I think something needs to be done, because we don’t seem to get any help really from anywhere. You’re just a bit left on your own.” 54 Inappropriate medical care was also reported by caregivers: “I was kind of astonished that the doctors were unsupportive, not only unsupportive, really very negative…this is a doctor and he’s telling me not to treat my father….” 55 Diagnosis commonly triggered search for better medical counselling:
I didn’t get any help at all. He just said that my husband had depression. In the finish and because I kept going back…and anyway it wasn’t…and I ended up having to pay for a specialist to get him referred to try and get him a diagnosis…We didn’t get any help at all. I didn’t get sent anywhere…. 56
The decision-making process is typically the responsibility of caregivers, leading to an impact on their own feelings and well-being. For example, placing the feeding tube, resuscitating and even choosing permanent formal care, such as a residence or nursing home, are very difficult decisions to make and bring feelings of sadness and guilt:
I promised faithfully that he would never go to a residence, and I still feel guilty. 57 I mean it’s totally on my shoulders too. And sometimes the amount of guilt is there, I mean it just weighs me down so much. But then I have to split myself, I still have kids at home, and I have to split myself there too. 40 Resuscitation was the biggest decision…I consulted with my children and my wife’s sisters and they were all in agreement…she has gone through enough . 58
Another negative factor that contributes to increased burden in the caregiver is the constant loss of patient competences, losing their ability to do daily activities such as walking, dressing, going to the bathroom, bathing, driving or cooking in an independent way, overloading the caregiver:
I’ve had to do it all . I bathe him because he is afraid. He does not finish it and leaves. He does not completely shave. For example: he cuts the right side of the moustache and leaves the other side. He eats but does it in a mess. 23 26 38 44 59 60
Witnessing the daily progressive health decline of their relatives, especially in the later stages of the disease, is a process that has significant impact on caregivers: “In the later stages it’s so difficult for them to indicate what their needs are.” 24 28 31 61 With the patient’s loss of abilities, caregivers try to adapt to the circumstances and might consider getting professional help at this point. 35 54 59 62 Another negative aspect that has a major impact is behavioural change, which in some cases leads to physical or verbal aggressions:
He’s very much reliant on me (…) He’s suddenly becoming aggressive, and gets angry really with no reason at all…. 63 She also gets quite aggressive when it comes to her kind of personal care really. You know she doesn’t like having a shower, having her hair washed…. 64 It is very hard for me to handle her behaviour (…) I know that you shouldn’t mention it and/or joke about it. But I’ve noticed that I still do it. I’m still having a hard time accepting how much my mother has changed (…). 65
On top of the above-mentioned negative aspects, the cost of the illness had a huge negative impact on caregivers’ daily living and well-being. Without a job in some cases, keeping up finances with the high cost of bills and home care is also a constant worry and is seen as a barrier to accessing formal care:
I can’t afford a decent one (home care service). Cost is a barrier for lots of people. You know, there’s a limit to how much home care they use because of the cost. 48 66
Another concern of caregivers is the duration of the disease:
I knew we had money if mom lived for one to two years, but if she lived for 20 … it was a big worry and a burden. I don’t have an unlimited amount of money for my mom. I am trying to sell her properties and get her settled. I am continually worried about resources . 51 59
Thus, financial guidance/support for this community is of great relevance not only to guarantee daily basic support of food, bills and medications, but also the need for institutionalisation and all other support that patients may require during their lives.
Discussion and implications
The current review focused on the perceptions of informal caregivers with regard to the holistic experience of caring for a person with dementia, including the positive and negative aspects. The included studies reviewed the diverse feelings and emotions that caring brings to caregivers. The diagnosis of dementia seems to generate positive consequences in the relationship between the caregiver and their relatives, contributing to a stronger relationship than before. 17 This strengthening of family ties has also been reported in other diseases such as cancer. 67 This fact may be related to the family companionship that is needed to face the disease and is probably related to the type of disease. Chronic diseases and/or a poor prognosis are seen to cause a very high burden to the patient, but can be reduced with the family being closer together. As described by Gitlin et al , 68 most of the caregivers found in caregiving a chance to “return the favour” to their relatives and the opportunity to do activities together, reducing both caregiver burden and behavioural symptoms of dementia, which is in agreement with our findings. Findings from Elnasseh et al 69 are consistent with past literature showing that the quality of previous familiar relationship is relevant when a family member becomes a caregiver. In families with healthier dynamics, caregivers are more likely to have greater personal strengths, while families with poor affinity are more likely to experience increased caregiver burden. 43
Finding good medical counselling and formal care support, as well as the the opportunity to enhance family cohesion, and the presence of friendships, especially old friends who remain after the diagnosis, were factors that contributed to positive appraisal. As previously demonstrated by Vellone et al , 70 all kinds of help and support are welcomed by caregivers, as these give them free time for themselves. Sharing caregiving tasks is a concrete way to reduce caregiver stress, with the free time being used by caregivers for activities such as going to the gym, taking a walk, going out with friends or just taking a nap. After relaxation, the caregiver would be much more ready to better take care of their relatives. The availability of formal care support, in addition to positive experiences with formal care, and good home care/day care services are important to caregivers, once they have perceived the knowledge, security and dignity needed to care for a person with dementia. Furthermore, good formal care can support caregivers in their role, reducing the burden and the negative impact of their daily routine. A recent review by Yu et al describes the positive influences of caregiving related to caregivers’ personal issues, highlighting feelings such as gratification and meaning in life, which is in accordance with our findings. 71 Additionally, we identified other factors that contributed to positive and negative experiences in caregivers’ daily life. This knowledge is crucial to the development of measures/programmes targeted at caregivers, which should consider caregiver concerns, but also empower them by highlighting the positive aspects and providing support (good formal care services, family support and so on). The result will broaden the spectrum of action of these types of programmes and improve the caregiving experience on several levels.
The imbalance of the negative over the positive aspects of caregiving has been shown in previous studies, with implications for both mental and physical health effects in caring. 14 15 A study of Pinquart and Sörensen 72 suggests that caregiving of individuals with dementia is more stressful than caring for individuals with other diseases. This phenomenon is probably related to the increased amount of time that caregiving for a person with dementia may involve, resulting in loss of spare time and consequent social isolation. 9 Most of the caregivers sacrifice their activities and hobbies, restrict their time with friends and family, and give up employment or reduce time at work. Therefore, caregivers tend to lose their meaning in life, or set it aside, leaving an opportunity for mental health problems to emerge, which can worsen in the future as a result of the emotional burden they are exposed to. 73 74 Anticipated loss is common in caregivers, and as previously described in the literature grieving over the whole period of illness increases the possibility of having a postdeath complicated grief. 75
The health of the caregiver has been studied by Widera et al , 76 who suggested that caregivers are less likely to engage in preventive health measures, leading to increased risk of mortality. One factor that may be contributing to this situation is the financial burden associated with caring for a person with dementia. Moreover, the daily overload, the patient’s dependence and the decision to stop working in order to care for their loved ones lead to postponement of medical examinations among caregivers, negatively impacting their health status. 76 77 Usually, caring for their relatives becomes a priority; however, this process is often done alone, resulting in the tendency of caregivers to forget to take care of themselves. Healthcare professionals have a central role in improving access and quality of health services to caregivers (which have been shown to reduce caregiver distress and assist patients to stay at home longer). However, little has been done with regard to the promotion of a healthier life for caregivers, who are known to be in need of good health support and monitoring. 5 76 Little is known about caregivers’ health and quality of life, and this is an important issue that requires more studies that better describe the general health status of caregivers and provide directions to improve their health condition. The general health of caregivers deserves a great deal of attention as negative health outcomes contribute to the risk of future serious health problems, compromising not only the caregiver’s health but also the care that is being provided to the patient. 78
Previous studies have reported that the patient’s dependence on activities of daily living is described by caregivers as one of the hardest things to deal with, which is due to the amount of care that needs to be provided. This is in accordance with the findings found in the studies included in this review. 79 80 Throughout the progression of the disease, the patient’s behavioural symptoms (agitation, sleep disturbance, wandering and apathy) and psychological symptoms (anxiety, depression, delusions and hallucinations) have a significant impact on caregivers, proving the negative experiences of caregivers.
Moreover, the effects of night agitation and sleep disturbances experienced during caregiving lead to poorer subjective sleep quality and higher rates of daytime sleepiness among caregivers of persons with dementia compared with non-caregivers. These factors, combined with daily routine, disease progression and the patient’s dependence, can lead to caregiver exhaustion. 81
The cost of the illness had a huge impact on caregivers’ routine, with the increased cost of formal care and medication becoming a concern. Cost is probably the reason caregivers resort to formal care as the disease becomes more severe, resulting in behaviour problems and more disabilities. 82 83 Supporting a person with dementia in their own home costs less than bringing them to a care home. As previous literature suggests, the transition from informal to formal care occurs mainly in the later stages of dementia and is considered as supplement to care since the caregiver remains present in all processes. 84 Additionally, caregivers attribute the change from informal to formal care as a failure of their responsibilities or make them feel they are bad family members. 85 86 The long waiting lists and the costs were further barriers that delay access to these services.
The economic environment of caregivers is never too comfortable since they are caring for their relatives and not being paid for this full-time job. As informal care is unpaid, it is viewed as a costless substitute to formal care. However, informal caregiving is not free of costs, which makes it relevant to estimate the value of the hours that caregivers spend on caring for their relatives in order to better know the monetary costs of informal caregiving and develop better financial support to these specific cases. Timely access to dementia care services and fairer costs are crucial to reducing informal caregiver burden and to increasing the quality of life of patients and caregivers. 87
Although it may be thought that the caregiver’s role is less important with the patient’s admission to a care facility, the caregiver remains involved in terms of important legal, financial and healthcare decisions. 88 89 The decision-making process becomes tougher with the associated ethical and emotional responsibilities. Family, friends and medical support is critical as this allows caregivers to better decide and deal with the feelings associated with the decision. 90
Due to the increasing complexity of caregivers’ responsibilities, training programmes are important to help caregivers understand and manage care recipients’ behaviour problems and thus reduce negative experiences. 91 However, despite the several interventions developed with the goal of alleviating caregiver burden, the experience continues to be very negative for caregivers. Why are these programmes/interventions not having the expected results of decreasing burden among informal caregivers? Caregivers are mostly women and elderly. Are these interventions well set to the target population? Do these programmes really fulfil the needs of families on an individual basis? It is suggested that personalised and multicomponent interventions, including a diversity of services (directed at the patient and the caregiver), will decrease burden, improve quality of life and enable home care for longer periods prior to institutionalisation. 92 The transition to formal services is postponed by family caregivers who, despite all the negative aspects of caregiving, chose to care for their relatives and provide them the best care they can. Interventions should demystify institutionalisation as a failure of the caregiver and should focus on facilitating a healthier transition to warrant patients and caregivers a sustained well-being for as long as possible. Also, it is important to provide interventions not only to caregivers, but also to former caregivers (who are usually neglected). There is evidence that the grieving process can be very stressful and can lead to depression.
The number of people suffering from dementia is expected to increase in the coming decades, and there is a need to strengthen informal caregiving to meet not only the care recipient’s needs, but also the caregiver’s needs. Adequate knowledge on the aspects that caregivers describe as positive and negative in caregiving experience and providing tools to level these aspects are urgently needed. Overall, a multicomplex intervention for dementia caregiving should be developed, with the entire society being invited to promote mental health, address caregivers’ needs and improve the quality of life for the person with dementia and their family caregivers.
Strengths and limitations
The strength of this systematic review is its description of the phenomenon of caregiving for a person with dementia, through the views of informal caregivers, encompassing both positive and negative experiences. The use of CASP for quality appraisal by two independent researchers strengthened the results. However, some studies presented methodological limitations that may impact the level of evidence, as some of the studies did not use appropriate theoretical frameworks, which is a limitation of qualitative research. The comprehensiveness of caregiver experiences might be limited because most studies did not primarily examine caregivers’ positive and negative experiences. The focus of the individuals included was on specific issues such as caregivers’ perceptions in formal care, family support, time of diagnosis and so on, and consequently reported limited aspects about the entire experience of caregiving.
Only qualitative studies have been included, and the results of quantitative studies were excluded. In addition, including only informal caregivers’ perceptions resulted in the exclusion of views of persons with dementia and formal caregivers. It is also important to consider other aspects of caregiving. Additionally, care recipient and caregiver characteristics such as demographics, relationship, gender and so on, which might influence caregiver experience, were not considered.
The study findings have important implications for the development of interventions that comprehensively address caregivers’ individual needs based on their experiences, and demonstrate there is a need for more rigorous qualitative studies that explore the perceived positive and negative aspects of caregiving. Altogether, these studies may generate new insights into the planning and design of more robust and flexible intervention programmes.
Ethics statements
Patient consent for publication.
Not required.
Acknowledgments
The authors acknowledge 'Fundação para a Ciência e Tecnologia (FCT)' Portugal and Merck Sharp & Dohme Portugal.
- Winblad B ,
- Amouyel P ,
- Andrieu S , et al
- Kadziola Z ,
- Brnabic AJ , et al
- Kivipelto M ,
- von Strauss E
- Verbeek H ,
- Leino-Kilpi H , et al
- Brodaty H ,
- Ibarria M ,
- Alegret M ,
- Valero S , et al
- Dening KH ,
- Greenish W ,
- Jones L , et al
- Connell CM ,
- Janevic MR ,
- Gilliam CM ,
- Livingston G ,
- Givens JL ,
- Mazor KM , et al
- Sörensen S ,
- Pinquart M ,
- Eazor LR , et al
- Liberati A ,
- Tetzlaff J , et al
- Critical Appraisal Skills Programme (CASP)
- Dissemination C for R
- Butcher HK ,
- Holkup PA ,
- Buckwalter KC
- Joosten-Weyn Banningh L ,
- Vernooij-Dassen M ,
- Rikkert MO , et al
- van Wezel N ,
- Francke AL ,
- Kayan-Acun E , et al
- Habermann B ,
- Shulver W ,
- Killington M , et al
- De GF , et al
- Oliveira D ,
- Aubeeluck A
- Edwards H ,
- Wolfs CAG ,
- de Vugt ME ,
- Verkaaik M , et al
- Stuckey JC , et al
- Karlin NJ ,
- Jamieson M ,
- Grealish L ,
- Brown J-A , et al
- Tekinsoy KP OC , et al
- He G-P , et al
- Bern-Klug M ,
- Polenick CA ,
- Struble LM ,
- Stanislawski B , et al
- Ledgerd R , et al
- Park J , et al
- Fjellström C ,
- Starkenberg Åsa ,
- Wesslén A , et al
- Robinson L , et al
- Manthorpe J ,
- Campbell S , et al
- Forbes DA ,
- Markle-Reid M ,
- Hawranik P , et al
- Prorok JC ,
- Hussain M ,
- Horgan S , et al
- Hemingway D ,
- MacCourt P ,
- Pierce J , et al
- Juozapavicius KP ,
- Hallberg IR ,
- Karlsson S , et al
- Morgan DG ,
- Semchuk KM ,
- Stewart NJ , et al
- Middlemass J ,
- Laparidou D ,
- Karran T , et al
- van Gennip IE ,
- Pasman HRW ,
- Oosterveld-Vlug MG , et al
- Sutcliffe CL ,
- Jasper R , et al
- Sarabia-Cobo CM ,
- de Lorena P , et al
- Livingston D , et al
- Jennings LA ,
- Palimaru A ,
- Corona MG , et al
- Chiu Y-C , et al
- Moreno-Cámara S ,
- Palomino-Moral Pedro Ángel ,
- Moral-Fernández L , et al
- Karlsson S ,
- Bleijlevens M ,
- Roe B , et al
- De Bellis A ,
- Duxbury J ,
- Pulsford D ,
- Hadi M , et al
- Huis in het Veld J ,
- van Meijel B ,
- van Meijel B
- HuisinhetVeldJ , et al
- Zabalegui A ,
- Rodriquez E , et al
- Bouhnik A-D ,
- md D , et al
- Gitlin LN ,
- Burke J , et al
- Elnasseh AG ,
- Trujillo MA ,
- Peralta SV , et al
- Vellone E ,
- Talucci C , et al
- Cheng S-T ,
- Hadzi-Pavlovic D
- Greenwood N ,
- Smith R , et al
- Blandin K ,
- Eric Widera MD ,
- Covinsky KE ,
- DeFeis BL ,
- Gu Y , et al
- Quittner AL
- Gallagher D ,
- Ni Mhaolain A ,
- Crosby L , et al
- Thapsuwan S , et al
- Mok V , et al
- van Vliet D , et al
- Albert SM ,
- Bell K , et al
- Vossius C ,
- Testad I , et al
- Zwakhalen SMG ,
- Challis D , et al
- Rönnbäck E ,
- Larsson B , et al
- Carey K , et al
- Stirling C ,
- Leggett S ,
- Lloyd B , et al
- Bonner GJ ,
- Wilkie DJ , et al
- Hebert LE ,
- Scherr PA ,
- Bienias JL , et al
- Goodall D ,
- Harrison BE
- Dincarslan O
- Harmer BJ ,
- Boots LMM ,
- Verhey FRJ , et al
- Bamford C ,
- McLellan E , et al
- Laditka SB ,
- Price AE , et al
- Lampley-Dallas VT ,
- Phillipson L ,
- Aminzadeh F ,
- Byszewski A ,
- Molnar FJ , et al
- Zeng F , et al
- Elliott BA ,
- Gessert CE ,
- Peden-McAlpine C
Supplementary materials
Supplementary data.
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
Correction notice This article has been updated since it was first published. The article type has been changed to Systematic review.
Contributors PL and MR were responsible for study conception, design and drafting of the manuscript. JC created and tested the research strategy. MG and MMR reviewed and made critical revisions to the paper. MMR supervised the study.
Funding This review was funded by the 'Fundação para a Ciência e Tecnologia (FCT)' Portugal and Merck Sharp & Dohme Portugal (grant number PDE/BDE/120498/2016).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Read the full text or download the PDF:
Two Decades of Academic Service-Learning in Chinese Higher Education: A Review of Research Literature
- Published: 01 May 2024
Cite this article

- Liu Hong ORCID: orcid.org/0000-0002-2250-773X 1 ,
- Yang-yang Wan 1 ,
- Wan-ting Yang 2 ,
- Zhi-jian Gong 1 ,
- Xiao-yue Hu 1 &
- Gaoming Ma 3
Service-learning is globally recognized as an impactful pedagogical approach in higher education. This study reviews literature from the past two decades on university course-based, credit-bearing academic service-learning in the Chinese mainland. It reveals a steady growth in service-learning courses across all regions of the Chinese mainland since 2006, with fifty-two courses documented in the academic literature by 2023. The courses span various disciplines and service populations and have shown positive impacts on university students’ cognitive skills, peer and community connectedness, development of self, disciplinary, and career identities, as well as social responsibility. The study observes the presence of heterogeneous research designs, incomplete reporting of course information, variability in writing styles, structure, and content across different journals and disciplines, indicating an early stage in the field’s development. This underscores the need for systematic documentation of course designs and processes and outcome evaluation with research rigor. The paper discusses the implications for the local development of service-learning practices and the advancement of research in this domain in light of the growing global interest in this educational approach.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price excludes VAT (USA) Tax calculation will be finalised during checkout.
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
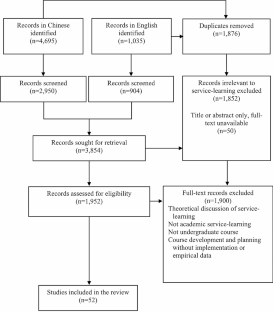
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Anorico, H. C. (2019). Service-learning in the Philippines: The university of Santo Thomas’ national service training program. Gateways: International Journal of Community Research and Engagement , 12 (1). https://doi.org/10.5130/ijcre.v12i1.5944 .
Antonak, R. F., & Harth, R. (1994). Psychometric analysis and revision of the mental retardation attitude inventory. Mental Retardation , 32 (4), 272–280. https://doi.org/10.1007/s003300000751 .
Article Google Scholar
Bennett, D., Sunderland, N., Bartleet, B. L., & Power, A. (2016). Implementing and sustaining higher education service-learning initiatives: Revisiting Young et al.’s organizational tactics. Journal of Experiential Education , 39 (2), 145–163. https://doi.org/10.1177/1053825916629987 .
Billig, S. H. (2009). Does quality really matter: Testing the new K–12 service-learning standards for quality practice. In B. E. Moely, S. H. Billig, & B. A. Holland (Eds.), Creating our identities in service-learning and community engagement (pp. 131–158). Information Age.
Braun, V., & Clarke, V. (2012). Thematic analysis. In H. Cooper, P. M. Camic, D. L. Long, A. T. Panter, D. Rindskopf, & K. J. Sher (Eds.), APA handbook of research methods in psychology, vol 2: Research designs: Quantitative, qualitative, neuropsychological, and biological (pp. 57–71). American Psychological Association. https://doi.org/10.1037/13620-004 .
Bringle, R. G., & Hatcher, J. A. (2000). Institutionalization of service learning in higher education. Journal of Higher Education , 71 (3), 273–290.
Butin, D. W. (2010). Service-learning in theory and practice: The future of community engagement in higher education . Palgrave Macmillan US. https://doi.org/10.1057/9780230106154 .
Celio, C. I., Durlak, J., & Dymnicki, A. (2011). A meta-analysis of the impact of service-learning on students. Journal of Experiential Education , 34 (2), 19. https://doi.org/10.1177/105382591103400205 .
Cen, X. Y., Zhang, H. C., Li, D. Q., Li, R. C., & Zheng, Q. R. (2007). Zai Shequ laonian fuwu zhong chengzhang [Growing in community elderly services]. Shehui Gongzuo Xiabanyue (Lilun) , 12 , 43–44.
Google Scholar
Chen, L. G. (2012). Kecheng daoxiang de shuzihua fuwu xuexi sheji yanjiu [Master’s thesis, Jiangsu Normal University].
Chen, H. L., & Zhang, Y. (2021). Xianshang fuwu xuexi shijian: Yiqing zhong de shehui gongzuo shiwu jiaoyu chengxiao yanjiu [Online service learning practice: A study on the effectiveness of practical social work education during the pandemic]. Shehui Jianshe , 8 (4), 24–35.
Choi, Y., Han, J., & Kim, H. (2023). Exploring key service-learning experiences that promote students’ learning in higher education. Asia Pacific Education Review . https://doi.org/10.1007/s12564-023-09833-5 .
Collins, J., Clark, E., Chau, C., & Pignataro, R. (2019). Impact of an international service learning experience in India for DPT students: Short- and long-term benefits. Journal of Allied Health , 48 (1), 22–30.
Compare, C., & Albanesi, C. (2023). Belief, attitude and critical understanding. A systematic review of social justice in service-learning experiences. Journal of Community & Applied Social Psychology , 33 (2), 332–355. https://doi.org/10.1002/casp.2639 .
Conway, J. M., Amel, E. L., & Gerwien, D. P. (2009). Teaching and learning in the social context: A meta-analysis of service learning’s effects on academic, personal, social, and citizenship outcomes. Teaching of Psychology , 36 (4), 233–245. https://doi.org/10.1080/00986280903172969 .
Dai, X. (2022). Fuwu Xuexi Zai shehui gongzuo kecheng shixi zhong de yunyong ——yi Ge’an Shehui Gongzuo kecheng weili [Application of service learning in social work course internship — case Social Work course as an example]. Zhongguo Shehui Gongzuo , (13) , 30–32.
Dai, K. Y., Hong, L., & Xu, K. (2023). Ti Xian Liang xing Yi Du De Jisuanjilei Fuwu Xuexi Kecheng De Sheji Yu shijian [Design and practice of computer service learning courses reflecting two sexes and one degree]. Ruanjian Daokan , 1–6.
Eyler, J., & Giles, D. E. Jr. (1997). The importance of program quality in service-learning. In A. S. Waterman (Ed.), Service-learning: Applications from the research (pp. 57–76). Lawrence Erlbaum Associates.
Eyler, J., Giles Jr, D. E., Stenson, C. M., & Gray, C. J. (2001). At a glance: What we know about the effects of service-learning on college students, faculty, institutions and communities, 1993–2000. Higher Education , 139.
Faulconer, E. (2021). eService-learning: A decade of research in undergraduate online service–learning. American Journal of Distance Education , 35 (2), 100–117. https://doi.org/10.1080/08923647.2020.1849941 .
Fu, J., & Li, Y. L. (2016). Fuwu Xuexi Dui daxuesheng shehui chengshudu de yingxiang [The impact of service learning on the social maturity of college students]. Guangxi Jiaoyu , 7 , 48–50.
Furco, A. (2007). Institutionalising service-learning in higher education. Higher Education and Civic Engagement: International perspectives . Routledge.
Gao, Z. M. (2016). Fuwu—Xuexi Bentuhua De Tansuo Yu sikao [Exploration and thinking on the localization of service-learning]. Gaojiao Xuekan , 17 , 24–25.
Gonzales, A. D., Harmon, K. S., & Fenn, N. E. (2020). Perceptions of service learning in pharmacy education: A systematic review. Currents in Pharmacy Teaching and Learning , 12 (9), 1150–1161. https://doi.org/10.1016/j.cptl.2020.04.005 .
Gordon, C. S., Pink, M. A., Rosing, H., & Mizzi, S. (2022). A systematic meta-analysis and meta-synthesis of the impact of service-learning programs on university students’ empathy. Educational Research Review , 37 , 100490. https://doi.org/10.1016/j.edurev.2022.100490 .
Guo, Y. Y. (2015). Fuwu-Xuexi xing jiaoxue fangfa zai peiyang shehui gongzuo xuesheng zhuanye nengli fangmian de yunyong yanjiu [Master’s thesis, Yunnan University].
Hammond, C. (1994). Integrating service and academic study: Faculty motivation and satisfaction in Michigan higher education. Michigan Journal of Community Service Learning , 1 (1), 21–28.
Han, Y. M. (2018). Oral history of Sian leprosy rehabilitation village: A service-learning project conducted by South China Normal University. In C. M. Hok-ka, A. C. Cheung-ming, A. L. Cheng, & F. M. Mui-fong (Eds.), Service-learning as a new paradigm in higher education of China (pp. 85–92). Michigan State University.
Harte, A., Persyn, A., Louro, J., de Smet, L., Harvey, K., Laabs, K., Minotti, S., Naujanyte, P., Porkola, R., & Semenski, S. (2019). & others. European student reflections and perspectives on service learning. In Embedding Service Learning in European Higher Education (pp. 196–209). Routledge.
Haski-Leventhal, D., GrÖNlund, H., Holmes, K., Meijs, L. C. P. M., Cnaan, R. A., Handy, F., Brudney, J. L., Hustinx, L., Kang, C., Kassam, M., Pessi, A. B., Ranade, B., Smith, K. A., Yamauchi, N., & Zrinscak, S. (2010). Service-learning: Findings from a 14-Nation study. Journal of Nonprofit & Public Sector Marketing , 22 (3), 161–179. https://doi.org/10.1080/10495141003702332 .
Hawes, J. K., Johnson, R., Payne, L., Ley, C., Grady, C. A., Domenech, J., Evich, C. D., Kanach, A., Koeppen, A., Roe, K., Caprio, A., Puente Castro, J., LeMaster, P., & Blatchley, E. R. (2021). Global service-learning: A systematic review of principles and practices. International Journal of Research on Service-Learning and Community Engagement , 9 (1). https://doi.org/10.37333/001c.31383 .
He, X. J. (2012). Fuwu Xuexi: Shehui gongzuo zhuanye nengli peiyang de guocheng—yici shehui xingzheng kecheng jiaoxue de shijian [Service learning: The process of cultivating social work professional ability—a practice of Social Administration course teaching]. Shehui Gongzuo , 1 , 41–43.
He, L., Zhu, X. Y., & Zhao, S. L. (2015). Fuwu Xuexi Linian Xia De Ketang Xuexi Yu Shequ fuwu—Yi Ertong Quanli Yu Baohu Kecheng Weili [Classroom learning and community service under the concept of service learning—taking children’s rights and Protection course as an example]. Zhongguo Qingnian Shehui Kexue , 34 (4), 93–97.
Holland, B. (1997). Analyzing institutional commitment to service: A model of key organizational factors. Michigan Journal of Community Service Learning , 4 , 30–41.
Hong, L. (2019). An alternative blueprint? Institutionalizing service-learning in a comprehensive university in China. Proceedings of the 3rd International Conference on Service-Learning (pp. 193–196). ICSL 2019
Hong, L., Peng, S. Q., Xu, K., & Chen, Y. (2020). Fuwu xuexi kecheng de sheji: Jiyu sheji siwei de shijian kuangjia [Service-Learning curriculum design: A practical framework based on design thinking]. Fudan Education Forum , 18 (5), 63–70
Hong, Q. N., Pluye, P., Bujold, M., & Wassef, M. (2017). Convergent and sequential synthesis designs: Implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Systematic Reviews , 6 (1), 61. https://doi.org/10.1186/s13643-017-0454-2 .
Honnet, E. P., & Poulsen, S. J. (1989). Wingspread special report: Principles of good practice for combining service and learning . The Johnson Foundation.
Huang, X. R., & Ye, L. H. (2022). Tiyanshi Gongyi De Bentuhua Tansuo Yu Shijian—Yi Huaqiao Daxue Tongshi Kecheng Qiaoai Zhiyuan Fuwu Xiangmu Shequ Fuwu Xuexi Wei Li [Exploration and practice of localizing experiential philanthropy — with the example of Qiao Ai Volunteer Service Community Service Learning of Huaqiao University’s general education course]. Xibu Suzhi Jiaoyu , 8 (4), 4–6.
ICSL 2019 (The 3rd International Conference on Service-Learning). Proceedings of the 3rd International Conference on Service-Learning, Hong Kong Polytechnic University, 10–12 (January, 2019). http://hdl.handle.net/10397/81823 .
Lemieux, C. M., & Allen, P. D. (2007). Service learning in social work education: The state of knowledge, pedagogical practicalities, and practice conundrums. Journal of Social Work Education , 43 (2), 309–326. https://doi.org/10.5175/JSWE.2007.200500548 .
Li, Y. H. (2008). Shehui Gongzuo Shiwu Kecheng Fuwu Xuexi Jiaoxue Moshi tansuo—Yi Laonian Shehui Gongzuo fuwu xuexi xiangmu weili [Exploration of service learning teaching model in social work practical courses: A case study of Elderly Social Work service learning project]. Shehui Gongzuo Xiabanyue (Lilun) , 3 , 18–21.
Li, Z., Wang, Q. Q., & Qi, B. C. (2011). Dangdai daxuesheng zhuanye rentongdu de xianzhuang ji duice yanjiu [Current situation and countermeasures research on contemporary college students’ professional identity]. Gaojiao Tansuo , 2 , 131–136.
Li, Y., Yao, M., Song, F., Fu, J., & Chen, X. (2018). Building a just world: The effects of service-learning on social justice beliefs of Chinese college students. Educational Psychology , 39 (5), 591–616. https://doi.org/10.1080/01443410.2018.1530733 .
Li, H., McDougle, L. M., & Gupta, A. (2019). Experiential philanthropy in China. Journal of Public Affairs Education , 26 (2), 205–227. https://doi.org/10.1080/15236803.2019.1667185 .
Li, L. W., Hou, J. W., & Wei, G. J. (2023). Fuwuxing Xuexi Zai Erke Hulixue kecheng zhong de xingdong yanjiu [Action research on service learning in Pediatric nursing course]. Quanke Huli , 21 (2), 286–288.
Lin, R., & Chen, Y. H. (2022). Jiyu jiji xinlixue de gongyi kecheng shijian de ge’an yanjiu [Case study on the practice of philanthropy courses based on positive psychology]. Yangzhou Daxue Xuebao (Gaojiao Yanjiuban) , 25 (4), 103–110.
Lin, P., & Huang, W. (2013). Fuwu Xuexi Linian Yingyong Yu wuli shifan jiaoyu de shijian [Application of service learning concept in physics normal education practice]. Hezhou Xueyuan Xuebao , 29 (1), 130–132.
Lin, Y., & Jiang, A. L. (2004). Huli zhuanye daxuesheng zizhu xuexi nengli ceping liangbiao de yanzhi [Development of the self-directed learning ability assessment scale for nursing college students]. Jiefangjun huli Zazhi , 6 , 1–4.
Liu, N., Yang, Y. Y., Dong, Z. G., Zhang, Y. Y., & Xu, Y. (2015). Husheng canjia Laonian Hulixue kecheng fuwuxing xuexi de tiyan ji fansi [Nursing students’ experience and reflection on service learning in geriatric nursing course]. Jiefangjun Huli Zazhi , 32 (7), 6–9.
Liu, J. E., Fan, G. H., Xu, L. S., Lin, X. Y., Zhang, A. Q., Huang, W. H., Zheng, S. Y., Zeng, Y., & Yang, M. H. (2021). Shantou Daxue Yixueyuan Yizhe Zhi Xin (HEART) yixue renwen jiaoyu Moshi Yu Shijian—Yi Yixuesheng Gongyi Zhongzi Peiyu Jihua Wei shijiao [Shantou University Medical College’s HEART medical humanities education model and practice — from the perspective of Medical Student Public Welfare seed cultivation plan]. Yixue Jiaoyu Guanli , 7 (4), 366–372.
Lo, K. W. K., Ngai, G., Chan, S. C. F., & Kwan, K. (2022). How students’ motivation and learning experience affect their service-learning outcomes: A structural equation modeling analysis. Frontiers in Psychology , 13 , 825902. https://doi.org/10.3389/fpsyg.2022.825902 .
Long, L., Wan, Y., Zou, K., Shen, Z. Q., Hao, Y., Zhao, X. Y., Feng, W. T., & Li, J. Y. (2022). Yi Fuwu Xuexi Wei Zhidao Sixiang De Kecheng Sheji Ji Fei Biaozhunhua Kaohe Moshi Tansuo—Yi Yufang Yixue Yu Gonggong Weisheng Fuwu Xuexi Shijian Kecheng Wei Li [Exploration of course design and non-standard assessment model guided by service learning — taking the Practice Course of Preventive Medicine and Public Health Service Learning as an example]. Xiandai Yufang Yixue , 49 (22), 4221–4224.
Ma, Y. J. (2020). Fuwu Xuexi Yanjiu: Yi Xinguan feiyan yiqing zhong Tiyanshi Cishan jiaoxue shijian weili [Service learning research: Taking Experiential Philanthropy teaching practice in COVID-19 as an example]. Gaodeng Jiaoyu Yanjiu , 41 (9), 93–102.
Marco-Gardoqui, M., Eizaguirre, A., & García-Feijoo, M. (2020). The impact of service-learning methodology on business schools’ students worldwide: A systematic literature review. Plos One , 15 (12), e0244389. https://doi.org/10.1371/journal.pone.0244389 .
Mashino, T. (2022). Not for democracy? Service-learning in Japanese higher education as compared to the United States. Educational Studies in Japan , 16 (0), 59–70. https://doi.org/10.7571/esjkyoiku.16.59 .
McIlrath, L., Aramburuzabala, P., & Opazo, H. (2019). Developing a culture of civic engagement through service learning within higher education in Europe. In P. Aramburuzabala, L. McIlrath, & H. Opazo (Eds.), Embedding Service Learning in European Higher Education: Developing a culture of Civic Engagement (pp. 69–80). Routledge.
Meijs, L. C., Maas, S. A., & Aramburuzabala, P. (2019). Institutionalisation of service learning in European higher education. In P. Aramburuzabala, L. McIlrath, & H. Opazo (Eds.), Embedding service learning in European higher education (pp. 213–229). Routledge.
Moely, B. E., & Ilustre, V. (2014). The impact of service-learning course characteristics on university students’ learning outcomes. Michigan Journal of Community Service Learning , 21 (1), 5–16. https://doi.org/10.3382/ps.0680287 .
Moely, B. E., Mercer, S. H., Ilustre, V., Miron, D., & McFarland, M. (2002). Psychometric properties and correlates of the Civic attitudes and skills Questionnaire (CASQ): A measure of students’ attitudes related to service-learning. Michigan Journal of Community Service Learning , 8 , 15–26. http://hdl.handle.net/2027/spo.3239521.0008.202 .
Mouton, J., & Wildschut, L. (2005). Service learning in South Africa: Lessons learnt through systematic evaluation. Acta Academica, sup-3 , 116–150.
Natarajarathinam, M., Qiu, S., & Lu, W. (2021). Community engagement in engineering education: A systematic literature review. Journal of Engineering Education , 110 (4), 1049–1077. https://doi.org/10.1002/jee.20424 .
Peng, H. M., Chen, X. F., & Gao, Y. X. (2009). Fuwu Xuexi: Qingnian Zhiyuan Fuwu Yu Daxue Jiaoyu Zhenghe Moshi yanjiu [Service learning: A study on the integration of youth volunteer service and university education]. Zhongguo Qingnian Yanjiu , 4 , 87–91.
Pérez-Ordás, R., Nuviala, A., Grao-Cruces, A., & Fernández-Martínez, A. (2021). Implementing service-learning programs in physical education; teacher education as teaching and learning models for all the agents involved: A systematic review. International Journal of Environmental Research and Public Health , 18 (2), 669. https://doi.org/10.3390/ijerph18020669 .
Preradović, N. M., & Mažeikienė, N. (2019). Service learning in post-communist countries: Lithuania and Croatia. Embedding Service Learning in European Higher Education (pp. 180–195). Routledge.
Qiu, X. (2013). Lun Fuwu Xuexi Moshi Zai Shehui Xingzheng shijian jiaoxue zhong de yunyong [On the application of service learning model in the practical teaching of Social Administration]. Heihe Xuekan , 5 , 125–126.
Queiruga-Dios, M., Santos Sánchez, M. J., Queiruga-Dios, M. Á., Castellanos, A., P. M., & Queiruga-Dios, A. (2021). Assessment methods for service-learning projects in engineering in higher education: A systematic review. Frontiers in Psychology , 12 , 629231. https://doi.org/10.3389/fpsyg.2021.629231 .
Salam, M., Awang Iskandar, D. N., Ibrahim, D. H. A., & Farooq, M. S. (2019). Service learning in higher education: A systematic literature review. Asia Pacific Education Review , 20 (4), 573–593. https://doi.org/10.1007/s12564-019-09580-6 .
Sandelowski, M., Voils, C. I., & Barroso, J. (2006). Defining and designing mixed research synthesis studies. Research in the Schools , 13 (1), 29–40.
Shek, D. T. L., Siu, A. M. H., & Lee, T. Y. (2007). The Chinese positive youth development scale: A validation study. Research on Social Work Practice , 17 (3), 380–391. https://doi.org/10.1177/1049731506296196 .
Shek, D. T. L., Yang, Z., Ma, C. M. S., & Chai, C. W. Y. (2021). Subjective outcome evaluation of service-learning by the service recipients: Scale development, normative profiles and predictors. Child Indicators Research , 14 (1), 411–434. https://doi.org/10.1007/s12187-020-09765-1 .
Sigmon, R. (1979). Service-learning: Three principles. Synergist , 8 (1), 9–11.
Song, F. N., & Chen, X. L. (2015). Fuwu Xuexi Dui daxuesheng zhuanye rentong Yu Zhiye Chengshudu De Yingxiang yanjiu [The influence of service learning on college students’ professional identity and vocational maturity]. Guangxi Daxue Xuebao (Zhexue Shehui Kexueban) , 37 (6), 115–119.
Sotelino-Losada, A., Arbués-Radigales, E., García-Docampo, L., & González-Geraldo, J. L. (2021). Service-learning in Europe. Dimensions and understanding from academic publication. Frontiers in Education , 6 , 604825. https://doi.org/10.3389/feduc.2021.604825 .
Stetten, N. E., Black, E. W., Edwards, M., Schaefer, N., & Blue, A. V. (2019). Interprofessional service learning experiences among health professional students: A systematic search and review of learning outcomes. Journal of Interprofessional Education & Practice , 15 , 60–69. https://doi.org/10.1016/j.xjep.2019.02.002 .
Stewart, T., & Wubbena, Z. C. (2015). A systematic review of service-learning in medical education: 1998–2012. Teaching and Learning in Medicine: An International Journal , 27 (2), 115–122. https://doi.org/10.1080/10401334.2015.1011647 .
Sun, Z. W. (2017). Ziran kexue kecheng zhiru fuwu xuexi de moshi tansuo [Exploring the model of integrating service learning into natural science courses]. Presented at the China Association for Higher Education Quality Education Research Branch 2017 Annual Meeting and the Sixth University Quality Education High-level Forum, Nanjing.
Tan, S. Y., & Soo, S. H. J. (2020). Service-learning and the development of student teachers in Singapore. Asia Pacific Journal of Education , 40 (2), 263–276. https://doi.org/10.1080/02188791.2019.1671809 .
Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology , 8 (1), 45. https://doi.org/10.1186/1471-2288-8-45 .
Tijsma, G., Hilverda, F., Scheffelaar, A., Alders, S., Schoonmade, L., Blignaut, N., & Zweekhorst, M. (2020). Becoming productive 21st century citizens: A systematic review uncovering design principles for integrating community service learning into higher education courses. Educational Research , 62 (4), 390–413. https://doi.org/10.1080/00131881.2020.1836987 .
Vergés Bosch, N., Freude, L., & Camps Calvet, C. (2021). Service learning with a gender perspective: Reconnecting service learning with feminist research and pedagogy in sociology. Teaching Sociology , 49 (2), 136–149. https://doi.org/10.1177/0092055X21993465 .
Wang, Y. (2006). Fuwu Xuexi Chutan [Preliminary exploration of service learning]. Shehui Gongzuo , 11 , 51–53.
Wang, J., Zhao, F., & Ge, R. Q. (2011). Fuwu Xuexi Yingyong Yu Gaoxiao Yingyu Jiaoxue Chutan [A preliminary study on the application of service learning in university English teaching]. Sheke Zongheng , 26 (3), 174–175.
Wang, C., Yao, M. L., Li, Y. L., & Guo, F. F. (2014). Fuwu Xuexi Zhong daxuesheng de teshu ertong rongheguan de bianhua: Yingyong butong daoxiang de fansi zhijia [Changes in college students’ inclusion of special children in service learning: Applying different reflection scaffolds]. Zhongguo Teshu Jiaoyu , 8 , 3–8.
Wang, S. S., Liu, Y. L., Lin, C. X., Lu, X., Huang, Z., & Guo, W. (2019a). Fuwu Xuexi Moshi Zai Shequ hulixue jiaoxue zhong de yingyong [Application of service learning model in community nursing teaching]. Hulixue Zazhi , 34 (17), 60–62.
Wang, X. L., Chen, H. Z., & Su, J. (2019b). Fuwuxing Xuexi Zai laonian hulixue shijian jiaoxue Zhong De Tansuo Yu yingyong [Exploration and application of service learning in geriatric nursing practical teaching]. Weisheng Zhiye Jiaoyu , 37 (19), 67–68.
Wang, Y., Hu, Y., Xiang, D., Fu, Y., & Hong, L. (2019). Application of social work supervision model in university service-learning courses in Mainland China: A qualitative study on students’ participation. 7th Asia-pacific regional conference on service-learning . Singapore
Warren, J. L. (2012). Does service-learning increase student learning? A meta-analysis. Michigan Journal of Community Service Learning , 18 (2), 56–61.
Wei, C. (2022). Fuwu Xuexi: Shehui Gongzuo Jiaoxue De Fansi Shijian Yu guanxixing cunzai [Service learning: Reflection on the practice of social work teaching and its relational existence]. Yinshan Xuekan , 35 (1), 95–106.
Weigert, K. M. (1998). Academic service learning: Its meaning and relevance. New Directions for Teaching & Learning , 1998 (73), 3–10. https://doi.org/10.1002/tl.7301 .
Wu, B. (2020). Fuwu Xuexi jiaoxuefa de yici xingdong tansuo [An action exploration of service learning teaching method]. Jiaoyu Xueshu Yuekan , 1 , 95–105.
Wu, L. P., Chen, X. Q., & Xu, J. Z. (2015). Yi Kecheng Wei zaiti de fuwuxing xuexi moshi tansuo [Exploration of service learning model with course as carrier]. Xiandai Yiyao Weisheng , 31 (15), 2378–2380.
Xing, J., & Ma, C. H. K. (2010). Service-learning in Asia: Curricular models and practices . Hong Kong University.
Xu, W. (2015). Fuwu Xuexi Yunyong Yu daxuesheng zhiyuan fuwu Zhong De Chengxiao chutan—Yi Zhuhai Mou gaoxiao zhiyuan huodong kecheng weili [A preliminary exploration of the effectiveness of service learning in college students’ volunteer service—taking the volunteer activity course of a university in Zhuhai as an example]. Qingshaonian Yanjiu Yu Shijian , 30 (3), 77–81.
Xu, L. L. (2022). Jiyu fuwu xuexi de Laonian Shehui Gongzuo kecheng shijian jiaoxue moshi tanxi [Exploration of practical teaching mode of Elderly Social Work course based on service learning]. Sudu , 21 , 175–177.
Yao, D., & Xiao, X. L. (2017). Zai shequ ketang xunlian zizhu xuexi nengli—jianzhuxue benke fuwu xuexi kecheng tansuo [Training self-study ability in community classroom—exploration of undergraduate service learning course in architecture]. Zhongguo Jianzhu Jiaoyu , Z1 , 112–117.
Yao, J., Pan, A. Q., & Yang, Y. (2017). Suzhi Jiaoyu Yu Tongshi Jiaoyu Lilun Dui Zhiyuan Fuwu Xuexi Kecheng De qifa—Yi tianjin mou gaoxiao weili [The enlightenment of quality education and general education theory to volunteer service learning course—taking a university in Tianjin as an example]. Xibu Suzhi Jiaoyu , 3 (6), 83–85.
Yao, Q. L., Hu, H., & Zheng, T. Y. (2018). Husheng Dui Zhongyi huli fuwu xuexi shijian jiaoxue moshi de zhenji tiyan [Nursing students’ true experience of traditional Chinese nursing service learning practical teaching model]. Huli Xuebao , 25 (14), 1–4.
Yao, J., Liu, F., Lu, D. D., Guo, Y., & Li, X. W. (2019). Zhuoyue Yixue Jiaoyu Beijing Xia fuwuxing xuexi zai fuchanke hulixue jiaoxue zhong de yingyong [Application of service learning in obstetrics and gynecology nursing teaching under the background of excellent medical education]. Xiandai Yangsheng , 4 , 188–189.
Yorio, P. L., & Ye, F. (2012). A meta-analysis on the effects of service-learning on the social, personal, and cognitive outcomes of learning. Academy of Management Learning & Education , 11 (1), 9–27. https://doi.org/10.5465/amle.2010.0072 .
Yu, X. L., Zhang, J. H., & Liu, S. J. (2020). Fuwu Xuexi Moshi Zai Shehui Gongzuo Rencai Shiwu Nengli Peiyang Zhong De Yunyong—Yi Shequ Gongzuo kecheng weili [Application of service learning model in cultivating practical abilities of social workers — taking Community Work course as an example]. Jingji Yanjiu Daokan , 21 , 145–146.
Yue, S. T., & Liu, L. M. (2019). Fuwuxing xuexi shijiao xia laonian huli shijian jiaoxue Gaige De Tansuo Yu sikao [Exploration and thinking of geriatric nursing practical teaching reform from the perspective of service learning]. Quanke Huli , 17 (24), 3071–3073.
Zhang, C. (2017). Fuwu Xuexi Quxiang De Shehui Gongzuo Jiaoxue Moshi tansuo—Yi Xuexiao Shehui Gongzuo shiwulei kecheng weili [Exploration of social work teaching model oriented by service learning—taking School Social Work practical course as an example]. Tonghua Shifan Xueyuan Xuebao , 38 (12), 96–98.
Zhang, L. J. (2018). Jiyu fuwu xuexi de Laonian Shehui Gongzuo shijian jiaoxue gaige tansuo [Exploration of the practical teaching reform of Elderly Social Work based on service learning]. Gaojiao Luntan , 5 , 30–32.
Zhang, X., & Fan, Y. M. (2014). Jiyu Fuwu Xuexi Moshi De Shengming Jiaoyu Kecheng Sheji Yu shishi—Yi Shantou daxue shengming jiaoyu kecheng weili [Design and implementation of life education curriculum based on service learning model—taking Shantou University life education curriculum as an example]. Shandong Qingnian , 3 , 9–10.
Zhang, Y., & Li, H. B. (2018). Jiyu fuwu—xuexi de gaoxiao sixiang zhengzhi lilunke shijian jiaoxue moshi yanjiu [Study on the practical teaching model of ideological and political theory courses in colleges and universities based on service—learning]. Dangdai Zhongguo Makesi Zhuyi Pinglun , 2 , 179–185.
Zhang, Z. Y., Rong, Y., & Guan, Y. J. (2006). Zhongguo daxuesheng zhiye chengshudu liangbiao de Xindu Yu xiaodu [Reliability and validity of the measurement scale of vocational maturity for Chinese college students]. Xinan Daxue Xuebao (Renwen Shehui Kexueban) , 5 , 1–6. https://doi.org/10.13718/j.cnki.xdsk.2006.05.002 .
Zhang, R. X., Hao, S. J., Yuan, Y. M., Wang, J. Q., Zhang, H. L., Fang, J. H., Xia, Z. Y., & Wang, J. (2022). Jiyu Xinxihua Huanjing de fuwuxing xuexi zai zhongyi hulixue kecheng shijian jiaoxue zhong de yingyong [Application of service learning in the practical teaching of traditional Chinese medicine nursing course based on information environment]. Anhui Zhongyiyao Daxue Xuebao , 41 (3), 97–99.
Zhao, R., & Lilly, A. G. (2022). The role of state mobilization for volunteerism in China. Nonprofit and Voluntary Sector Quarterly , 51 (6), 1304–1323. https://doi.org/10.1177/08997640211057458 .
Zhou, Z., Mu, L., Qi, S., & Shek, D. T. L. (2022). Service leadership through serving minority adolescents in rural China using a rural version of a positive youth development program. Applied Research in Quality of Life , 1–23. https://doi.org/10.1007/s11482-022-10098-0 .
Zhu, J. G. (2020). Fuwu Xuexi: Shehui gongzuo jiaoyu de tongshihua [Service learning: The generalization of social work education]. Xuehai , 1 , 113–118.
Zhu, Y. Z., Ma, L. Y., & Cao, X. Y. (2020). Nixiang Sheji Kuangjia Xia De Fuwu Xuexi Kecheng Shishi Tansuo—Yi Huiben Yingyu Jiaoxue Shijian kecheng weili [Exploration of service learning course implementation under the framework of reverse design — taking the Picture Book English teaching practice course as an example]. Gaojiao Xuekan , 21 , 106–108.
Zhu, Z., Xing, W., Liang, Y., Hong, L., & Hu, Y. (2022). Nursing students’ experiences with service learning: A qualitative systematic review and meta-synthesis. Nurse Education Today , 108 , 105206. https://doi.org/10.1016/j.nedt.2021.105206 .
Zhuang, J. Y., Hu, R., Chen, Y. M., & Shen, L. (2016). Fuwuxing xuexi zai shequ hulixue shijian jiaoxue zhong de yingyong [The application of service learning in community nursing practice teaching]. Zhonghua Huli Jiaoyu , 13 (4), 287–290.
Download references
This research received no funding.
Author information
Authors and affiliations.
School of Social Development and Public Policy, Fudan University, Shanghai, China
Liu Hong, Yang-yang Wan, Zhi-jian Gong & Xiao-yue Hu
Lexium Centre for Innovation and Public Purpose, Shanghai, China
Wan-ting Yang
Center of Social Welfare and Governance, Department of Social Welfare and Risk Management, School of Public Affairs, Zhejiang University, Zijingang Campus, No. 866 Yuhangtang Road, City of Hangzhou, Zhejiang Province, China
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Gaoming Ma .
Ethics declarations
Conflict of interest.
All authors declare no conflict of interest.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Hong, L., Wan, Yy., Yang, Wt. et al. Two Decades of Academic Service-Learning in Chinese Higher Education: A Review of Research Literature. Applied Research Quality Life (2024). https://doi.org/10.1007/s11482-024-10318-9
Download citation
Received : 31 July 2023
Accepted : 19 April 2024
Published : 01 May 2024
DOI : https://doi.org/10.1007/s11482-024-10318-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Academic service-learning
- Literature review
- Higher education
- Positive youth development
- Find a journal
- Publish with us
- Track your research
IMAGES
VIDEO
COMMENTS
Examples of literature reviews. Step 1 - Search for relevant literature. Step 2 - Evaluate and select sources. Step 3 - Identify themes, debates, and gaps. Step 4 - Outline your literature review's structure. Step 5 - Write your literature review.
Literature reviews are in great demand in most scientific fields. Their need stems from the ever-increasing output of scientific publications .For example, compared to 1991, in 2008 three, eight, and forty times more papers were indexed in Web of Science on malaria, obesity, and biodiversity, respectively .Given such mountains of papers, scientists cannot be expected to examine in detail every ...
This article is organized as follows: The next section presents the methodology adopted by this research, followed by a section that discusses the typology of literature reviews and provides empirical examples; the subsequent section summarizes the process of literature review; and the last section concludes the paper with suggestions on how to improve the quality and rigor of literature ...
To understand better how to achieve a good quality literature review, it is helpful to look at the specific processes of the archetypes of literature reviews introduced in Section 2.5; they can also be found in Fig. 3.1, which presents a further classification of the protocol-driven approaches to literature reviews.Even though different archetypes serve different purposes, there are similar ...
A literature review forms the basis for high-quality medical education research and helps maximize relevance, originality, generalizability, and impact. A literature review provides context, informs methodology, maximizes innovation, avoids duplicative research, and ensures that professional standards are met.
Systematic reviews that summarize the available information on a topic are an important part of evidence-based health care. There are both research and non-research reasons for undertaking a literature review. It is important to systematically review the literature when one would like to justify the need for a study, to update personal ...
A literature review is not just about reporting published facts; it requires careful consideration of the published literature to construct an unbiased narrative supported by published evidence. Whilst summarising published findings, it is important for you to add perspective by commenting on the quality of the evidence presented.
The best proposals are timely and clearly explain why readers should pay attention to the proposed topic. It is not enough for a review to be a summary of the latest growth in the literature: the ...
Example: Predictors and Outcomes of U.S. Quality Maternity Leave: A Review and Conceptual Framework: 10.1177/08948453211037398 ; Systematic review: "The authors of a systematic review use a specific procedure to search the research literature, select the studies to include in their review, and critically evaluate the studies they find." (p. 139).
study quality is the systematic literature review, or system-atic review, whose primary task is to evaluate "a field's knowledge claims while recognizing omissions, limits, and untested assumptions" (Rousseau et al., 2008, p. 479). In brief, systematic reviews synthesize evidence, identify gaps
Quality requirements deal with how well a product should perform the intended functionality, such as start-up time and learnability. Researchers argue they are important and at the same time studies indicate there are deficiencies in practice. Our goal is to review the state of evidence for quality requirements. We want to understand the empirical research on quality requirements topics as ...
A literature review is a document or section of a document that collects key sources on a topic and discusses those sources in conversation with each other (also called synthesis ). The lit review is an important genre in many disciplines, not just literature (i.e., the study of works of literature such as novels and plays).
Context: Quality Assessment (QA) of reviewed literature is paramount to a Systematic Literature Review (SLR) as the quality of conclusions completely depends on the quality of selected literature.A number of researchers in Software Engineering (SE) have developed a variety of QA instruments and also reported their challenges. We previously conducted a tertiary study on SLRs with QA from 2004 ...
This is why the literature review as a research method is more relevant than ever. Traditional literature reviews often lack thoroughness and rigor and are conducted ad hoc, rather than following a specific methodology. Therefore, questions can be raised about the quality and trustworthiness of these types of reviews.
In step 6 you will evaluate the articles you included in your review for quality and bias. To do so, you will: Use quality assessment tools to grade each article. Create a summary of the quality of literature included in your review. This page has links to quality assessment tools you can use to evaluate different study types.
the literature review easier to understand; a partial list of them can be found in Table 1. Organize Key Ideas The first step in a literature review is to clearly define the researchquestions,hypotheses, qualityimprovement pro-cedures, or a description of the proposed evidence-based practice along with the specific population of interest for
For this review, a comprehensive literature search was performed from many databases using generic search terms such as Qualitative Research, Criteria, etc. The following databases were chosen for the literature search based on the high number of results: IEEE Explore, ScienceDirect, PubMed, Google Scholar, and Web of Science.
One platform for judging study quality is the systematic literature review, or systematic review, whose primary task is to evaluate "a field's knowledge claims while ... (2008). Undertaking a structured literature review or structuring a literature review: Tales from the field. The Electronic Journal of Business Research Methods, 6(2 ...
A literature review can be just a simple summary of the sources, but it usually has an organizational pattern and combines both summary and synthesis. A summary is a recap of the important information of the source, but a synthesis is a re-organization, or a reshuffling, of that information. It might give a new interpretation of old material or ...
Literature Review; Write and Cite. This guide offers information on writing resources, citation style guides, and academic writing expectations and best practices, as well as information on resources related to copyright, fair use, permissions, and open access. Table of Contents .
First, a search using the exact terms ("evidence based quality improvement," "evidence-based quality improvement," or "EBQI") was employed to identify publications published to March 2020 that explicitly refer to EBQI in the title, abstract, or keyword of the publication (i.e., the elements that are searchable in research databases).
Service quality becomes the crucial issue for hospitality industry and the theory of service quality has evolved over long period of time through testing and trials in service sector. .
We conducted a systematic literature review (SLR) to characterize the humanistic (quality of life [QoL]) and economic burden of FD. Methods: Searches were conducted in the Embase, MEDLINE ®, and MEDLINE ® In-Process databases from inception to January 19, 2022. Conference abstracts of specified congresses were manually searched.
Qualitative methods of effect size calculations have been described in the literature,48 49 which was captured in this review by the number of studies that identified each subtheme, with an assigned frequency rating to compare their relative significance. Subthemes were given a frequency rating of A, B, C or D if they were identified by >10, 7 ...
Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology , 18(1), 1-7.
The concept of "quality of life" (QoL) encompasses all aspects of people's standard of living, including economic, social, or health-related factors, ... In this work, we conducted a systematic literature review (SLR) to investigate the contribution of AI to QoL studies. For this, we collected 68 research works published between 2008 and 2022
The review by Gurol-Urganci, de Jongh, Vodopivec-Jamsek, Atun, and Car (2013) on the effects of mobile phone messaging reminders for attendance at healthcare appointments is an illustrative example of a high-quality systematic review with meta-analysis. Missed appointments are a major cause of inefficiency in healthcare delivery with ...
Introduction Caregivers play a major role in providing all the support and care in daily activities for their relatives with dementia. To fully describe the influence of dementia caregiving on family caregivers' life, we conducted a systematic review including caregivers' perceptions about the positive and negative aspects of caring and the expressed factors. Materials and methods We ...
Service-learning is globally recognized as an impactful pedagogical approach in higher education. This study reviews literature from the past two decades on university course-based, credit-bearing academic service-learning in the Chinese mainland. It reveals a steady growth in service-learning courses across all regions of the Chinese mainland since 2006, with fifty-two courses documented in ...