What Is A Case Control Study?
Julia Simkus
Editor at Simply Psychology
BA (Hons) Psychology, Princeton University
Julia Simkus is a graduate of Princeton University with a Bachelor of Arts in Psychology. She is currently studying for a Master's Degree in Counseling for Mental Health and Wellness in September 2023. Julia's research has been published in peer reviewed journals.
Learn about our Editorial Process
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
On This Page:
A case-control study is a research method where two groups of people are compared – those with the condition (cases) and those without (controls). By looking at their past, researchers try to identify what factors might have contributed to the condition in the ‘case’ group.

Explanation
A case-control study looks at people who already have a certain condition (cases) and people who don’t (controls). By comparing these two groups, researchers try to figure out what might have caused the condition. They look into the past to find clues, like habits or experiences, that are different between the two groups.
The “cases” are the individuals with the disease or condition under study, and the “controls” are similar individuals without the disease or condition of interest.
The controls should have similar characteristics (i.e., age, sex, demographic, health status) to the cases to mitigate the effects of confounding variables .
Case-control studies identify any associations between an exposure and an outcome and help researchers form hypotheses about a particular population.
Researchers will first identify the two groups, and then look back in time to investigate which subjects in each group were exposed to the condition.
If the exposure is found more commonly in the cases than the controls, the researcher can hypothesize that the exposure may be linked to the outcome of interest.

Figure: Schematic diagram of case-control study design. Kenneth F. Schulz and David A. Grimes (2002) Case-control studies: research in reverse . The Lancet Volume 359, Issue 9304, 431 – 434
Quick, inexpensive, and simple
Because these studies use already existing data and do not require any follow-up with subjects, they tend to be quicker and cheaper than other types of research. Case-control studies also do not require large sample sizes.
Beneficial for studying rare diseases
Researchers in case-control studies start with a population of people known to have the target disease instead of following a population and waiting to see who develops it. This enables researchers to identify current cases and enroll a sufficient number of patients with a particular rare disease.
Useful for preliminary research
Case-control studies are beneficial for an initial investigation of a suspected risk factor for a condition. The information obtained from cross-sectional studies then enables researchers to conduct further data analyses to explore any relationships in more depth.
Limitations
Subject to recall bias.
Participants might be unable to remember when they were exposed or omit other details that are important for the study. In addition, those with the outcome are more likely to recall and report exposures more clearly than those without the outcome.
Difficulty finding a suitable control group
It is important that the case group and the control group have almost the same characteristics, such as age, gender, demographics, and health status.
Forming an accurate control group can be challenging, so sometimes researchers enroll multiple control groups to bolster the strength of the case-control study.
Do not demonstrate causation
Case-control studies may prove an association between exposures and outcomes, but they can not demonstrate causation.
A case-control study is an observational study where researchers analyzed two groups of people (cases and controls) to look at factors associated with particular diseases or outcomes.
Below are some examples of case-control studies:
- Investigating the impact of exposure to daylight on the health of office workers (Boubekri et al., 2014).
- Comparing serum vitamin D levels in individuals who experience migraine headaches with their matched controls (Togha et al., 2018).
- Analyzing correlations between parental smoking and childhood asthma (Strachan and Cook, 1998).
- Studying the relationship between elevated concentrations of homocysteine and an increased risk of vascular diseases (Ford et al., 2002).
- Assessing the magnitude of the association between Helicobacter pylori and the incidence of gastric cancer (Helicobacter and Cancer Collaborative Group, 2001).
- Evaluating the association between breast cancer risk and saturated fat intake in postmenopausal women (Howe et al., 1990).
Frequently asked questions
1. what’s the difference between a case-control study and a cross-sectional study.
Case-control studies are different from cross-sectional studies in that case-control studies compare groups retrospectively while cross-sectional studies analyze information about a population at a specific point in time.
In cross-sectional studies , researchers are simply examining a group of participants and depicting what already exists in the population.
2. What’s the difference between a case-control study and a longitudinal study?
Case-control studies compare groups retrospectively, while longitudinal studies can compare groups either retrospectively or prospectively.
In a longitudinal study , researchers monitor a population over an extended period of time, and they can be used to study developmental shifts and understand how certain things change as we age.
In addition, case-control studies look at a single subject or a single case, whereas longitudinal studies can be conducted on a large group of subjects.
3. What’s the difference between a case-control study and a retrospective cohort study?
Case-control studies are retrospective as researchers begin with an outcome and trace backward to investigate exposure; however, they differ from retrospective cohort studies.
In a retrospective cohort study , researchers examine a group before any of the subjects have developed the disease, then examine any factors that differed between the individuals who developed the condition and those who did not.
Thus, the outcome is measured after exposure in retrospective cohort studies, whereas the outcome is measured before the exposure in case-control studies.
Boubekri, M., Cheung, I., Reid, K., Wang, C., & Zee, P. (2014). Impact of windows and daylight exposure on overall health and sleep quality of office workers: a case-control pilot study. Journal of Clinical Sleep Medicine: JCSM: Official Publication of the American Academy of Sleep Medicine, 10 (6), 603-611.
Ford, E. S., Smith, S. J., Stroup, D. F., Steinberg, K. K., Mueller, P. W., & Thacker, S. B. (2002). Homocyst (e) ine and cardiovascular disease: a systematic review of the evidence with special emphasis on case-control studies and nested case-control studies. International journal of epidemiology, 31 (1), 59-70.
Helicobacter and Cancer Collaborative Group. (2001). Gastric cancer and Helicobacter pylori: a combined analysis of 12 case control studies nested within prospective cohorts. Gut, 49 (3), 347-353.
Howe, G. R., Hirohata, T., Hislop, T. G., Iscovich, J. M., Yuan, J. M., Katsouyanni, K., … & Shunzhang, Y. (1990). Dietary factors and risk of breast cancer: combined analysis of 12 case—control studies. JNCI: Journal of the National Cancer Institute, 82 (7), 561-569.
Lewallen, S., & Courtright, P. (1998). Epidemiology in practice: case-control studies. Community eye health, 11 (28), 57–58.
Strachan, D. P., & Cook, D. G. (1998). Parental smoking and childhood asthma: longitudinal and case-control studies. Thorax, 53 (3), 204-212.
Tenny, S., Kerndt, C. C., & Hoffman, M. R. (2021). Case Control Studies. In StatPearls . StatPearls Publishing.
Togha, M., Razeghi Jahromi, S., Ghorbani, Z., Martami, F., & Seifishahpar, M. (2018). Serum Vitamin D Status in a Group of Migraine Patients Compared With Healthy Controls: A Case-Control Study. Headache, 58 (10), 1530-1540.
Further Information
- Schulz, K. F., & Grimes, D. A. (2002). Case-control studies: research in reverse. The Lancet, 359(9304), 431-434.
- What is a case-control study?
Related Articles

Research Methodology
Discourse Analysis

Phenomenology In Qualitative Research

Ethnography In Qualitative Research

Narrative Analysis In Qualitative Research

Thematic Analysis: A Step by Step Guide

Metasynthesis Of Qualitative Research
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- What Is a Case-Control Study? | Definition & Examples
What Is a Case-Control Study? | Definition & Examples
Published on February 4, 2023 by Tegan George . Revised on June 22, 2023.
A case-control study is an experimental design that compares a group of participants possessing a condition of interest to a very similar group lacking that condition. Here, the participants possessing the attribute of study, such as a disease, are called the “case,” and those without it are the “control.”
It’s important to remember that the case group is chosen because they already possess the attribute of interest. The point of the control group is to facilitate investigation, e.g., studying whether the case group systematically exhibits that attribute more than the control group does.
Table of contents
When to use a case-control study, examples of case-control studies, advantages and disadvantages of case-control studies, other interesting articles, frequently asked questions.
Case-control studies are a type of observational study often used in fields like medical research, environmental health, or epidemiology. While most observational studies are qualitative in nature, case-control studies can also be quantitative , and they often are in healthcare settings. Case-control studies can be used for both exploratory and explanatory research , and they are a good choice for studying research topics like disease exposure and health outcomes.
A case-control study may be a good fit for your research if it meets the following criteria.
- Data on exposure (e.g., to a chemical or a pesticide) are difficult to obtain or expensive.
- The disease associated with the exposure you’re studying has a long incubation period or is rare or under-studied (e.g., AIDS in the early 1980s).
- The population you are studying is difficult to contact for follow-up questions (e.g., asylum seekers).
Retrospective cohort studies use existing secondary research data, such as medical records or databases, to identify a group of people with a common exposure or risk factor and to observe their outcomes over time. Case-control studies conduct primary research , comparing a group of participants possessing a condition of interest to a very similar group lacking that condition in real time.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

Case-control studies are common in fields like epidemiology, healthcare, and psychology.
You would then collect data on your participants’ exposure to contaminated drinking water, focusing on variables such as the source of said water and the duration of exposure, for both groups. You could then compare the two to determine if there is a relationship between drinking water contamination and the risk of developing a gastrointestinal illness. Example: Healthcare case-control study You are interested in the relationship between the dietary intake of a particular vitamin (e.g., vitamin D) and the risk of developing osteoporosis later in life. Here, the case group would be individuals who have been diagnosed with osteoporosis, while the control group would be individuals without osteoporosis.
You would then collect information on dietary intake of vitamin D for both the cases and controls and compare the two groups to determine if there is a relationship between vitamin D intake and the risk of developing osteoporosis. Example: Psychology case-control study You are studying the relationship between early-childhood stress and the likelihood of later developing post-traumatic stress disorder (PTSD). Here, the case group would be individuals who have been diagnosed with PTSD, while the control group would be individuals without PTSD.
Case-control studies are a solid research method choice, but they come with distinct advantages and disadvantages.
Advantages of case-control studies
- Case-control studies are a great choice if you have any ethical considerations about your participants that could preclude you from using a traditional experimental design .
- Case-control studies are time efficient and fairly inexpensive to conduct because they require fewer subjects than other research methods .
- If there were multiple exposures leading to a single outcome, case-control studies can incorporate that. As such, they truly shine when used to study rare outcomes or outbreaks of a particular disease .
Disadvantages of case-control studies
- Case-control studies, similarly to observational studies, run a high risk of research biases . They are particularly susceptible to observer bias , recall bias , and interviewer bias.
- In the case of very rare exposures of the outcome studied, attempting to conduct a case-control study can be very time consuming and inefficient .
- Case-control studies in general have low internal validity and are not always credible.
Case-control studies by design focus on one singular outcome. This makes them very rigid and not generalizable , as no extrapolation can be made about other outcomes like risk recurrence or future exposure threat. This leads to less satisfying results than other methodological choices.
If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Student’s t -distribution
- Normal distribution
- Null and Alternative Hypotheses
- Chi square tests
- Confidence interval
- Quartiles & Quantiles
- Cluster sampling
- Stratified sampling
- Data cleansing
- Reproducibility vs Replicability
- Peer review
- Prospective cohort study
Research bias
- Implicit bias
- Cognitive bias
- Placebo effect
- Hawthorne effect
- Hindsight bias
- Affect heuristic
- Social desirability bias
Prevent plagiarism. Run a free check.
A case-control study differs from a cohort study because cohort studies are more longitudinal in nature and do not necessarily require a control group .
While one may be added if the investigator so chooses, members of the cohort are primarily selected because of a shared characteristic among them. In particular, retrospective cohort studies are designed to follow a group of people with a common exposure or risk factor over time and observe their outcomes.
Case-control studies, in contrast, require both a case group and a control group, as suggested by their name, and usually are used to identify risk factors for a disease by comparing cases and controls.
A case-control study differs from a cross-sectional study because case-control studies are naturally retrospective in nature, looking backward in time to identify exposures that may have occurred before the development of the disease.
On the other hand, cross-sectional studies collect data on a population at a single point in time. The goal here is to describe the characteristics of the population, such as their age, gender identity, or health status, and understand the distribution and relationships of these characteristics.
Cases and controls are selected for a case-control study based on their inherent characteristics. Participants already possessing the condition of interest form the “case,” while those without form the “control.”
Keep in mind that by definition the case group is chosen because they already possess the attribute of interest. The point of the control group is to facilitate investigation, e.g., studying whether the case group systematically exhibits that attribute more than the control group does.
The strength of the association between an exposure and a disease in a case-control study can be measured using a few different statistical measures , such as odds ratios (ORs) and relative risk (RR).
No, case-control studies cannot establish causality as a standalone measure.
As observational studies , they can suggest associations between an exposure and a disease, but they cannot prove without a doubt that the exposure causes the disease. In particular, issues arising from timing, research biases like recall bias , and the selection of variables lead to low internal validity and the inability to determine causality.
Sources in this article
We strongly encourage students to use sources in their work. You can cite our article (APA Style) or take a deep dive into the articles below.
George, T. (2023, June 22). What Is a Case-Control Study? | Definition & Examples. Scribbr. Retrieved June 18, 2024, from https://www.scribbr.com/methodology/case-control-study/
Schlesselman, J. J. (1982). Case-Control Studies: Design, Conduct, Analysis (Monographs in Epidemiology and Biostatistics, 2) (Illustrated). Oxford University Press.
Is this article helpful?

Tegan George
Other students also liked, what is an observational study | guide & examples, control groups and treatment groups | uses & examples, cross-sectional study | definition, uses & examples, what is your plagiarism score.
- En español – ExME
- Em português – EME
Case-control and Cohort studies: A brief overview
Posted on 6th December 2017 by Saul Crandon

Introduction
Case-control and cohort studies are observational studies that lie near the middle of the hierarchy of evidence . These types of studies, along with randomised controlled trials, constitute analytical studies, whereas case reports and case series define descriptive studies (1). Although these studies are not ranked as highly as randomised controlled trials, they can provide strong evidence if designed appropriately.
Case-control studies
Case-control studies are retrospective. They clearly define two groups at the start: one with the outcome/disease and one without the outcome/disease. They look back to assess whether there is a statistically significant difference in the rates of exposure to a defined risk factor between the groups. See Figure 1 for a pictorial representation of a case-control study design. This can suggest associations between the risk factor and development of the disease in question, although no definitive causality can be drawn. The main outcome measure in case-control studies is odds ratio (OR) .
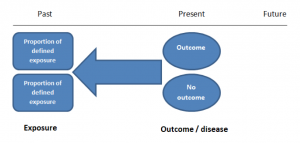
Figure 1. Case-control study design.
Cases should be selected based on objective inclusion and exclusion criteria from a reliable source such as a disease registry. An inherent issue with selecting cases is that a certain proportion of those with the disease would not have a formal diagnosis, may not present for medical care, may be misdiagnosed or may have died before getting a diagnosis. Regardless of how the cases are selected, they should be representative of the broader disease population that you are investigating to ensure generalisability.
Case-control studies should include two groups that are identical EXCEPT for their outcome / disease status.
As such, controls should also be selected carefully. It is possible to match controls to the cases selected on the basis of various factors (e.g. age, sex) to ensure these do not confound the study results. It may even increase statistical power and study precision by choosing up to three or four controls per case (2).
Case-controls can provide fast results and they are cheaper to perform than most other studies. The fact that the analysis is retrospective, allows rare diseases or diseases with long latency periods to be investigated. Furthermore, you can assess multiple exposures to get a better understanding of possible risk factors for the defined outcome / disease.
Nevertheless, as case-controls are retrospective, they are more prone to bias. One of the main examples is recall bias. Often case-control studies require the participants to self-report their exposure to a certain factor. Recall bias is the systematic difference in how the two groups may recall past events e.g. in a study investigating stillbirth, a mother who experienced this may recall the possible contributing factors a lot more vividly than a mother who had a healthy birth.
A summary of the pros and cons of case-control studies are provided in Table 1.
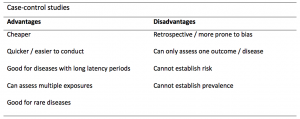
Table 1. Advantages and disadvantages of case-control studies.
Cohort studies
Cohort studies can be retrospective or prospective. Retrospective cohort studies are NOT the same as case-control studies.
In retrospective cohort studies, the exposure and outcomes have already happened. They are usually conducted on data that already exists (from prospective studies) and the exposures are defined before looking at the existing outcome data to see whether exposure to a risk factor is associated with a statistically significant difference in the outcome development rate.
Prospective cohort studies are more common. People are recruited into cohort studies regardless of their exposure or outcome status. This is one of their important strengths. People are often recruited because of their geographical area or occupation, for example, and researchers can then measure and analyse a range of exposures and outcomes.
The study then follows these participants for a defined period to assess the proportion that develop the outcome/disease of interest. See Figure 2 for a pictorial representation of a cohort study design. Therefore, cohort studies are good for assessing prognosis, risk factors and harm. The outcome measure in cohort studies is usually a risk ratio / relative risk (RR).
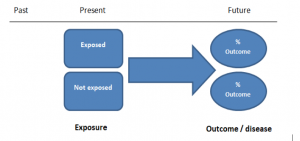
Figure 2. Cohort study design.
Cohort studies should include two groups that are identical EXCEPT for their exposure status.
As a result, both exposed and unexposed groups should be recruited from the same source population. Another important consideration is attrition. If a significant number of participants are not followed up (lost, death, dropped out) then this may impact the validity of the study. Not only does it decrease the study’s power, but there may be attrition bias – a significant difference between the groups of those that did not complete the study.
Cohort studies can assess a range of outcomes allowing an exposure to be rigorously assessed for its impact in developing disease. Additionally, they are good for rare exposures, e.g. contact with a chemical radiation blast.
Whilst cohort studies are useful, they can be expensive and time-consuming, especially if a long follow-up period is chosen or the disease itself is rare or has a long latency.
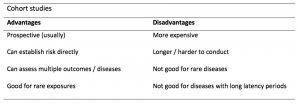
A summary of the pros and cons of cohort studies are provided in Table 2.
The Strengthening of Reporting of Observational Studies in Epidemiology Statement (STROBE)
STROBE provides a checklist of important steps for conducting these types of studies, as well as acting as best-practice reporting guidelines (3). Both case-control and cohort studies are observational, with varying advantages and disadvantages. However, the most important factor to the quality of evidence these studies provide, is their methodological quality.
- Song, J. and Chung, K. Observational Studies: Cohort and Case-Control Studies . Plastic and Reconstructive Surgery.  2010 Dec;126(6):2234-2242.
- Ury HK. Efficiency of case-control studies with multiple controls per case: Continuous or dichotomous data . Biometrics . 1975 Sep;31(3):643–649.
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.  Lancet 2007 Oct;370(9596):1453-14577. PMID: 18064739.

Saul Crandon
Leave a reply cancel reply.
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
No Comments on Case-control and Cohort studies: A brief overview

Very well presented, excellent clarifications. Has put me right back into class, literally!

Very clear and informative! Thank you.

very informative article.

Thank you for the easy to understand blog in cohort studies. I want to follow a group of people with and without a disease to see what health outcomes occurs to them in future such as hospitalisations, diagnoses, procedures etc, as I have many health outcomes to consider, my questions is how to make sure these outcomes has not occurred before the “exposure disease”. As, in cohort studies we are looking at incidence (new) cases, so if an outcome have occurred before the exposure, I can leave them out of the analysis. But because I am not looking at a single outcome which can be checked easily and if happened before exposure can be left out. I have EHR data, so all the exposure and outcome have occurred. my aim is to check the rates of different health outcomes between the exposed)dementia) and unexposed(non-dementia) individuals.

Very helpful information

Thanks for making this subject student friendly and easier to understand. A great help.

Thanks a lot. It really helped me to understand the topic. I am taking epidemiology class this winter, and your paper really saved me.
Happy new year.

Wow its amazing n simple way of briefing ,which i was enjoyed to learn this.its very easy n quick to pick ideas .. Thanks n stay connected

Saul you absolute melt! Really good work man

am a student of public health. This information is simple and well presented to the point. Thank you so much.

very helpful information provided here

really thanks for wonderful information because i doing my bachelor degree research by survival model

Quite informative thank you so much for the info please continue posting. An mph student with Africa university Zimbabwe.

Thank you this was so helpful amazing

Apreciated the information provided above.

So clear and perfect. The language is simple and superb.I am recommending this to all budding epidemiology students. Thanks a lot.

Great to hear, thank you AJ!

I have recently completed an investigational study where evidence of phlebitis was determined in a control cohort by data mining from electronic medical records. We then introduced an intervention in an attempt to reduce incidence of phlebitis in a second cohort. Again, results were determined by data mining. This was an expedited study, so there subjects were enrolled in a specific cohort based on date(s) of the drug infused. How do I define this study? Thanks so much.

thanks for the information and knowledge about observational studies. am a masters student in public health/epidemilogy of the faculty of medicines and pharmaceutical sciences , University of Dschang. this information is very explicit and straight to the point

Very much helpful
Subscribe to our newsletter
You will receive our monthly newsletter and free access to Trip Premium.
Related Articles

Cluster Randomized Trials: Concepts
This blog summarizes the concepts of cluster randomization, and the logistical and statistical considerations while designing a cluster randomized controlled trial.

Expertise-based Randomized Controlled Trials
This blog summarizes the concepts of Expertise-based randomized controlled trials with a focus on the advantages and challenges associated with this type of study.

An introduction to different types of study design
Conducting successful research requires choosing the appropriate study design. This article describes the most common types of designs conducted by researchers.
- Skip to secondary menu
- Skip to main content
- Skip to primary sidebar
Statistics By Jim
Making statistics intuitive
Case Control Study: Definition, Benefits & Examples
By Jim Frost 2 Comments
What is a Case Control Study?
A case control study is a retrospective, observational study that compares two existing groups. Researchers form these groups based on the existence of a condition in the case group and the lack of that condition in the control group. They evaluate the differences in the histories between these two groups looking for factors that might cause a disease.

By evaluating differences in exposure to risk factors between the case and control groups, researchers can learn which factors are associated with the medical condition.
For example, medical researchers study disease X and use a case-control study design to identify risk factors. They create two groups using available medical records from hospitals. Individuals with disease X are in the case group, while those without it are in the control group. If the case group has more exposure to a risk factor than the control group, that exposure is a potential cause for disease X. However, case-control studies establish only correlation and not causation. Be aware of spurious correlations!
Case-control studies are observational studies because researchers do not control the risk factors—they only observe them. They are retrospective studies because the scientists create the case and control groups after the outcomes for the subjects (e.g., disease vs. no disease) are known.
This post explains the benefits and limitations of case-control studies, controlling confounders, and analyzing and interpreting the results. I close with an example case control study showing how to calculate and interpret the results.
Learn more about Experimental Design: Definition, Types, and Examples .
Related posts : Observational Studies Explained and Control Groups in Experiments
Benefits of a Case Control Study
A case control study is a relatively quick and simple design. They frequently use existing patient data, and the experimenters form the groups after the outcomes are known. Researchers do not conduct an experiment. Instead, they look for differences between the case and control groups that are potential risk factors for the condition. Small groups and individual facilities can conduct case-control studies, unlike other more intensive types of experiments.
Case-control studies are perfect for evaluating outbreaks and rare conditions. Researchers simply need to let a sufficient number of known cases accumulate in an established database. The alternative would be to select a large random sample and hope that the condition afflicts it eventually.
A case control study can provide rapid results during outbreaks where the researchers need quick answers. They are ideal for the preliminary investigation phase, where scientists screen potential risk factors. As such, they can point the way for more thorough, time-consuming, and expensive studies. They are especially beneficial when the current state of science knows little about the connection between risk factors and the medical condition. And when you need to identify potential risk factors quickly!
Cohort studies are another type of observational study that are similar to case-control studies, but there are some important differences. To learn more, read my post about Cohort Studies .
Limitations of a Case Control Study
Because case-control studies are observational, they cannot establish causality and provide lower quality evidence than other experimental designs, such as randomized controlled trials . Additionally, as you’ll see in the next section, this type of study is susceptible to confounding variables unless experimenters correctly match traits between the two groups.
A case-control study typically depends on health records. If the necessary data exist in sources available to the researchers, all is good. However, the investigation becomes more complicated if the data are not readily available.
Case-control studies can incorporate biases from the underlying data sources. For example, researchers frequently obtain patient data from hospital records. The population of hospital patients is likely to differ from the general population. Even the control patients are in the hospital for some reason—they likely have serious health problems. Consequently, the subjects in case-control studies are likely to differ from the general population, which reduces the generalizability of the results.
A case-control study cannot estimate incidence or prevalence rates for the disease. The data from these studies do not allow you to calculate the probability of a new person contracting the condition in a given period nor how common it is in the population. This limitation occurs because case-control studies do not use a representative sample.
Case-control studies cannot determine the time between exposure and onset of the medical condition. In fact, case-control studies cannot reliably assess each subject’s exposure to risk factors over time. Longitudinal studies, such as prospective cohort studies, can better make those types of assessment.
Related post : Causation versus Correlation in Statistics
Use Matching to Control Confounders
Because case-control studies are observational studies, they are particularly vulnerable to confounding variables and spurious correlations . A confounder correlates with both the risk factor and the outcome variable. Because observational studies don’t use random assignment to equalize confounders between the case and control groups, they can become unbalanced and affect the results.
Unfortunately, confounders can be the actual cause of the medical condition rather than the risk factor that the researchers identify. If a case-control study does not account for confounding variables, it can bias the results and make them untrustworthy.
Case-control studies typically use trait matching to control confounders. This technique involves selecting study participants for the case and control groups with similar characteristics, which helps equalize the groups for potential confounders. Equalizing confounders limits their impact on the results.
Ultimately, the goal is to create case and control groups that have equal risks for developing the condition/disease outside the risk factors the researchers are explicitly assessing. Matching facilitates valid comparisons between the two groups because the controls are similar to cases. The researchers use subject-area knowledge to identify characteristics that are critical to match.
Note that you cannot assess matching variables as potential risk factors. You’ve intentionally equalized them across the case and control groups and, consequently, they do not correlate with the condition. Hence, do not use the risk factors you want to evaluate as trait matching variables.
Learn more about confounding variables .
Statistical Analysis of a Case Control Study
Researchers frequently include two controls for each case to increase statistical power for a case-control study. Adding even more controls per case provides few statistical benefits, so studies usually do not use more than a 2:1 control to case ratio.
For statistical results, case-control studies typically produce an odds ratio for each potential risk factor. The equation below shows how to calculate an odds ratio for a case-control study.

Notice how this ratio takes the exposure odds in the case group and divides it by the exposure odds in the control group. Consequently, it quantifies how much higher the odds of exposure are among cases than the controls.
In general, odds ratios greater than one flag potential risk factors because they indicate that exposure was higher in the case group than in the control group. Furthermore, higher ratios signify stronger associations between exposure and the medical condition.
An odds ratio of one indicates that exposure was the same in the case and control groups. Nothing to see here!
Ratios less than one might identify protective factors.
Learn more about Understanding Ratios .
Now, let’s bring this to life with an example!
Example Odds Ratio in a Case-Control Study
The Kent County Health Department in Michigan conducted a case-control study in 2005 for a company lunch that produced an outbreak of vomiting and diarrhea. Out of multiple lunch ingredients, researchers found the following exposure rates for lettuce consumption.
| 53 | 33 | |
| 1 | 7 |
By plugging these numbers into the equation, we can calculate the odds ratio for lettuce in this case-control study.

The study determined that the odds ratio for lettuce is 11.2.
This ratio indicates that those with symptoms were 11.2 times more likely to have eaten lettuce than those without symptoms. These results raise a big red flag for contaminated lettuce being the culprit!
Learn more about Odds Ratios.
Epidemiology in Practice: Case-Control Studies (NIH)
Interpreting Results of Case-Control Studies (CDC)
Share this:

Reader Interactions

January 18, 2022 at 7:56 am
Great post, thanks for writing it!
Is it possible to test an odds ration for statistical significance?

January 18, 2022 at 7:41 pm
Hi Michael,
Thanks! And yes, you can test for significance. To learn more about that, read my post about odds ratios , where I discuss p-values and confidence intervals.
Comments and Questions Cancel reply
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.

StatPearls [Internet].
Case control studies.
Steven Tenny ; Connor C. Kerndt ; Mary R. Hoffman .
Affiliations
Last Update: March 27, 2023 .
- Introduction
A case-control study is a type of observational study commonly used to look at factors associated with diseases or outcomes. [1] The case-control study starts with a group of cases, which are the individuals who have the outcome of interest. The researcher then tries to construct a second group of individuals called the controls, who are similar to the case individuals but do not have the outcome of interest. The researcher then looks at historical factors to identify if some exposure(s) is/are found more commonly in the cases than the controls. If the exposure is found more commonly in the cases than in the controls, the researcher can hypothesize that the exposure may be linked to the outcome of interest.
For example, a researcher may want to look at the rare cancer Kaposi's sarcoma. The researcher would find a group of individuals with Kaposi's sarcoma (the cases) and compare them to a group of patients who are similar to the cases in most ways but do not have Kaposi's sarcoma (controls). The researcher could then ask about various exposures to see if any exposure is more common in those with Kaposi's sarcoma (the cases) than those without Kaposi's sarcoma (the controls). The researcher might find that those with Kaposi's sarcoma are more likely to have HIV, and thus conclude that HIV may be a risk factor for the development of Kaposi's sarcoma.
There are many advantages to case-control studies. First, the case-control approach allows for the study of rare diseases. If a disease occurs very infrequently, one would have to follow a large group of people for a long period of time to accrue enough incident cases to study. Such use of resources may be impractical, so a case-control study can be useful for identifying current cases and evaluating historical associated factors. For example, if a disease developed in 1 in 1000 people per year (0.001/year) then in ten years one would expect about 10 cases of a disease to exist in a group of 1000 people. If the disease is much rarer, say 1 in 1,000,0000 per year (0.0000001/year) this would require either having to follow 1,000,0000 people for ten years or 1000 people for 1000 years to accrue ten total cases. As it may be impractical to follow 1,000,000 for ten years or to wait 1000 years for recruitment, a case-control study allows for a more feasible approach.
Second, the case-control study design makes it possible to look at multiple risk factors at once. In the example above about Kaposi's sarcoma, the researcher could ask both the cases and controls about exposures to HIV, asbestos, smoking, lead, sunburns, aniline dye, alcohol, herpes, human papillomavirus, or any number of possible exposures to identify those most likely associated with Kaposi's sarcoma.
Case-control studies can also be very helpful when disease outbreaks occur, and potential links and exposures need to be identified. This study mechanism can be commonly seen in food-related disease outbreaks associated with contaminated products, or when rare diseases start to increase in frequency, as has been seen with measles in recent years.
Because of these advantages, case-control studies are commonly used as one of the first studies to build evidence of an association between exposure and an event or disease.
In a case-control study, the investigator can include unequal numbers of cases with controls such as 2:1 or 4:1 to increase the power of the study.
Disadvantages and Limitations
The most commonly cited disadvantage in case-control studies is the potential for recall bias. [2] Recall bias in a case-control study is the increased likelihood that those with the outcome will recall and report exposures compared to those without the outcome. In other words, even if both groups had exactly the same exposures, the participants in the cases group may report the exposure more often than the controls do. Recall bias may lead to concluding that there are associations between exposure and disease that do not, in fact, exist. It is due to subjects' imperfect memories of past exposures. If people with Kaposi's sarcoma are asked about exposure and history (e.g., HIV, asbestos, smoking, lead, sunburn, aniline dye, alcohol, herpes, human papillomavirus), the individuals with the disease are more likely to think harder about these exposures and recall having some of the exposures that the healthy controls.
Case-control studies, due to their typically retrospective nature, can be used to establish a correlation between exposures and outcomes, but cannot establish causation . These studies simply attempt to find correlations between past events and the current state.
When designing a case-control study, the researcher must find an appropriate control group. Ideally, the case group (those with the outcome) and the control group (those without the outcome) will have almost the same characteristics, such as age, gender, overall health status, and other factors. The two groups should have similar histories and live in similar environments. If, for example, our cases of Kaposi's sarcoma came from across the country but our controls were only chosen from a small community in northern latitudes where people rarely go outside or get sunburns, asking about sunburn may not be a valid exposure to investigate. Similarly, if all of the cases of Kaposi's sarcoma were found to come from a small community outside a battery factory with high levels of lead in the environment, then controls from across the country with minimal lead exposure would not provide an appropriate control group. The investigator must put a great deal of effort into creating a proper control group to bolster the strength of the case-control study as well as enhance their ability to find true and valid potential correlations between exposures and disease states.
Similarly, the researcher must recognize the potential for failing to identify confounding variables or exposures, introducing the possibility of confounding bias, which occurs when a variable that is not being accounted for that has a relationship with both the exposure and outcome. This can cause us to accidentally be studying something we are not accounting for but that may be systematically different between the groups.
The major method for analyzing results in case-control studies is the odds ratio (OR). The odds ratio is the odds of having a disease (or outcome) with the exposure versus the odds of having the disease without the exposure. The most straightforward way to calculate the odds ratio is with a 2 by 2 table divided by exposure and disease status (see below). Mathematically we can write the odds ratio as follows.
Odds ratio = [(Number exposed with disease)/(Number exposed without disease) ]/[(Number not exposed to disease)/(Number not exposed without disease) ]
This can be rewritten as:
Odds ratio = [ (Number exposed with disease) x (Number not exposed without disease) ] / [ (Number exposed without disease ) x (Number not exposed with disease) ]
The odds ratio tells us how strongly the exposure is related to the disease state. An odds ratio of greater than one implies the disease is more likely with exposure. An odds ratio of less than one implies the disease is less likely with exposure and thus the exposure may be protective. For example, a patient with a prior heart attack taking a daily aspirin has a decreased odds of having another heart attack (odds ratio less than one). An odds ratio of one implies there is no relation between the exposure and the disease process.
Odds ratios are often confused with Relative Risk (RR), which is a measure of the probability of the disease or outcome in the exposed vs unexposed groups. For very rare conditions, the OR and RR may be very similar, but they are measuring different aspects of the association between outcome and exposure. The OR is used in case-control studies because RR cannot be estimated; whereas in randomized clinical trials, a direct measurement of the development of events in the exposed and unexposed groups can be seen. RR is also used to compare risk in other prospective study designs.
- Issues of Concern
The main issues of concern with a case-control study are recall bias, its retrospective nature, the need for a careful collection of measured variables, and the selection of an appropriate control group. [3] These are discussed above in the disadvantages section.
- Clinical Significance
A case-control study is a good tool for exploring risk factors for rare diseases or when other study types are not feasible. Many times an investigator will hypothesize a list of possible risk factors for a disease process and will then use a case-control study to see if there are any possible associations between the risk factors and the disease process. The investigator can then use the data from the case-control study to focus on a few of the most likely causative factors and develop additional hypotheses or questions. Then through further exploration, often using other study types (such as cohort studies or randomized clinical studies) the researcher may be able to develop further support for the evidence of the possible association between the exposure and the outcome.
- Enhancing Healthcare Team Outcomes
Case-control studies are prevalent in all fields of medicine from nursing and pharmacy to use in public health and surgical patients. Case-control studies are important for each member of the health care team to not only understand their common occurrence in research but because each part of the health care team has parts to contribute to such studies. One of the most important things each party provides is helping identify correct controls for the cases. Matching the controls across a spectrum of factors outside of the elements of interest take input from nurses, pharmacists, social workers, physicians, demographers, and more. Failure for adequate selection of controls can lead to invalid study conclusions and invalidate the entire study.
- Review Questions
- Access free multiple choice questions on this topic.
- Comment on this article.
2x2 table with calculations for the odds ratio and 95% confidence interval for the odds ratio Contributed by Steven Tenny MD, MPH, MBA
Disclosure: Steven Tenny declares no relevant financial relationships with ineligible companies.
Disclosure: Connor Kerndt declares no relevant financial relationships with ineligible companies.
Disclosure: Mary Hoffman declares no relevant financial relationships with ineligible companies.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
- Cite this Page Tenny S, Kerndt CC, Hoffman MR. Case Control Studies. [Updated 2023 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
In this Page
Bulk download.
- Bulk download StatPearls data from FTP
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Similar articles in PubMed
- Suicidal Ideation. [StatPearls. 2024] Suicidal Ideation. Harmer B, Lee S, Rizvi A, Saadabadi A. StatPearls. 2024 Jan
- Qualitative Study. [StatPearls. 2024] Qualitative Study. Tenny S, Brannan JM, Brannan GD. StatPearls. 2024 Jan
- Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas. [Cochrane Database Syst Rev. 2022] Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas. Crider K, Williams J, Qi YP, Gutman J, Yeung L, Mai C, Finkelstain J, Mehta S, Pons-Duran C, Menéndez C, et al. Cochrane Database Syst Rev. 2022 Feb 1; 2(2022). Epub 2022 Feb 1.
- Review The epidemiology of classic, African, and immunosuppressed Kaposi's sarcoma. [Epidemiol Rev. 1991] Review The epidemiology of classic, African, and immunosuppressed Kaposi's sarcoma. Wahman A, Melnick SL, Rhame FS, Potter JD. Epidemiol Rev. 1991; 13:178-99.
- Review Epidemiology of Kaposi's sarcoma. [Cancer Surv. 1991] Review Epidemiology of Kaposi's sarcoma. Beral V. Cancer Surv. 1991; 10:5-22.
Recent Activity
- Case Control Studies - StatPearls Case Control Studies - StatPearls
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
Study Design 101: Case Control Study
- Case Report
- Case Control Study
- Cohort Study
- Randomized Controlled Trial
- Practice Guideline
- Systematic Review
- Meta-Analysis
- Helpful Formulas
- Finding Specific Study Types
A study that compares patients who have a disease or outcome of interest (cases) with patients who do not have the disease or outcome (controls), and looks back retrospectively to compare how frequently the exposure to a risk factor is present in each group to determine the relationship between the risk factor and the disease.
Case control studies are observational because no intervention is attempted and no attempt is made to alter the course of the disease. The goal is to retrospectively determine the exposure to the risk factor of interest from each of the two groups of individuals: cases and controls. These studies are designed to estimate odds.
Case control studies are also known as "retrospective studies" and "case-referent studies."
- Good for studying rare conditions or diseases
- Less time needed to conduct the study because the condition or disease has already occurred
- Lets you simultaneously look at multiple risk factors
- Useful as initial studies to establish an association
- Can answer questions that could not be answered through other study designs
Disadvantages
- Retrospective studies have more problems with data quality because they rely on memory and people with a condition will be more motivated to recall risk factors (also called recall bias).
- Not good for evaluating diagnostic tests because it's already clear that the cases have the condition and the controls do not
- It can be difficult to find a suitable control group
Design pitfalls to look out for
Care should be taken to avoid confounding, which arises when an exposure and an outcome are both strongly associated with a third variable. Controls should be subjects who might have been cases in the study but are selected independent of the exposure. Cases and controls should also not be "over-matched."
Is the control group appropriate for the population? Does the study use matching or pairing appropriately to avoid the effects of a confounding variable? Does it use appropriate inclusion and exclusion criteria?
Fictitious Example
There is a suspicion that zinc oxide, the white non-absorbent sunscreen traditionally worn by lifeguards is more effective at preventing sunburns that lead to skin cancer than absorbent sunscreen lotions. A case-control study was conducted to investigate if exposure to zinc oxide is a more effective skin cancer prevention measure. The study involved comparing a group of former lifeguards that had developed cancer on their cheeks and noses (cases) to a group of lifeguards without this type of cancer (controls) and assess their prior exposure to zinc oxide or absorbent sunscreen lotions.
This study would be retrospective in that the former lifeguards would be asked to recall which type of sunscreen they used on their face and approximately how often. This could be either a matched or unmatched study, but efforts would need to be made to ensure that the former lifeguards are of the same average age, and lifeguarded for a similar number of seasons and amount of time per season.
Real-life Examples
Boubekri, M., Cheung, I., Reid, K., Wang, C., & Zee, P. (2014). Impact of windows and daylight exposure on overall health and sleep quality of office workers: a case-control pilot study. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine, 10 (6), 603-611. https://doi.org/10.5664/jcsm.3780
This pilot study explored the impact of exposure to daylight on the health of office workers (measuring well-being and sleep quality subjectively, and light exposure, activity level and sleep-wake patterns via actigraphy). Individuals with windows in their workplaces had more light exposure, longer sleep duration, and more physical activity. They also reported a better scores in the areas of vitality and role limitations due to physical problems, better sleep quality and less sleep disturbances.
Togha, M., Razeghi Jahromi, S., Ghorbani, Z., Martami, F., & Seifishahpar, M. (2018). Serum Vitamin D Status in a Group of Migraine Patients Compared With Healthy Controls: A Case-Control Study. Headache, 58 (10), 1530-1540. https://doi.org/10.1111/head.13423
This case-control study compared serum vitamin D levels in individuals who experience migraine headaches with their matched controls. Studied over a period of thirty days, individuals with higher levels of serum Vitamin D was associated with lower odds of migraine headache.
Related Formulas
- Odds ratio in an unmatched study
- Odds ratio in a matched study
Related Terms
A patient with the disease or outcome of interest.
Confounding
When an exposure and an outcome are both strongly associated with a third variable.
A patient who does not have the disease or outcome.
Matched Design
Each case is matched individually with a control according to certain characteristics such as age and gender. It is important to remember that the concordant pairs (pairs in which the case and control are either both exposed or both not exposed) tell us nothing about the risk of exposure separately for cases or controls.
Observed Assignment
The method of assignment of individuals to study and control groups in observational studies when the investigator does not intervene to perform the assignment.
Unmatched Design
The controls are a sample from a suitable non-affected population.
Now test yourself!
1. Case Control Studies are prospective in that they follow the cases and controls over time and observe what occurs.
a) True b) False
2. Which of the following is an advantage of Case Control Studies?
a) They can simultaneously look at multiple risk factors. b) They are useful to initially establish an association between a risk factor and a disease or outcome. c) They take less time to complete because the condition or disease has already occurred. d) b and c only e) a, b, and c
Evidence Pyramid - Navigation
- Meta- Analysis
- Case Reports
- << Previous: Case Report
- Next: Cohort Study >>

- Last Updated: Sep 25, 2023 10:59 AM
- URL: https://guides.himmelfarb.gwu.edu/studydesign101

- Himmelfarb Intranet
- Privacy Notice
- Terms of Use
- GW is committed to digital accessibility. If you experience a barrier that affects your ability to access content on this page, let us know via the Accessibility Feedback Form .
- Himmelfarb Health Sciences Library
- 2300 Eye St., NW, Washington, DC 20037
- Phone: (202) 994-2850
- [email protected]
- https://himmelfarb.gwu.edu
Case–Control Study
- First Online: 13 December 2023
Cite this chapter

- Noraini Abdul Ghafar 2
594 Accesses
A case–control study is an observational study designed to determine if a risk factor is associated with an outcome of interest (disease or condition). This study design permits the researcher to determine if an exposure is associated with an outcome. First, a group with the outcome of interest (“cases”) is identified. Next, a group similar to cases (“controls”) is selected from the “study base” that yielded the cases but without the outcome of interest. Matching of cases and controls on certain characteristics ensures similarity and increases study efficiency. Historical risk factors in both groups are evaluated to determine whether some RFs occur more frequently in cases than controls. Case–control studies may establish an association between a risk factor and outcome but cannot demonstrate causation because of its retrospective nature. Compared to other study designs, case–control studies are inexpensive, quick, and allow the evaluation of several risk factors. Case–control study designs are useful for studying rare diseases, diseases with long latent periods, and for outbreak investigations. Limitations include selection bias and recall bias. Among the strategies to overcome selection bias include an appropriate sampling method, matching, using a minimum of two control groups, and drawing both cases and controls from the same population. Meanwhile, recall bias could be minimized by blinding.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Similar content being viewed by others

Case Control Studies

Level III Evidence: A Case-Control Study

Epidemiological Studies
Lewallen S, Courtright P. Epidemiology in practice: case-control studies. Community Eye Health. 1998;11(28):57–8. PMID: 17492047; PMCID: PMC1706071
CAS PubMed PubMed Central Google Scholar
dos Santos Silva I. 1999. Chapter 9: case control studies in cancer epidemiology: principles and methods ISBN-13 978–92–832-0405-3.
Google Scholar
Breslow NE. Statistics in epidemiology: the case-control study. J Am Stat Assoc. 1996;91(433):14–28. https://doi.org/10.1080/01621459.1996.10476660 . PMID: 12155399
Article CAS PubMed Google Scholar
Setia MS. Methodology series module 2: case control studies. Indian J Dermatol. 2016;61:146–51.
Article PubMed PubMed Central Google Scholar
Mitra AK. Investigating the types of epidemiologic studies. In: Epidemiology for dummies. 1st ed. Hoboken, New Jersey, United States: Wiley; 2023.
Critchley J. Epidemiology for the uninitiated, 5th ed. J Epidemiol Community Health. 2004;58
Wacholder S, McLaughlin JK, Silverman DT, Mandel JS. Selection of controls in case-control studies. I Principles Am J Epidemiol. 1992;135(9):1019–28. https://doi.org/10.1093/oxfordjournals.aje.a116396 . PMID: 1595688
Hennessy S, Bilker WB, Berlin JA, Strom BL. Factors influencing the optimal control-to-case ratio in matched case-control studies. Am J Epidemiol. 1999;149(2):195–7. https://doi.org/10.1093/oxfordjournals.aje.a009786 . Erratum in: Am J Epidemiol 1999 Mar 1;149(5):489. PMID: 9921965
Sedgwick P. Case-control studies: advantages and disadvantages. BMJ. 2014;3(348):f7707. https://doi.org/10.1136/bmj.f7707 . PMID: 31419845
Article Google Scholar
Sedgwick P. Nested case-control studies: advantages and disadvantages. BMJ (online). 2014;348:g1532. https://doi.org/10.1136/bmj.g1532 .
Sedgwick P. Nested case-control studies. BMJ. 2010;(340):c2582. https://doi.org/10.1136/bmj.c2582 . PMID: 20484347
Ernster. Nested case control studies. Prev Med. 1994;23:587–90.
Langholz B, Clayton D. Sampling strategies in nested case-control studies. Environ Health Perspect. 1994;102 Suppl 8(Suppl 8):47–51. https://doi.org/10.1289/ehp.94102s847 . PMID: 7851330; PMCID: PMC1566552
Tan MM, Ho WK, Yoon SY, Mariapun S, Hasan SN, Lee DS, Hassan T, Lee SY, Phuah SY, Sivanandan K, Ng PP, Rajaram N, Jaganathan M, Jamaris S, Islam T, Rahmat K, Fadzli F, Vijayananthan A, Rajadurai P, See MH, Thong MK, Mohd Taib NA, Yip CH, Teo SH. A case-control study of breast cancer risk factors in 7,663 women in Malaysia. PLoS One. 2018;13(9):e0203469. https://doi.org/10.1371/journal.pone.0203469 . PMID: 30216346; PMCID: PMC6138391
Article CAS PubMed PubMed Central Google Scholar
Ganesh B, Sushama S, Monika S, Suvarna P. A case-control study of risk factors for lung cancer in Mumbai. India Asian Pac J Cancer Prev. 2011;12(2):357–62. PMID: 21545194
CAS PubMed Google Scholar
Xi C, Luo M, Wang T, Wang Y, Wang S, Guo L, Lu C. Association between maternal lifestyle factors and low birth weight in preterm and term births: a case-control study. Reprod Health. 2020;17(1):93. https://doi.org/10.1186/s12978-020-00932-9 .
Shimeles E, Enquselassie F, Aseffa A, Tilahun M, Mekonen A, Wondimagegn G, Hailu T. Risk factors for tuberculosis: a case-control study in Addis Ababa, Ethiopia. PLoS One. 2019;14(4):e0214235. https://doi.org/10.1371/journal.pone.0214235 . PMID: 30939169; PMCID: PMC6445425
Kalra A. The odds ratio: principles and applications. J Pract Cardiovasc Sci. 2016;2:49–51.
Szumilas M. Explaining odds ratios. J Can Acad Child Adolesc Psychiatry. 2010;19(3):227–9. Erratum in: J Can Acad Child Adolesc Psychiatry. 2015 Winter;24(1):58. PMID: 20842279; PMCID: PMC2938757
PubMed PubMed Central Google Scholar
Mann CJ. Observational research methods. Research design II: cohort, cross sectional, and case-control studies. Emerg Med J. 2003;20:54–60.
Song JW, Chung KC. Observational studies: cohort and case-control studies. Plast Reconstr Surg. 2010;126(6):2234–42. https://doi.org/10.1097/PRS.0b013e3181f44abc . PMID: 20697313; PMCID: PMC2998589
Download references
Author information
Authors and affiliations.
School of Health Sciences, Universiti Sains Malaysia (Health Campus), Kubang Kerian, Kelantan, Malaysia
Noraini Abdul Ghafar
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Noraini Abdul Ghafar .
Editor information
Editors and affiliations.
Department of Epidemiology and Biostatistics, Jackson State University, Jackson, MS, USA
Amal K. Mitra
Rights and permissions
Reprints and permissions
Copyright information
© 2024 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter
Ghafar, N.A. (2024). Case–Control Study. In: Mitra, A.K. (eds) Statistical Approaches for Epidemiology. Springer, Cham. https://doi.org/10.1007/978-3-031-41784-9_3
Download citation
DOI : https://doi.org/10.1007/978-3-031-41784-9_3
Published : 13 December 2023
Publisher Name : Springer, Cham
Print ISBN : 978-3-031-41783-2
Online ISBN : 978-3-031-41784-9
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Last updated 20/06/24: Online ordering is currently unavailable due to technical issues. We apologise for any delays responding to customers while we resolve this. For further updates please visit our website: https://www.cambridge.org/news-and-insights/technical-incident
We use cookies to distinguish you from other users and to provide you with a better experience on our websites. Close this message to accept cookies or find out how to manage your cookie settings .
Login Alert
- > Case-Control Studies
- > Introduction to case-control studies

Book contents
- Frontmatter
- 1 Introduction to case-control studies
- 2 The simplest situation
- 3 Matched case-control studies
- 4 A general formulation
- 5 Case-control studies with more than two outcomes
- 6 Special sampling designs
- 7 Nested case-control studies
- 8 Case-subcohort studies
- 9 Misclassification and measurement error
- 10 Synthesis of studies
- Appendix: A theoretical diversion
1 - Introduction to case-control studies
Published online by Cambridge University Press: 05 April 2014
• A case-control study is a retrospective observational study and is an alternative to a prospective observational study. Cases are identified in an underlying population and a comparable control group is sampled.
• In the standard design exposure information is obtained retrospectively, though this is not necessarily the case if the case-control sample is nested within a prospective cohort.
• Prospective studies are not cost effective for rare outcomes. By contrast, in a case-control study the ratio of cases and controls is higher than in the underlying population in order to make more efficient use of resources.
• There are two main types of case-control design; matched and unmatched.
• The odds ratio is the most commonly used measure of association between exposure and outcome in a case-control study.
• Important extensions to the standard case-control design include the explicit incorporation of time into the choice of controls and into the analysis.
Defining a case-control study
Consider a population of interest, for example the general population of the UK, perhaps restricted by gender or age group. We may call a representation of the process by which exposures X and outcomes Y occur in the presence of intrinsic features W the population model . As noted in the Preamble, such a system may be investigated prospectively or retrospectively; see Figure 1.1. In a prospective or cohort study a suitable sample of individuals is chosen to represent the population of interest, values of ( W, X ) are determined and the individuals are followed through time until the outcome Y can be observed.
Access options
Save book to kindle.
To save this book to your Kindle, first ensure [email protected] is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about saving to your Kindle .
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
Find out more about the Kindle Personal Document Service .
- Introduction to case-control studies
- Ruth H. Keogh , London School of Hygiene and Tropical Medicine , D. R. Cox , University of Oxford
- Book: Case-Control Studies
- Online publication: 05 April 2014
- Chapter DOI: https://doi.org/10.1017/CBO9781139094757.004
Save book to Dropbox
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Dropbox .
Save book to Google Drive
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Google Drive .
Case-Control Study: Definition, Real Life Examples
Design of Experiments > Case-Control Study
What is a Case-Control Study?
A case-control study is a retrospective study that looks back in time to find the relative risk between a specific exposure (e.g. second hand tobacco smoke) and an outcome (e.g. cancer). A control group of people who do not have the disease or who did not experience the event is used for comparison. The goal is figure out the relationship between risk factors and disease or outcome and estimate the odds of an individual getting a disease or experiencing an event.
Case-control studies have four main steps:
- The study begins by enrolling people who already have a certain disease or outcome.
- A second control group of similar size is sampled, preferably from a population identical in every way except that they don’t have the disease or condition being studied. They should not be selected because of an exposure status.
- People are asked about their exposure to risk factors.
- Finally, an odds ratio is calculated.
- Non-matched case-control study: this is the simplest form. Find a person with the disease and enroll them in the study. Then enroll a control and determine their exposure status.
- Matched case-control: Find a person with the disease and enroll them in the study. Match the person for some characteristic (e.g. sex, age, weight) with a control. This can eliminate or minimize confounding variables . However, it generally results in a longer study; the more characteristics being “matched”, the longer the study takes.
Advantages and Disadvantages
Advantages A case-control study is often the best choice for rare conditions or diseases . Let’s say 10 people in Duval county in Florida had a particularly rare disease. Random sampling for a cohort study would involve large numbers of people and may not pick up any of the diseased people at all. With a case-control study, all 10 people who have the disease can be identified (assuming they are in a medical database) and enrolled in the study. Random sampling could then be used on the non-diseased population to form the control group. Other Advantages :
- Short term study that doesn’t require waiting for events to happen, as they have already occurred.
- Inexpensive.
- Multiple risk factors can be studied at the same time.
- Quickly establishes associations between risk factors and disease. This can be especially useful with disease outbreaks, as causes can be identified with small sample sizes.
- Stronger than cross-sectional studies for establishing causation.
Disadvantages :
- Control groups can be difficult to find.
- Results can easily be tainted by recall bias , where people with the disease or condition are more likely to remember past details compared to people who don’t have the disease or condition.
- Is weaker than a cohort study for establishing causation.
- Usually not generalizable .
Examples from Real Life
- This study for non-Hodgkin lymphoma found a connection between the disease and inflammatory disorders like Sjögrens, Celiac and rheumatoid arthritis.
- This study investigated how increased consumption of fruits and vegetables protects against Cervical Intraepithelial Neoplasia.
- This INTERHEART study looked at second hand tobacco smoke and increased risk of myocardial infarction.
- Search Menu
- Sign in through your institution
- Supplements
- Cohort Profiles
- Education Corner
- Author Guidelines
- Submission Site
- Open Access
- About the International Journal of Epidemiology
- About the International Epidemiological Association
- Editorial Team
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Dispatch Dates
- Contact the IEA
- Journals on Oxford Academic
- Books on Oxford Academic
Article Contents
Introduction, case–control studies in dynamic populations, case–control studies within cohorts, unity of the concept of density sampling from dynamic populations and sampling from cohorts, discussion: differences with classic case–control teaching, and consequences.
- < Previous
Case–control studies: basic concepts
- Article contents
- Figures & tables
- Supplementary Data
Jan P Vandenbroucke, Neil Pearce, Case–control studies: basic concepts, International Journal of Epidemiology , Volume 41, Issue 5, October 2012, Pages 1480–1489, https://doi.org/10.1093/ije/dys147
- Permissions Icon Permissions
The purpose of this article is to present in elementary mathematical and statistical terms a simple way to quickly and effectively teach and understand case–control studies, as they are commonly done in dynamic populations—without using the rare disease assumption. Our focus is on case–control studies of disease incidence (‘incident case–control studies’); we will not consider the situation of case–control studies of prevalent disease, which are published much less frequently.
Readers of the medical literature were once taught that case–control studies are ‘cohort studies in reverse’, in which persons who developed disease during follow-up are compared with persons who did not. In addition, they were told that the odds ratio calculated from case–control studies is an approximation of the risk ratio or rate ratio, but only if the disease is ‘rare’ (say, if <5% of the population develops disease). These notions are no longer compatible with present-day epidemiological theory of case–control studies which is based on ‘density sampling’. Moreover, a recent survey found that the large majority of case–control studies do not sample cases and control subjects from a cohort with fixed membership; rather, they sample from dynamic populations with variable membership. 1 Of all case–control studies involving incident cases, 82% sampled from a dynamic population; only 18% of studies sampled from a cohort, and only some of these may need the ‘rare disease assumption’ (depending on how the control subjects were sampled). Thus, the ‘rare disease assumption’ is not needed for the large majority of published case–control studies. In addition, different assumptions are needed for case–control studies in dynamic populations and those in cohorts to ensure that the odds ratios are estimates of ratios of incidence rates.
The underlying theory for case–control studies in dynamic populations has been developed in epidemiological and statistical journals and textbooks over several decades, 2–19 and its history has been described. 20 Still, the theory is not well known or well understood outside professional epidemiological and statistical circles. Introductory textbooks of epidemiology often fall back on methods of control sampling, which involve the ‘rare disease assumption’ as it was proposed by Cornfield in 1951, 3 because it seems easier to explain. 1 Moreover, several advanced textbooks or articles depict the different ways of sampling cases and control subjects from the point of view of a cohort with fixed membership. 13 , 18 This reinforces the view of case–control studies as constructed within a cohort, even though this applies to only a small minority of published case–control studies.
The purpose of this article is to present in elementary mathematical and statistical terms a simple way to quickly and effectively teach and understand case–control studies as they are commonly done in dynamic populations––without using the rare disease assumption. Our focus is on case–control studies of disease incidence (‘incident case–control studies’); we will not consider the situation of case–control studies of prevalent disease, which are published much less frequently, 1 except in certain situations as discussed by Pearce 21 (e.g. for diseases such as asthma in which it is difficult to identify incident cases).
The theory of case–control studies in dynamic populations cannot be explained before first going back to the calculation of incidence rates and risks in dynamic populations. In a previous article, we have reviewed the demographic concepts that underpin these calculations. 22 In the current article, these concepts will first be applied to case–control studies involving sampling from dynamic populations. Second, we discuss how to teach the theory in the situation of sampling from a cohort. In the third part, it is explained how these two distinct ways of sampling cases and control subjects can be unified conceptually in the proportional hazards model (Cox regression). Finally, we discuss the consequences of this way of teaching case–control studies for understanding the assumptions behind these studies, and for appropriately designing studies. We propose that the explanation of case–control studies within dynamic populations should become the basis for teaching case–control studies, in both introductory and more advanced courses.
Basic teaching
To understand the application of the basic concepts of incidence rate calculations to case–control studies, we start with the demographic perspective of a dynamic population in which we calculate and compare incidence rates of disease. 22
Suppose that investigators are interested in the effect of oral contraceptive use on the incidence of myocardial infarction among women of reproductive age. They might investigate this in a large town in a particular calendar year (we base this example loosely on one of the first case–control studies that investigated this association 23 ). The time-population structure of the study is depicted in Figure 1 .
The underlying dynamic ‘source’ population of a study of myocardial infarction (MI) and oral contraceptive use. The bold undulating lines show the fluctuating number of users and non-users of oral contraceptives in a population that is in a steady state. The finer lines below it depict individuals who enter and leave the populations of users and non-users. Closed circles indicate cases of MI emanating from the population. For users and non-users separately, an incidence rate (IR) of MI can be calculated. The incidence rate ratio (IRR) can be used to compare the incidence of MI between users and non-users. In the description of the example in the text, the time t was set to one calendar year. Figure adapted from Miettinen 9
In Figure 1 , for the sake of simplicity, imagine that, on average, 120 000 young women of reproductive age (between ages 15 and 45 years) who have never had coronary heart disease (CHD), are living in the town, on each day during the calendar year of investigation. This is a dynamic population: each day, new young women will become 15 years old, others will turn 46, some will leave town and others will come to live in the town, some will develop CHD and be replaced by others who do not have the disease and so forth. Such a population can be safely regarded as being ‘in steady state’. The demographic principle of a steady-state population was explained in our previous article; 22 in brief, it assumes that over a small period, e.g. a calendar year, the number of people in a population is approximately constant from day to day because the population is constantly depleted and replenished at about the same rate. It was also explained why this assumption holds, even if the population is not perfectly in a steady state. 22 Thus, we take it that each day of the year, ∼120 000 women of reproductive age, free of clinically recognized CHD, live in the town. Suppose that, on average, 40 000 women use oral contraceptives and 80 000 do not. Again, these are two dynamic subpopulations that can be regarded as being in a steady state. Women start and stop using oral contraceptives for various reasons and switch from use to non-use and back again. As such, in one calendar year, we have 40 000 woman-years of pill use and 80 000 woman-years of non-use, free of CHD.
Suppose that a group of investigators surveys all coronary care units in the town each week to identify all women, aged 15–45 years, admitted with acute myocardial infarction during that period. When a young woman is admitted, the investigators enquire whether she was on the pill––and whether she had previously had a coronary event (if she had, she is excluded from the study). Suppose that, in total, 12 women were admitted for first myocardial infarction during the year of study: eight pill users and four non-users. That produces an incidence rate of 8/40 000 woman-years among pill users and 4/80 000 woman-years among non-users. The ratio of these incidence rates becomes (8/40 000 woman-years)/(4/80 000 woman-years), which is a rate ratio of 4, indicating that women on the pill have an incidence rate of myocardial infarction that is four times that of those not on the pill.
Transformation to a case–control study
In total, 12 cases arise from the population: eight users and four non-users. Those are the potential cases for a case–control study in which the investigators would survey all coronary care units each week of the year. Suppose that the investigators, as their next step, would take a random sample of 600 control subjects from the total source population of the cases (the total of 120 000), by asking 600 women aged 15–45 years, without previous CHD, whether they are ‘on the pill’ at the time the question is asked. Then, on whatever day of the year, this sample of control subjects will include, on average, 200 users and 400 non-users of oral contraceptives. These numbers represent the underlying distribution of woman-years of users and non-users. Together with the cases, this is the complete case–control study (see Table 1 ).
Layout of case-control data sampled from dynamic population: study of occurrence of myocardial infarction in users vs non-users of oral contraceptives, corresponding to Figure 1
| . | Myocardial infarction . | Control subjects . |
|---|---|---|
| Oral contraceptive use | ||
| Yes | 8 | 200 |
| No | 4 | 400 |
| Odds ratio | 4 | |
| . | Myocardial infarction . | Control subjects . |
|---|---|---|
| Oral contraceptive use | ||
| Yes | 8 | 200 |
| No | 4 | 400 |
| Odds ratio | 4 | |
From Table 1 , an odds ratio can be calculated as (8 × 400)/(4 × 200). This exactly equals the ratio of the incidence rates in the underlying population. Algebraically: the incidence rate ratio from the complete dynamic population, which we calculated earlier, can be easily rewritten as (8/4)/(40 000 woman-years/80 000 woman-years). Between parentheses in the numerator of this formula is the number of pill users divided by the number of non-users among all women newly admitted with CHD (= cases in the case–control study). In the denominator, we find the proportion of woman-years on the pill divided by the proportion of woman-years of non-use. It is immediately obvious that—if the steady-state assumption holds—we can estimate the latter proportion directly from the sample of 600 women (= control subjects in case–control study). Among the 600 control subjects, the ratio of exposed to unexposed is expected to be the same as the ratio of the woman-years—except for sampling fluctuations. Thus, what we do in a case–control study is to replace the denominator ratio (40 000 woman-years /80 000 woman-years) by a sample (200/400). We still obtain, on average, the same rate ratio of 4. It follows that to estimate the rate ratio, we do not have to measure, nor to estimate, all the person-years of pill-using and non-using women in town; we can simply determine the ratio of those woman-years by asking a representative sample of women free of CHD from the population from which the cases arise, about their pill use. The complete dynamic population is called the ‘source population’ from which we identify the cases and the sample of control subjects, and the period over which cases and control subjects are identified is the ‘time window’ of observation, also called the ‘risk period’.
The ‘odds ratio’ which is calculated from Table 1 is technically also known as the ‘exposure odds ratio’, as it is the ‘odds of exposure’ in the cases divided by the ‘odds of exposure’ in the controls: (8/4)/(200/400) = 4, the same as the ratio of incidence rates in the whole source population. The great advantage of case–control studies is that we can calculate relative incidences of disease in a population, by collecting all the data for the numerator (by collecting cases in hospitals or registries where they naturally come together), and sampling control subjects from the denominator, i.e. sampling ‘control subjects’ to estimate the relative proportions (exposed vs non-exposed) of the person-years of the exposure of interest in the source population. Thus, one achieves the same result as in a comprehensive population follow-up, at much less expense of time and money. Just imagine the effort of having to do a follow-up study of all 120 000 women of reproductive age in town, also keeping track of when they move in and out of town and constantly updating their oral contraceptive use in a particular calendar year!
Advanced teaching
Cohorts vs dynamic populations.
For researchers who are used to think in terms of clinical cohorts, it can be difficult to understand that populations are not depleted: is it not true that the people with a particular risk factor will develop some disease more often, and thus in the course of time, there will be less of them who are still candidates for developing the disease? That will be true in cohorts because their membership is fixed, but not in dynamic populations. One way to understand this is to think of genetic exposures. People with blood group O develop clotting disorders more frequently, whereas people with blood group A develop more often gastric cancer. However, in a dynamic population, the numbers of people with blood group O or A are not constantly depleted—blood group distribution is fairly constant over time, as new people are born with these blood groups so that an equilibrium is maintained. 22
Another way to understand this concept is to think about an imaginary town and the cases of myocardial infarction that are enrolled in a study. For the aforementioned discussion, we assumed that we were studying all women living in a town during some time over the course of one calendar year (this could be the whole year or a few months). The situation would be entirely different if we restricted our study to all women who lived in the town on the 1 January of that year: then we would only count the myocardial infarctions that happened during this year in women who had been living in town on the 1 January; indeed, the number of women on the pill might decline more than the number of women not on the pill because the myocardial infarctions predominantly occur in the users. That situation would be akin to a clinical cohort study, i.e a study with fixed membership defined by a single common event. 22 However, in a dynamic population, a myocardial infarction that happens in a woman who moved into town during the year also counts in the numerator; she and the other women who move into town replenish the denominator because other women move out. By and large, as with blood groups, the population denominator remains constant in terms of its exposure distributions: the woman-years of oral contraceptive use vs non-use. If the population is truly in steady state, it does not matter when the control subjects are sampled—at the beginning, at the end or at the halfway point of the calendar period (the time window or ‘risk period’).
To refine the concept, the members of a dynamic population do not necessarily have to be present for long periods in the population—as might be surmised from the examples about towns and countries of which one is either an inhabitant or not, and usually for several years. Members of a dynamic population may also switch continuously between being in and out of the population. 22 Take a study on car accidents and mobile phone use by the driver. The risk periods of interest are the periods when people drive. The exposure of interest is phone use. In a case–control study, car accidents are sampled, and it is ascertained (say, via mobile phone operators) whether the driver was phoning at the time of the accident. Control moments might be sampled from the same driver (say, in the previous week) or from other drivers, by sampling other moments of time when they were driving; for each of these control moments, it might be ascertained, via the same mechanism as for the cases, whether they were phoning while driving. These control moments are contrasted with the moment of the accident (the case). If the same driver is used as his or her own control, this type of case–control study is called a ‘case–crossover study’. 24 From the example, it can be understood readily that such a case–control study compares the incidence rate of accidents while driving and phoning vs the incidence rate of accidents while driving and not phoning. 25
What if the exposure distribution of the population is not in steady state?
But what if the exposure distribution in the population is not in steady state? For example, suppose that one wants to investigate in a case–control study whether two different types of oral contraceptives give a different risk of venous thrombosis: ‘third-generation oral contraceptives’ vs ‘second-generation oral contraceptives’ (this was once a real and hotly debated question 26 ). Suppose further that the newer ‘third-generation oral contraceptives’ are strongly marketed, and that their market share clearly increases in the course of the calendar year. That situation is depicted in Figure 2 .
Sampling from the middle of the ‘risk period’ when the exposure distribution is not in steady state. The bold undulating lines show the increasing use of one type of oral contraceptives and the decreasing use of the other type during the time period (risk period). The finer lines below it depict individuals who enter and leave the populations of users of these types of oral contraceptives. Closed circles indicate cases of deep venous thrombosis (DVT) emanating from the population. B and D represent the numbers of users of one type or the other contraceptive at a cross-section in the middle of the time period. Incidence rates (IRs) of DVT can be calculated for both populations separately, and an incidence rate ratio (IRR) can be used to compare these two incidence rates. In a case–control study, B and D are estimated by ‘b’ and ‘d’, the numbers of users of one type or the other type of oral contraceptives in a sample from the source population taken in the middle of the period. The algebraic redrafting of the IRR shows that a ratio of IRs is algebraically equivalent to an ‘exposure odds ratio’ or the ‘cross-product’ that is obtained in a case–control study
There are two solutions:
Sample the control subjects in the middle of the period when the cases accrued, and thereby use the additional assumption that the rise (or fall) of the use of a particular brand of pill is roughly linear over the risk period. Then the control subjects will still represent the average proportion of person-years over the risk period. This is depicted in Figure 2 and is the same solution as is used to calculate person-years (i.e. the denominator) when populations are not in steady state [see previous article on the calculation of incidence rates for explanation]. 22 Alternatively, if one assumes that the incident cases in the dynamic population are evenly spread over time, one might sample control subjects evenly over time.
The more sophisticated solution is the one that researchers often use spontaneously: they sample a (number of) control subject(s) each time there is a case, which amounts to ‘matching on calendar time’. Then the control subject(s) will reflect the underlying population distribution of exposure at each point in time a case occurs, and any assumption about linearity is not needed. This is the most exact solution and is represented in Figure 3 . Matching on calendar time can be done in two ways: (i) invite the control subject(s) around the same calendar date as the case and ask them about their exposure (at that time or at previous times if exposure has a lag time to produce disease); or (ii) if control subjects are invited at a later point in time, present them with an ‘index date’, which is the date as the event of the matching case, and question them and/or measure their exposures for that index date. If control subjects are matched on calendar time, then it is appropriate to take the time matching (and, of course, any other matching factors) into account in the analysis, or at least to check whether it is necessary to control for them.
Case–control sampling in dynamic populations when a control is sampled each time a case occurs: matching on calendar time. Persons move in or out of the population by mechanisms such as birth or death, or move in or out from this population to another. Person-time is indicated by horizontal lines. The time axis is calendar time. The sampling of the control subjects is ‘matched on calendar time’: each time a case occurs, one or more control subjects are sampled. Cases and control subjects can be either exposed or unexposed (not shown here). A person who will become a case can be a control subject earlier, and multiple control subjects or even a variable number of control subjects can be drawn for each case
Hospital-based case–control studies
In most examples presented earlier, the patients are assumed to be sampled from a defined geographical population (via disease registries or by having access to all hospitals of some region), and control subjects are sampled from the underlying dynamic population of this geographical area. If cases from a case–control investigation are sampled from one or more hospitals that do not reflect a well-defined geographic population, still each hospital has a ‘catchment population’, consisting of the patients who will be admitted to that hospital when they develop a particular disease. Such a catchment population can be seen as a dynamic population, with inflow and outflow depending on patient and referring doctor preferences, religious or insurance affiliations, or on the reputation of a particular hospital for particular diseases and so forth. To obtain control subjects for such cases, the investigator should consider patients who are admitted to the same hospital and come from the same catchment population—meaning that if they had developed the case disease, they would have been admitted to that same hospital. This approach obviously has some risks in that the control disease may be associated with the exposure that one wants to study; that risk can (it is hoped) be minimized by using a mix of control diseases, none of which is known to be associated with the exposure under study. 27 Still, the principle of sampling control subjects from a dynamic population remains the same, whether the controls are population-based or hospital-based.
The early case–control study on oral contraceptives and myocardial infarction, which inspired the example presented earlier, sampled cases from a number of coronary care units that were surveyed in one geographically defined hospital area in the UK; for each case interviewed, three women of the same age who were discharged after some acute or elective medical or surgical condition were similarly interviewed about their use of oral contraceptives. 23 Likewise, the first case–control studies on smoking and lung cancer were hospital-based, and control subjects were non-cancer patients being present in the same wards or the same hospital as the lung cancer patients. 2 , 28
Doing a case–control study by sampling from a cohort with fixed membership is relatively rare—a recent survey found that it only occurs in 18% of published case–control studies. 1 It is mostly done when investigators have data available from a cohort, and when it is too expensive to go back and assess the exposures of everybody in the cohort. For example, in an occupational cohort study, personnel records may be available for all cohort members from date of employment, but it may take a considerable amount of work to assess these work histories and estimate cumulative exposures to particular chemicals, whether by using a job-exposure matrix or by an expert panel assessment. 29
Another example is the ‘re-use’ of data or samples from a randomized controlled trial (RCT) for a subsequent investigation. For example, the data from the ‘Physician’s Health Study’ 30 were re-used several years after the trial was finished for a new genetic case–control study; baseline blood samples of participants who developed cardiovascular end points in the trial were used, as were blood samples of matched participants in the trial who remained free of those diseases, and the frequency of one genetic factor (Factor V Leiden) was compared between these cases and control subjects. This investigation thereby considered the trial data as a single cohort in which new exposures were assessed, irrespective of the original randomization.
Figure 4 depicts a cohort with fixed membership from time 0. The cases accrue in the course of the follow-up in the exposed and unexposed part of the cohort. The available cohort data may only relate to exposure status at baseline (as in the aforementioned RCT example), but may also indicate changes in exposure over time, for example, if repeated measurements were done in the cohort study, or if time-related exposure information can be assessed from personnel records, prescribing records or other sources (as in the occupational example).
| Measure . | Definition . | Alternative formulation . |
|---|---|---|
| Odds ratio under exclusive sampling | ||
| Risk ratio under inclusive sampling |
Figure refers to methods 1 and 2 in text under subheading ‘Case–control studies within cohorts’, and is adapted from Rodrigues et al. [13] and Szklo and Nieto [18]
For each case, one or more control subjects are selected from the overall cohort, and the exposure statuses of the case and control subjects are determined at the time they are sampled. There are three options to sample control subjects: 12 , 13 , 18
As in the aforementioned RCT example, investigators often sample control subjects from the people who have still not developed the disease of interest at the end of follow-up (this is termed ‘cumulative incidence sampling’ or ‘exclusive sampling’), and exposure status at beginning of follow-up is used for these cases and controls. As shown algebraically in many textbooks, in that situation, the odds ratio is exactly the same (on average) as the corresponding odds ratio from the full cohort study, and this will approximate the risk ratio or rate ratio (in the full cohort study) only if the disease is rare (say, <5% of exposed and non-exposed develop the disease). This is the ‘rare disease assumption’, as historically first proposed by Cornfield in 1951. 3 It can be seen from Figure 4 that if the disease is rare, even in the exposed (sub)cohort, the ratio of people with and without exposure among those without disease at the end of the follow-up will remain about the same as at the beginning of the follow-up, which is why the ‘rare disease assumption’ works.
An imaginative solution, first proposed by Kupper et al. , 8 is to sample control subjects from all those in the cohort at the beginning of follow-up instead of at the end (‘case-cohort’ or ‘inclusive sampling’). At the beginning of the follow-up, all persons are still disease free (if they are not, then they would not have been included in the cohort). Then, the control subjects reflect the proportion exposed among the source population at the start of follow-up. Some of the control subjects who are sampled at baseline may become cases during follow-up. This seems strange at first sight, but it is not: if in a cohort study or an RCT, the risk is calculated, one uses all persons developing a disease outcome in the numerator, and divides by the denominator, which consists of all people who were present at start of follow-up, including those who will later turn up in the numerator. As can be seen from Figure 4 , sampling from the persons present at the beginning of the follow-up makes the odds ratio from the case–control study exactly the same (on average) as the risk ratio from the full cohort study. This can be understood most easily if one imagines taking a control sample of 100%, that is, all persons present at the beginning: then the odds ratio in the case–control study will be exactly the same as the risk ratio from the cohort study. Next, if one imagines taking a 50% sample for the control subjects, the odds ratio will remain the same (on average). One complication with this method is the calculation of the standard error of the odds ratio, as some persons are both cases and control subjects; different solutions exist. 31 A further complication is that, just as with the estimation of risks (which this sampling scheme corresponds to), losses to follow-up for other reasons than developing the disease that is studied are not easily taken into account; such losses to follow-up may produce bias if they are substantial and differ between exposed and unexposed.
The third option is to sample control subjects longitudinally throughout the risk period (i.e. not just at the beginning or just at the end). Throughout the follow-up of a cohort, the numbers of both exposed and unexposed persons who are free of disease will decrease, and people may be lost to follow-up for other reasons. Moreover, persons may move between exposure categories. The ‘royal road’ is to sample one or more control subjects at each point in time when a case occurs (‘density sampling’, ‘risk-set sampling’ or ‘concurrent sampling’) and determine the exposure status of cases and control subjects at that point in time. This is depicted in Figure 5 . By this sampling approach, the odds ratio from the case–control study will estimate the rate ratio from the cohort study. This is the equivalent of ‘matching on time’ in dynamic populations. This approach is most correct theoretically, but can only be used for cohorts when one has information about disease status of all persons at regular intervals during follow-up (e.g. when cancer incidence or mortality data are available over time).
Third method of sampling from a cohort: longitudinal sampling, also called concurrent sampling, density sampling or risk-set sampling. Persons start follow-up at inclusion in the cohort (e.g. date of surgery) and are followed until either end point occurs (person becomes a case), or the last calendar day of the study. Persons are indicated by fine lines from start of follow-up onwards. The time axis is follow-up time from inclusion (time 0). The longest period of follow-up is by persons who enter the cohort on the calendar day that the study starts; persons entering later will have shorter follow-up because they will be withdrawn from the study at the last calendar day of the study. Cases and control subjects can be either exposed or non-exposed (not shown here). A person who will become a case can be a control subject earlier, and multiple control subjects, or even a variable number of control subjects, can be drawn for each case. In text, see method 3, under subheading ‘Case–control studies within cohorts’
The first solution corresponds to the original theory proposed by Cornfield, 3 and requires the ‘rare disease assumption’ if the goal is to estimate rate ratio or risk ratios; it was the most frequently used method in case–control studies within cohorts in the past—and that approach was used in almost all case–control studies based on cohorts that were identified in the review by Knol et al. 1 Solution 2 still pertains to cohort thinking, but has an imaginative solution to calculate risk ratios; it is often called a ‘case–cohort’ study, and is particularly useful in studies in which a single control sample can be used for multiple case–control studies of various outcomes. Solution 3 is the more sophisticated development in case–control theory, in which the case–control odds ratio estimates the rate ratio from the cohort population over the follow-up period without the need for any rare disease assumption. 10 , 11 However, it is used relatively rarely. 1
A note about terminology: the term ‘nested case–control studies’ seems to be mostly used to denote case–control studies within cohorts which use the third sampling option. However, it is sometimes loosely used to denote all types of case–control sampling within a cohort.
The last method of sampling (method 3) immediately points to a conceptual unity of ‘incidence density sampling’ or ‘density sampling’ in cohorts and in dynamic populations. This was described by Prentice and Breslow in 1978 10 and expanded by Greenland and Thomas in 1982. 11 It can be grasped intuitively by comparing Figures 3 and 5 . The basis of the conceptual unity is that person-years can be calculated from cohorts and from dynamic populations, as was explained in our earlier article. 22
In a case–control study in a dynamic population, investigators often use matching on calendar time spontaneously (a control is chosen each time a case occurs), which is an ideal way of sampling, as it produces an odds ratio that directly estimates the incidence rate ratio, as in Figure 3 . In cohorts, however, one has to use sampling strategy 3, presented earlier, to estimate the incidence rate ratio, as in Figure 5 . The latter necessitates advanced insight and is used infrequently. In advanced textbooks, the ‘matching on time’ in dynamic populations and the ‘concurrent sampling’ in cohorts are often mentioned together as ‘density sampling’. This is theoretically correct, although it obscures the practicalities of the different sampling options.
‘Density sampling’ or ‘risk-set sampling’ from a cohort (i.e. the purer form of sampling of aforementioned strategy 3) involves sampling control subjects from the risk sets that are used in the corresponding Cox proportional hazards model. 10 , 11 A ‘hazard’ or ‘hazard rate’ is the name used in statistics for a peculiar form of ‘incidence rate’, wherein the duration of the follow-up approaches the limit of zero and becomes infinitesimally small; it is also called an ‘instantaneous hazard’. 22 When follow-up time is small, there is no numerical difference between risks and incidence rates. 22 Intuitively, a proportional hazards model in a follow-up analysis of a cohort can be understood as comparing the exposure odds of all successive cases at each point in time with those of the non-cases who are still at risk at that point in time (some of whom may become cases later), that is, the ‘risk set’. The exposure odds ratio or hazard ratio is then averaged over all of these comparisons, assuming it to be constant. Thus, a Cox proportional hazards model in a cohort becomes conceptually similar to a study that is ‘matched’ on time with a ‘variable control-to-case-ratio’ in a dynamic population. The estimation of the proportional hazard in a Cox model can be seen as an average of odds ratios over several risk sets; as the follow-up time in each risk set is small (say, the day of occurrence of the case disease), the odds ratios directly translate to relative risks and incidence rates, for reasons explained in the article on incidence calculations in dynamic populations. 21 , 22
The main difference between the approach we have described in this paper and the classic view of case–control studies as a ‘cohort study in reverse’ is that the dynamic population view reflects how the large majority of case–control studies are actually done. They are not done within cohorts, neither real nor imaginary. Rather, most case–control studies have an underlying population that is dynamic: for example, the geographically defined source population of a disease registry, the catchment areas of a hospital region or people who are driving.
The first case–control studies on smoking and lung cancer were done using cases and control subjects admitted to hospital from vaguely defined catchment areas. 2 , 28 Doll and Hill showed in the discussion of their original case–control study on smoking and lung cancer how one might calculate back to the general population, 2 as they assumed that they had sampled from that population—an insight that was far ahead of their time because it did not need the ‘rare disease assumption’. Although it originated during the period when Cornfield proposed his ‘rare disease assumption’, Doll and Hill’s solution was largely forgotten. Only occasionally does one read back-calculations from case–control studies to the background or source population, perhaps because such back-calculations have intricacies of their own, for example, in the case of matching. 32
An important consequence of primarily teaching case–control studies in dynamic populations, without the rare disease assumption, is that the real assumptions that are necessary for the majority of case–control studies become clear: either the exposure distribution should be in steady state in the dynamic population, or sampling of control subjects should be matched on time in a dynamic population (or equivalently, concurrent in the follow-up of a cohort).
An often-heard precept to guide the design of case–control studies is ‘Think of an imaginary randomized trial when planning your case–control study’. This gives the impression of automatically assuming a cohort, as all randomized trials are cohorts with a fixed membership. However, randomized trials can be done equally well on dynamic populations—public health interventions are often on dynamic populations. When the intervention or the exposure is studied in a case–control study with an underlying dynamic population, design features can be construed that are impossible or difficult in cohorts. For example, a dynamic population free of other key risk factors can be proposed: in a case–control study of the risk of oral contraceptives and venous thrombosis, an investigator might stipulate a dynamic population that has neither major surgery nor plaster casts after breaking legs and so forth—thus limiting the study to ‘idiopathic cases’. That would be difficult in a cohort; for example, in an imaginary randomized trial on oral contraceptives, wherein the outcome would be venous thrombosis, it would seem strange to truncate follow-up at the time of major surgery or plaster cast. In a dynamic population, however, the population is constantly renewed, and this exclusion comes naturally and may have advantages in attributing causality because other major risk factors for the outcome are excluded.
It should be emphasized that when cases and control subjects are selected from a dynamic population (or by risk-set sampling from a cohort), exposures do not need to be assessed solely at the time cases and control subjects are selected (e.g. ‘current use’ of oral contraceptives). In many circumstances, investigators need information on the duration of exposure and/or cumulative exposure. For example, in studies of smoking, the effect on lung cancer only becomes clear after several years. In contrast, the cardiovascular adverse effects of hormone replacement therapy may be limited to the first year of use, so recent exposure is most relevant. Recent and historical exposures can be assessed by a variety of methods in case–control studies, ranging from subjective (e.g. questionnaires) to more objective methods (e.g. birth records, pharmacy records and work histories combined with historical exposure monitoring data). The exposure definition can be easily adapted, by defining as many time windows of exposure as is deemed necessary, for recent and for long-term exposure, because there is a continuous turnover between these categories over time in the underlying population.
In summary, case–control studies with incident cases can be conducted in two contexts—dynamic populations and cohorts—of which the first is the most commonly used 1 because it comes naturally to most investigations. This method should become the basis of teaching case–control studies—in both introductory and more advanced courses:
Case–control studies can be conducted in a dynamic population, and the resulting odds ratio directly estimates the rate ratio from this dynamic population, provided that the control subjects represent the source population’s distribution of person-time of exposure over the risk period. This can be achieved either by matching on time or by selecting control subjects more loosely from the same period, if the population is judged to be in steady state for the exposure(s) and other variables of interest.
Case–control studies can also be conducted within a cohort; in this situation, control subjects can be sampled in three different ways, and the resulting odds ratio can estimate the odds ratio, risk ratio or rate ratio from the corresponding full cohort analysis. 21 Because such case–control studies are a minority, and the need for the rare disease assumption only applies for one method of sampling in such studies, they should not be made central to the basic teaching of case–control studies.
Jan P Vandenbroucke is an Academy Professor of the Royal Netherlands Academy of Arts and Sciences. The center for Public Health research is supported by a Programme Grant from the Health Research Council of New Zealand.
Conflict of interest: None declared.
Google Scholar
Google Preview
- steady state
- oral contraceptives
- mathematics
- rare diseases
| Month: | Total Views: |
|---|---|
| January 2017 | 94 |
| February 2017 | 445 |
| March 2017 | 229 |
| April 2017 | 56 |
| May 2017 | 246 |
| June 2017 | 145 |
| July 2017 | 112 |
| August 2017 | 113 |
| September 2017 | 191 |
| October 2017 | 254 |
| November 2017 | 237 |
| December 2017 | 642 |
| January 2018 | 808 |
| February 2018 | 822 |
| March 2018 | 1,019 |
| April 2018 | 1,157 |
| May 2018 | 980 |
| June 2018 | 798 |
| July 2018 | 560 |
| August 2018 | 1,048 |
| September 2018 | 1,034 |
| October 2018 | 970 |
| November 2018 | 878 |
| December 2018 | 564 |
| January 2019 | 580 |
| February 2019 | 817 |
| March 2019 | 952 |
| April 2019 | 947 |
| May 2019 | 980 |
| June 2019 | 583 |
| July 2019 | 531 |
| August 2019 | 460 |
| September 2019 | 710 |
| October 2019 | 704 |
| November 2019 | 560 |
| December 2019 | 446 |
| January 2020 | 485 |
| February 2020 | 580 |
| March 2020 | 489 |
| April 2020 | 405 |
| May 2020 | 395 |
| June 2020 | 532 |
| July 2020 | 404 |
| August 2020 | 442 |
| September 2020 | 561 |
| October 2020 | 660 |
| November 2020 | 483 |
| December 2020 | 422 |
| January 2021 | 453 |
| February 2021 | 443 |
| March 2021 | 565 |
| April 2021 | 503 |
| May 2021 | 465 |
| June 2021 | 330 |
| July 2021 | 310 |
| August 2021 | 321 |
| September 2021 | 574 |
| October 2021 | 564 |
| November 2021 | 387 |
| December 2021 | 344 |
| January 2022 | 427 |
| February 2022 | 501 |
| March 2022 | 500 |
| April 2022 | 451 |
| May 2022 | 488 |
| June 2022 | 319 |
| July 2022 | 291 |
| August 2022 | 289 |
| September 2022 | 440 |
| October 2022 | 571 |
| November 2022 | 461 |
| December 2022 | 377 |
| January 2023 | 380 |
| February 2023 | 359 |
| March 2023 | 415 |
| April 2023 | 460 |
| May 2023 | 414 |
| June 2023 | 329 |
| July 2023 | 325 |
| August 2023 | 332 |
| September 2023 | 483 |
| October 2023 | 647 |
| November 2023 | 475 |
| December 2023 | 370 |
| January 2024 | 673 |
| February 2024 | 502 |
| March 2024 | 708 |
| April 2024 | 530 |
| May 2024 | 563 |
| June 2024 | 284 |
Email alerts
Citing articles via, looking for your next opportunity.
- About International Journal of Epidemiology
- Recommend to your Library
Affiliations
- Online ISSN 1464-3685
- Copyright © 2024 International Epidemiological Association
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.

Case-Control Studies
Chris nickson.
- Nov 3, 2020
- a type of retrospective observational study
- control patients are ‘matched’ using some criteria (age, gender), typically should have no history of the disease of interest and should be representative of the general population
- begins with a definition of outcome or interest
- aims to identify potential risk factors associated with outcomes
- measures exposure to risk factors
- outcome = in case and controls
- odds ratio used to quantify risk, and can be adjusted for confounders (e.g. using logistic regression)
- quick, cheap and easy
- cases and controls may be sampled from pre-existing databases
- useful for identifying possible risk factors of a condition
- useful for studying rare conditions and those with a long latency period following exposure to risk
- not prone to loss to follow-up, unlike cohort studies
- may be used as the initial study generating hypotheses to be studied further by larger, more expensive prospective studies
DISADVANTAGES
- controls are often recruited by convenience sampling, and are thus not representative of the general population and prone to selection bias
- subject to confounding (other risk factors may be present that were not measured)
- not always possible in case-control studies to predict whether exposure to the risk factors preceded development of the disease or condition
- relative risk can not be determined as the incidence or prevalence of the condition of interest cannot be estimated in the population
- not suitable if exposure to the risk factors of interest is rare, as few of the cases and controls will have been exposed to them
- cannot determine causation, only association

Critical Care

Chris is an Intensivist and ECMO specialist at the Alfred ICU in Melbourne. He is also a Clinical Adjunct Associate Professor at Monash University . He is a co-founder of the Australia and New Zealand Clinician Educator Network (ANZCEN) and is the Lead for the ANZCEN Clinician Educator Incubator programme. He is on the Board of Directors for the Intensive Care Foundation and is a First Part Examiner for the College of Intensive Care Medicine . He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives.
After finishing his medical degree at the University of Auckland, he continued post-graduate training in New Zealand as well as Australia’s Northern Territory, Perth and Melbourne. He has completed fellowship training in both intensive care medicine and emergency medicine, as well as post-graduate training in biochemistry, clinical toxicology, clinical epidemiology, and health professional education.
He is actively involved in in using translational simulation to improve patient care and the design of processes and systems at Alfred Health. He coordinates the Alfred ICU’s education and simulation programmes and runs the unit’s education website, INTENSIVE . He created the ‘Critically Ill Airway’ course and teaches on numerous courses around the world. He is one of the founders of the FOAM movement (Free Open-Access Medical education) and is co-creator of litfl.com , the RAGE podcast , the Resuscitology course, and the SMACC conference.
His one great achievement is being the father of three amazing children.
On Twitter, he is @precordialthump .
| INTENSIVE | RAGE | Resuscitology | SMACC
Leave a Reply Cancel reply
This site uses Akismet to reduce spam. Learn how your comment data is processed .
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Case-control studies: basic concepts
Affiliation.
- 1 Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands. [email protected]
- PMID: 23045208
- DOI: 10.1093/ije/dys147
The purpose of this article is to present in elementary mathematical and statistical terms a simple way to quickly and effectively teach and understand case-control studies, as they are commonly done in dynamic populations-without using the rare disease assumption. Our focus is on case-control studies of disease incidence ('incident case-control studies'); we will not consider the situation of case-control studies of prevalent disease, which are published much less frequently.
PubMed Disclaimer
Similar articles
- Incidence rates in dynamic populations. Vandenbroucke JP, Pearce N. Vandenbroucke JP, et al. Int J Epidemiol. 2012 Oct;41(5):1472-9. doi: 10.1093/ije/dys142. Int J Epidemiol. 2012. PMID: 23045207 Free PMC article.
- Methods in epidemiology: observational study designs. DiPietro NA. DiPietro NA. Pharmacotherapy. 2010 Oct;30(10):973-84. doi: 10.1592/phco.30.10.973. Pharmacotherapy. 2010. PMID: 20874034 Review.
- What do case-control studies estimate? Survey of methods and assumptions in published case-control research. Knol MJ, Vandenbroucke JP, Scott P, Egger M. Knol MJ, et al. Am J Epidemiol. 2008 Nov 1;168(9):1073-81. doi: 10.1093/aje/kwn217. Epub 2008 Sep 15. Am J Epidemiol. 2008. PMID: 18794220
- Basic concepts in statistics for veterinary ophthalmologists. Montiani-Ferreira F, Cardoso FF, Petersen-Jones S. Montiani-Ferreira F, et al. Vet Ophthalmol. 2004 Mar-Apr;7(2):79-85. doi: 10.1111/j.1463-5224.2004.04002.x. Vet Ophthalmol. 2004. PMID: 14982586 Review.
- The case-crossover and case-time-control designs in pharmacoepidemiology. Donnan PT, Wang J. Donnan PT, et al. Pharmacoepidemiol Drug Saf. 2001 May;10(3):259-62. doi: 10.1002/pds.590. Pharmacoepidemiol Drug Saf. 2001. PMID: 11501340 No abstract available.
- Association between mRNA COVID-19 vaccine boosters and mortality in Japan: The VENUS study. Mimura W, Ishiguro C, Maeda M, Murata F, Fukuda H. Mimura W, et al. Hum Vaccin Immunother. 2024 Dec 31;20(1):2350091. doi: 10.1080/21645515.2024.2350091. Epub 2024 May 17. Hum Vaccin Immunother. 2024. PMID: 38757631 Free PMC article.
- Low-dose aspirin use and risk of ovarian cancer: a combined analysis from two nationwide studies in Denmark and Sweden. Zheng G, Faber MT, Wang J, Baandrup L, Hertzum-Larsen R, Sundström K, Kjær SK. Zheng G, et al. Br J Cancer. 2024 May;130(8):1279-1285. doi: 10.1038/s41416-024-02609-7. Epub 2024 Feb 12. Br J Cancer. 2024. PMID: 38347096
- Type, Etiology, and Duration of Epilepsy as Risk Factors for SUDEP: Further Analyses of a Population-Based Case-Control Study. Sveinsson O, Andersson T, Carlsson S, Tomson T. Sveinsson O, et al. Neurology. 2023 Nov 27;101(22):e2257-e2265. doi: 10.1212/WNL.0000000000207921. Neurology. 2023. PMID: 37813583
- Association between cumulative exposure periods of flupentixol or any antipsychotics and risk of lung cancer. Chai Y, Chu RYK, Hu Y, Lam ICH, Cheng FWT, Luo H, Wong MCS, Chan SSM, Chan EWY, Wong ICK, Lai FTT. Chai Y, et al. Commun Med (Lond). 2023 Sep 26;3(1):126. doi: 10.1038/s43856-023-00364-z. Commun Med (Lond). 2023. PMID: 37752185 Free PMC article.
- Circulating IgG antibodies to periodontal bacteria and lung cancer risk in the CLUE cohorts. Ampomah NK, Teles F, Martin LM, Lu J, Koestler DC, Kelsey KT, Beck JD, Platz EA, Michaud DS. Ampomah NK, et al. JNCI Cancer Spectr. 2023 May 2;7(3):pkad029. doi: 10.1093/jncics/pkad029. JNCI Cancer Spectr. 2023. PMID: 37040077 Free PMC article.
Publication types
- Search in MeSH
LinkOut - more resources
Full text sources.
- Ovid Technologies, Inc.
- Silverchair Information Systems

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
CBSE Class 12 Case Studies In Business Studies – Controlling
CONTROLLING Controlling: Definition Controlling means ensuring that activities in an organisation are performed as per the plans.
Importance of Controlling
- It helps in accomplishing organisational goals by constantly monitoring the performance of the employees and bringing to light the deviations, if any, and taking appropriate corrective action.
- It helps the business managers to judge the objectivity and accuracy of the standards.
- It seeks to make efficient use of resources.
- It seeks to motivate the employees and helps them in giving a better performance.
- It creates an atmosphere of order and discipline in the organisation.
- It facilitates coordination in action by providing direction to all activities within and among departments.
Features of Controlling
- It is a goal-oriented function.
- It is a pervasive function as it is used in the organisations of varying types and sizes.
- It is considered to be a forward looking function as it helps to improve the planning by providing valuable feedback for reviewing and revising the standards.
- It is considered to be a backward looking function as it is like the post mortem of the past activities to ascertain the deviations if any.
- It is not the last function of management as it brings the management cycle back to the planning function.
Steps Involved in the Controlling Process
- Setting performance standards in clear, specific and measurable terms.
- Measurement of actual performance as far as possible in the same units in which standards are set.
- Comparing actual performance with standards to identify deviations if any.
- Analysing deviations through critical point control and management by exception approaches to identify the causes for their occurrence.
- Taking corrective action whenever the deviation occurs beyond the permissible limits so that it does not reoccur in future.
Relationship between Planning and Controlling
- Planning without controlling is useless and controlling without planning is blind.
- Planning provides the basis of controlling by setting the standards in advance. In the absence of these standards, managers will not know what all activities have to be controlled.
- Planning is prescriptive in nature whereas, controlling is evaluative.
- Thus, planning and controlling are interrelated and interdependent. As planning is based on facts, it makes controlling easier and effective whereas controlling helps to improve future planning by providing valuable information derived from the past experiences.
LATEST CBSE QUESTIONS
Question 1. Hina Sweets is a renowned name for quality sweets since 1935. Harsh the owner of Hina Sweets was worried as the sales had declined during the last three months. When he enquired from the Sales Manager, the Sales Manager reported that there were some complaints about the quality of sweets. Therefore Harsh ordered for sample checking of sweets. Identify the step taken by Harsh that is related to one of the functions of management. (CBSE, Delhi 2017) Answer: Measurement of actual performance is the step in controlling process being described.
Question 2. State the steps in the process of controlling. (CBSE, Delhi 2017) Answer: The various steps involved in the controlling process are described below:
- Setting performance standards: The first step in the controlling process involves setting standards in clear, specific and measurable terms. Standards can be set in both quantitative as well as qualitative terms. It is important that standards should be flexible enough to be modified with the changes taking place in the internal and external business environment.
- Measurement of actual performance: The next step relates to the measurement of actual performance. Performance should be measured in an objective and reliable manner. As far as possible, performance should be measured in the same units in which standards are set as this would make their comparison easier. Depending upon the nature of work various techniques for measurement of performance like personal observation, sample checking, performance reports, etc. may be used.
- Comparison of actual performance with standards: This step involves comparison of actual performance with the standard. Such comparison will reveal the deviation and noting deviations if any. If the actual performance is more than planned performance deviations are said to be positive or vice-versa.
- Critical point control: All the deviations may not be significant. Moreover, it may not be either economical nor easy to monitor each and every activity in the organisation. Therefore, every organisation identifies and states its specific key result areas (KRAs) or critical points which require tight control are likely to have a significant effect on the working of the business. Any deviations on these points are attended to urgently by the management. Like if the expenditure on refreshment of workers goes up by 10% it can be ignored but if the production cost goes up by 5% it may call for managerial action.
- Management by exception: Management by exception is the principle of management control which is based on the belief that if you try to control everything, you may end up controlling nothing. Therefore, only significant deviations which go beyond the permissible limits should be brought to the notice of the management. Like the output defects upto 2% may be considered acceptable but if goes up by 5% it may call for managerial action.
- Taking corrective action: This is the final step involved in the controlling process. When the deviations are within acceptable limits no corrective action is required. However, when the deviations go beyond the acceptable range, especially in the important areas, it demands immediate managerial attention so that deviations do not occur again and standards are accomplished. Corrective action might involve training of employees, buying new machinery, increasing supervision and so on.
- Planning is based on facts and makes controlling process easier and adds to the effectiveness.
- Controlling also adds to the effectiveness of planning process by providing valuable feedback based on past experiences.
Question 4. State any five points that highlight the importance of ‘controlling’ function of management. (CBSE, Delhi 2017) Answer: The importance of controlling function of management is described below:
- Accomplishing organisational goals: The controlling function facilitates constant monitoring of the actual performance in comparison to the predetermined standards and brings to light the deviations, if any, and indicates corrective action. All these activities ensure that organisational goals are realised efficiently and effectively.
- Judging accuracy of standards: A good control system enables management to verify whether the standards set are accurate and objective. Moreover, helps to review and revise the standards in light of changes taking place in the organisation or business environment in general.
- Making efficient use of resources: By implementing a good control system a manager seeks to reduce wastage and spoilage of resources. This is because each activity is performed in accordance with predetermined standards and norms rather than hit and trial method.
- Improving employee motivation: An effective control system seeks to provide motivation to the employees as they are made aware well in advance what they are expected to do and what are the standards of performance on the basis of which they will be appraised. This approach helps them to give better performance.
- Ensuring order and discipline: A constant check on the behaviour and work of the employees leads to creation of an atmosphere of order and discipline in the organisation.
Question 5. How does controlling help in “Judging accuracy of standards” and “Ensuring order and discipline” ? (CBSE, Sample Paper, 2017) Answer: Controlling helps in “Judging accuracy of standards” and “Ensuring order and discipline” as explained below:
- Judging accuracy of standards: An efficient control system enables management to determine weather the standards set are accurate and objective. This is because it helps to helps to review and revise the standards in light the changes taking place in the organisation and in the environment.
- Ensuring order and discipline: Controlling helps to minimise dishonest behaviour on the part of the employees by keeping a close check on their activities. Thus, it creates an atmosphere of order and discipline in the organisation.
Question 6. ‘If anything goes wrong with the performance of key activities, the entire organisation suffers. Therefore, the organisation should focus on them.’ Explain the statement with a suitable example. (CBSE, Sample Paper 2015-16) Answer: The given statement refers to the importance of ‘Critical Point Control’ in order to ensure effective performance of key activities in an organisation. Critical Point Control: It may not be either economical nor easy to monitor each and every activity in the organisation. Therefore, every organisation identifies and states its specific Key Result Areas (KRAs) or critical points which require tight control and are likely to have a significant effect on the working of the business. Any deviations on these points are attended to urgently by the management. For example, if in an organisation, the expenditure on stationery goes up by 10%, it can be ignored but if the production cost goes up by 5%, it may call for managerial action.
Question 7. Mr. Nath, a recently appointed production manager of Suntech Ltd., has decided to produce jute bags instead of plastic bags as these are banned by the government. He set a target of producing 1000 jute bags a day. It was reported that the employees were not able to achieve the target. After analysis, he found that employees were demotivated and not putting in their best for achieving the target. Mr. Nath’s behaviour is good towards the employees. His attitude is always positive. So, he announced various incentive schemes for the employees like:
- Installing awards or certificates for best performance
- Rewarding an employee for giving valuable suggestions
- Identify the functions of management highlighted in the above paragraph.
- State the incentive under which the employee are motivated.
- State any two values which the production manager wants to communicate to society by his work and behaviour. (CBSE, Sample Paper 2015)
- The functions of management highlighted in the above paragraph are Controlling and Directing.
- The employees are motivated under Employee recognition programmes which is a non-financial incentive. Employee recognition programmes helps to fulfill the need of due consideration and appreciation of the people working in an organisation. It boosts their self-esteem and motivates them to work with greater zeal and enthusiasm.
- Respect for employees
- Concern for environment
Question 8. A company was manufacturing LED bulbs which were in great demand. It was found that the target of producing 300 bulbs a day was not met by the employees. On analysis, it was found that the workers were not at fault. Due to electricity failure and shortage of workers, the company was not able to achieve the set targets and alternative arrangements were needed. To meet the increased demand, the company assessed that approximately 88 additional workers were required out of which 8 would work as heads of different departments and 10 would work as subordinates under each head. The required qualifications and job specifications were also enlisted. It was also decided that necessary relaxations should be given to encourage women, people from backward and rural areas and people with special abilities to assume responsible positions in the organisations. All efforts were made to match the ability of the applicants with the nature of work.
- Identify the functions of management discussed above.
- State the two steps in the process of each function discussed in the above paragraph.
- List any two values which the company wants to communicate to the society. (CBSE, Delhi 2015)
- The functions of management discussed above are Staffing and Controlling.
- Estimating manpower requirements: The manpower requirements of an organisation are estimated through workload analysis and workforce analysis. The workload analysis helps to determine the number and type of human resource required in the organisation to meet its present and future needs. Whereas workforce analysis seeks to determine the number and type of human resource available within the organisation.
- Recruitment: The process of recruitment involves searching for the prospective candidates and stimulating them to apply for jobs in the organisation. There are two sources of recruitment namely, internal and external. The two steps involved in controlling function are as follows:
- Comparing actual performance with standards to identify deviations if any. “It was found that the target of producing 300 bulbs a day was not met by the employees.”
- Analysing deviations through critical point control and management by exception approach to identify the causes for their occurrence. “On analysis, it was found that the workers were not at fault. Due to electricity failure and shortage of workers, the company was not able to achieve the set targets and alternative arrangements were needed.”
- Taking corrective action, if required “To meet the increased demand, the company assessed that approximately … as subordinate under each head.”
- Women empowerment
Question 9. ‘AS Ltd.’ is a large company engaged in assembling of air-conditioners. Recently the company had conducted the ‘Time’ and ‘Motion’ study and concluded that on an average, a worker can assemble ten air-conditioners in a day. The target volume of the company in a day is assembling of 1,000 units of air-conditioners. The company is providing attractive allowances to reduce labour turnover and absenteeism. All the workers are happy. Even then the assembling of air-conditioners per day is 800 units only. To find out the reason, the company compared actual performance of each worker and observed through CCTV that some of the workers were busy in gossiping.
- Identify the function of management discussed above.
- State the steps in the process of the function identified which are discussed in the above paragraph. (CBSE, 2015)
- The function of management discussed above is Controlling.
- Setting standards of performance: “concluded that on an average, a worker can assemble ten air-conditioners in a day.” “The target volume of the company in a day is assembling of 1,000 units of air-conditioners.”
- Measurement of actual performance: ” Even then the assembling of air-conditioners per day is 800 units only.”
- Comparison of actual performance with the standards: The company compared actual performance of the workers with the planned performance and noted deviation of 200 units.
- Analysing deviations: “To find out the reason, the company compared the actual performance of each worker and observed through CCTV that some of the workers were busy in gossiping.”
Question 10. PQR Ltd. is engaged in manufacturing machine components. The target production is 200 units per day. The company had been successfully attaining this target until two months ago. Over the last two months, it has been observed that daily production varies between 150-170 units.
- Identify the management function to rectify the above situation.
- Briefly state the procedure to be followed so that the actual production may come up to the target production. (CBSE, Delhi 2010)
- The controlling function of management is needed to rectify the above situation.
- Providing training to workers if the workers are not well versed with the production process.
- Improving the work environment if it is not conducive to efficient working.
- Ensuring timely availability of the raw materials and other equipments if they are not made available on time.
- Replacing the machinery if it is defective or has become obsolete.
Question 11. Rajeev and Sanjeev are managers in the same organisation heading different units. While discussing about the functions of management, Rajeev says that ‘Planning is looking ahead whereas controlling is looking back.’ But Sanjeev says, ‘You are wrong because planning is looking back whereas controlling is looking ahead.’ Both are giving reasons in favour of their statements. Explain the possible reasons given by both and justify who is correct. (CBSE, 2009) Answer: Both Rajeev and Sanjeev are correct in their statements as explained below:
- Planning is considered as a forward looking function by Rajeev as plans are made for future.
- Planning may be considered as a backward looking function by Sanjeev because the quality of planning can be improved with the help of valuable information provided by controlling in terms of results achieved.
- Controlling is considered as a backward looking function by Rajeev as it is like the post mortem of the past activities to ascertain the deviations if any.
- Controlling is considered as a forward looking function by Sanjeev as it helps to improve the future performance by providing guidance for taking corrective action so that deviations do not reoccur in future.
Question 12. Kapil & Co. is a large manufacturing unit. Recently the company had conducted time and motion studies and concluded that on an average, a worker could produce 300 units per day. However, it has been noticed that the average daily production per worker is in the range of 200-225 units.
- Name the function of management and identify the steps in the process of this function which helped in finding out that the actual production of a worker is less than the set target.
- To complete the process of the function identified in (1) and to ensure the performance as per time and motion studies, explain what further steps a manager has to take? (CBSE, 2010)
- Setting performance standards in clear, specific and measurable terms. “Recently the company had conducted time and motion studies and concluded that on an average, a worker could produce 300 units per day.”
- Measurement of actual performance as far as possible in the same units in which standards are set. “It has been noticed that the average daily production per worker is in the range of 200-225 units”.
- Comparing actual performance with standards to identify deviations if any. In the given case there is a deviation in output in the range of 25-50 units per worker.
- The workers are not well versed with the production process.
- The working environment is not conducive to efficient working.
- The raw materials and other equipment are not available on time.
- Taking corrective action: The deviations require immediate management attention so that they do not reoccur in future. Therefore, the manager should take appropriate corrective action after analyzing the situation like providing training to workers, improving the work environment, and ensuring timely availability of the raw materials and other equipment.
Question 13. K&K Co. Ltd. is engaged in manufacturing of machine components. The target of production is 200 units daily. The company had been successfully attaining this target until two months ago. Over the last two months it has been observed that daily production varies between 150-170 units. Identify the possible causes for the decline in production and the steps to be taken to achieve the desire targets. (CBSE, 2008) Answer: The possible causes for decline in production are listed below:
- The machinery is defective or has become obsolete.
The deviations require immediate management attention so that- they do not reoccur in future. Therefore, the manager should take appropriate corrective action after analyzing the situation like providing training to workers, improving the work environment, ensuring timely availability of the raw materials and other equipment or replacing the machinery.
ADDITIONAL QUESTIONS
Question 1. ‘Taste Buds Ltd.’ is a company known for manufacturing good quality confectionery products. The automated system of production ensures uniformity in production and quality maintenance. The quality assurance team conducts stringent checks at all stages, records and analyses the deviations and takes the necessary corrective actions right from the procurement of raw material to its processing, production and packaging. The company has a well-equipped in¬house quality inspection cell where confectionery products are tested on various parameters of quality by the team of experienced quality staff. In context of the above case:
- Identify and explain the function of management being performed by the quality assurance team of ‘Taste Buds Ltd.’
- Explain the statement, “records and analyses the deviations and takes the necessary corrective actions”.
- Controlling is the function of management being performed by the quality assurance team of ‘Taste Buds Ltd.’ Controlling is the process of ensuring that events conform to plans.
- Comparing the actual performance with the standards: The actual performance is compared with the standards and deviations, if any, are recorded.
- Critical point control: All the deviations may not be significant. Moreover, it may not be either economical nor easy to monitor each and every activity in the organisation. Therefore, every organisation identifies and states its specific key result areas (KRAs) or critical points which require tight control as they are likely to have a significant effect on the working of the business. Any deviations on these points are attended to urgently by the management. Like in the above case, if the expenditure on refreshment of workers goes up by 10% it can be ignored but if the production cost goes up by 5% it may call for managerial action.
- Management by exception: Management by exception is the principle of manage¬ment control which is based on the belief that if you try to control everything, you may end up controlling nothing. Therefore, only significant deviations which go beyond the permissible limits should be brought to the notice of the management. Like in the above case, the output defects upto 2% may be considered acceptable but if it goes up by 5%, it may cal for managerial action.
- Taking corrective action: The last step in controlling process involves taking corrective action whenever the deviation occurs beyond the permissible limits so that they do not reoccur in future. However, the standards may be revised if it is not possible to check deviations through corrective action.
Question 2. Anubhav has set up an export house after completing his masters in fashion designing. As the quality of the garment depends on the quality of raw material used, he assures that the fabric meets the requirements by conducting a series of tests for the fabrics like shrinkage test, testing colour fastness to washing, colour fastness to light, colour fastness to perspiration etc through laboratory tests. Later on, at the production areas, fabric inspection is also conducted by stopping the production process. The tests help to detect the deviations and also take corrective action. Moreover, he ensures that complete training about production work was given to every worker at the time of joining his export house. In context of the above case:
- Identify the function of management being performed by Anubhav by conducting tests to assure for the quality of the garments manufactured in his export house.
- Briefly explain the term ‘deviations.’
- Give any three advantages of giving training to the employees.
- Controlling is the function of management being performed by Anubhav by conducting tests to assure for the quality of the garments manufactured in his export house.
- The term ‘deviations’ refers to the difference between the actual performance and planned performance. If the actual performance is more than the planned performance, it may be said to be positive in nature or vice-versa.
- Training imparts systematic learning to the employees thereby helping to avoid wastage of efforts and money and is considered better than the hit and trial method.
- It increases the employees’ productivity both in terms of quantity and quality, leading to higher profits.
- Training increases the morale of the employees and reduces absenteeism and employee turnover.
Question 3. Raghav started a take away eating joint in a nearby market. His business was doing well. He ensured that the food was properly cooked, a standard taste was maintained, packing of food was done effectively and the orders were executed on time. But unfortunately he met with an accident and was advised three months bed rest. In his absence, his cousin Rohit took charge of his business. When he resumed his work after three months, he realised that his clientele had dropped. The people were not happy with the services as the quality of food had deteriorated and the delivery time for orders had increased considerably. All this was happening because most of his previous staff had left as Rohit used to adopt a very strict and authoritative approach towards them. In context of the above case:
- List any two aspects about his business that Raghav was controlling in order to make it successful.
- Explain briefly any two points to highlight the importance of the controlling function.
- Name and explain the style of leadership adopted by Rohit.
- A standard taste was maintained.
- The orders were executed on time.
- Judging accuracy of standards: The controlling function helps the business managers to judge the objectivity and accuracy of the current standards. It also assists in reviewing and revising the standards keeping in view the forthcoming changes in both the internal and external environment of the business.
- Improving employee motivation: The controlling function seeks to motivate the employees and helps them to give better performance. This is because it makes them aware well in advance about what they are expected to do and what the standards of performance are on the basis of which they will be judged.
- Rohit had adopted an autocratic style of leadership. An autocratic leader expects strict compliance from his subordinates with regard to the orders and instructions given by him. Therefore, it involves only one-way communication.
Question 4. ‘Saurashtra’ is a company involved in the export of indigenous food products like chutneys and pickles. It has tied up with the small farmers in various states for sourcing of fruits and vegetables. In this way it helps the small farmers to sell their produce at reasonable rates. The company follows a practice where only significant deviations from a budget or plan are brought to the attention of management. The degree of deviations allowed in different categories in the budget are well defined in advance, along with the appropriate levels of management who will respond to the deviations in question. For example, a deviation of Rs. 20,000 or more in purchase costs will be reported to the concerned department manager. In context of the above case:
- Identify the principle of management control adopted by the company. State the belief underlying this principle.
- List any two values that the company wants to communicate to the society.
- Management by exception is the principle of management control adopted by the company. It is based on the belief that ‘if you try to control everything, you may end up controlling nothing’.
- Rural development
- Sense of responsibility
Question 5. Shruti has established a small scale factory after completing a course in textile designing. She has tied up with the big home furnishing retail outlets in the city for supplying to them good quality designer home furnishing products like bed covers, cushions etc. She believes that controlling without planning is blind. So, every time she gets an order, she sets the standards in terms of the number of personnel required, the estimated requirements in man-hours per product, the requirements of direct materials for the projected production and the amount of normal overhead expenses required at the projected work-load. She also keeps a close watch on the activities so as to ensure that they conform to plans. Whenever the order size is too large, she hires extra workers by placing a notice on the notice-board of the factory specifying the details of the jobs available. In context of the above case:
- Identify the functions of management being performed by Shruti.
- Do you think Shruti is right in her thinking that, “controlling without planning is blind.” Explain by bringing out the relationship between planning and controlling.
- Name the source of recruitment adopted by Shruti. Also, mention its type.
- The functions of management being performed by Shruti are Controlling and Staffing.
- Yes, Shruti is right in thinking that, ” controlling without planning is blind.” Planning provides the basis of controlling by setting the standards in advance. In the absence of these standards, managers will not know what all activities have to be controlled. Planning is prescriptive in nature whereas controlling is evaluative. Thus, planning and controlling are interrelated and interdependent as planning is based on facts and makes controlling easier and effective whereas controlling helps to improve future planning by providing valuable information derived from the past experiences.
- The source of recruitment adopted by Shruti is Direct Recruitment. It is an external source of recruitment.
Question 6. Vishesh works as an interior designer. He gets a contract to redesign a play school. He employs three painters on the site assuming that an average painter will be able to paint 10 desks in a day. At the end of the first day of their work, Vishesh finds that the painter A, painter B and painter C have painted 12, 14 and 15 desks respectively. On comparing the actual performance with the planned performance, he realises that the standard set by him is too low. Consequently, he decides to review and revise the standard and raise it. In context of the above case:
- Identify the function of management being performed by Vishesh.
- “Planning and controlling are both backward looking as well as forward looking functions.” Explain the statement with reference to the above paragraph.
- Controlling is the function of management being performed by Vishesh.
- It is appropriate to say that, “Planning and controlling are both backward looking as well as forward looking functions” as evident from the above case. Planning is considered as a forward looking function as plans are made for future. “assuming that an average painter will be able to paint 10 desks in a day.” Planning may be considered as a backward looking function because the quality of planning can be improved with the help of valuable information provided by controlling in terms of results achieved. “On comparing the actual performance with the planned performance, he realises that the standard set by him is too low.” Controlling is considered as a backward looking function as it is like the post mortem of the past activities to ascertain the deviations if any. “At the end of the first day of their work, Vishesh finds that the painter A, painter B and painter C have painted 12, 14 and 15 desks respectively.” Controlling is considered as a forward looking function as it helps to improve the future performance by providing guidance for taking corrective action so that deviations do not reoccur in future. “Consequently, he decides to review and revise the standard and raise it.
Question 7. A critical point control (CPC) approach is followed by McDonald in the cooking and handling process so that any food safety threat can be prevented, eliminated, or reduced to an acceptable level. Hence, continuous monitoring of activities are undertaken to ensure that the process is right at each critical point control. The main principle followed for cooking at McDonald is “less amount many time” which can ensure the high quality and high fresh level of the food. For instance, if four hamburgers have to be made, a worker cannot cook all the four hamburgers at one time. The time figured out for making one hamburger is one hundred and forty-five seconds. Moreover, nearly all foods in the McDonald have the specific holding time, the holding time for hamburgers is ten minutes and for french fries is seven minutes. If it is not sold within that time it is thrown away. Also, the temperature of the milk sent by the supplier must be under 4° C, otherwise, it will be returned. In context of the above case:
- Name the steps involved in the controlling process which is being discussed in the above lines.
- What do you understand by ‘critical point control’? Explain.
- How does the controlling function of management help in accomplishing organisational .goals and ensure efficient use of resources?
- Analysing deviation and taking corrective action are being discussed in the above lines.
- Since it may neither be economical nor easy to monitor each and every activity in the organisation, therefore, every organisation identifies ar\d states its specific key result areas (KRAs) or critical points which require tight control are likely to have a significant effect on the working of the business. Any deviations on these points are attended to urgently by the management.
- Accomplishing organisational goals: The controlling function helps in accomplishing organisational goals by constantly monitoring the performance of the employees and bringing to light the deviations, if any, and taking appropriate corrective action.
- Making efficient use of resources: The controlling function enables the managers to work as per predetermined standards. This helps to avoid any ambiguity in business operations and reduce wastage and spoilage of resources in the organisation.
Case Studies in Business Studies Business Studies Case Studies Business Studies Commerce
Studyresearch
End to your search for good notes!!
- MCQs – Nature & Significance of Management
- MCQs- Principles of Management
- MCQs – Chapter – Business Environment
- MCQs – Chapter Planning
- MCQs – Chapter – Organizing
- MCQs – Chapter Staffing
- MCQs – Chapter – Directing PART-1
- MCQs – Chapter – Directing – Part-2
- MCQs- Chapter Controlling
- MCQs- Chapter – Financial Management
- MCQs – Chapter – Marketing Management Part-1
- MCQs- Chapter- Marketing Management -Part-2
- MCQs – Chapter- Marketing Management – Part-3
- Case Studies- Principles of Management
- Case Study – Business Environment
- Case Study-Planning
- Case Study-Organizing
- Case Study- Staffing
- Case Study-Directing
- Case Study – Chapter Controlling
- MCQs – Ch-2 – An Entrepreneur – Part-1
- MCQs – Ch-2 – An Entrepreneur – Part-2
- Ch-3 MCQs for ENTREPRENEURIAL JOURNEY
- MCQs – Ch-4 Entrepreneurship As Innovation And Problem Solving
- Ch-5 MCQs Analysis of Market Env & Market Research
- CH-6 MCQs Unit of sale – Unit cost – Gross Profit
- Unit-2 Entrepreneurial Planning
- Download PDF| Unit-3 Marketing Strategies
- Download PDF | UNIT-4 Enterprise Growth Strategies
- Download PDF | UNIT-6 Resource Mobilization
- Download PDF |Unit 1 ENTREPRENEURSHIP
- Download PDF | Unit-3 Marketing Strategies
- Download PDF| UNIT-4 | Enterprise Growth Strategies

Case Study – Chapter Controlling
Case Studies – Class 12 – Controlling
Case Study for chapter – Controlling
Especially for class 12 – cbse business studies students.
Q1: Managers at Virginia city import-export company suspected Corporate Defence Strategies od Maywood New jersey advised the firm to install a software program that could secretly log every single stroke of the suspect’s computer Keys and send an encrypted e-mail report to CDS. Investigator revealed that two employees were deleting orders from the corporate books after processing them, pocketing the revenue and building their own company with in. In the above one of the important functions of management is performed.
(a) Identify the function
(b) and identify one of the importance of this function corresponding to above case.
(c) explain any other two importance of identified function.
Q2: FedEx operates an $ 23 billion delivery system from its London and six international based hubs. An important part of FedEx system was their ability to track customers parcels at each stage of collection, shipment and delivery also at FedEx its system helps in identify which customers generate maximum profits and which eventually end up costing the company. FedEx closes the accounts that are not profitable to serve.
(a): In the above case identify the function of management by quoting the lines which helped in identifying above function.
(b) Also identify two steps of above function by quoting the lines from above case study.
Answers: (a) Controlling, Quoted line: An important part………..profitable to serve
(b): Measuring actual performance.” An important…….shipment and delivery”. Comparing actual performance with standards, ” its system…………costing the company”.
Taking corrective action ” FedEx closes the accounts……………to serve.
Q3: Raman and Aman are working as planning department and quality check department in their organisation respectively. Raman is of the view that quality check is not possible without standards and Aman is of the view that standards for coming year cannot be made without the help of quality check department. Who among them is correct? Give conceptual reason for your answer.
For reason explain the relation between Planning and Controlling
Q4: Smith Courier System based in Switzerland is a provider of same day delivery services. although Smith may do everything right to meet its delivery commitments, it relies on commercial airlines to transport its parcels and occasionally fails to meet its deadlines. Delays are usually a result of packages being misplaced in airlines tracking systems. Such incidents are beyond Sterling’s control. But from the customer’s vantage point, the failure is smith’s problem. To control the damage created by such delays, Smith had to take some rectification measures. for example, for several months in 1990 and early 1991 several S deliveries disappeared in transit. The packages turned up later, but customer has already suffered financial losses. Yet because the packages were eventually recovered, neither insurance company nor the airlines was liable. The decision of the president Glenn was whether to compensate the customers for their losses or simply not to charge them for the shipments, Glenn concluded that not charging for the shipment was inadequate response given the suffered downtime. but paying the $30,000 in losses would push the then five-year-old $6 million company to losses for the quarter. Glenn’s decision was to pay out the $30,000 in gratis service, the customer stayed, and Smith continue to grow.
(a) Identify one of the important management functions performed by Glenn which helped Smith Courier System to survive and grow.
(b) Also identify the steps of Process of function identified in (a) by quoting the lines from above case.
Answers: (a) Controlling
(b) line quoted: ‘smith courier………..delivery commitments’., step: setting performance standards, line quoted: it relies………its deadlines”, step: measurement of actual performance, line quoted: “delays are…….tracking system”., step: analysing deviations, line quoted: “glenn’s decision……to grow”., step: taking corrective action..
Q5: At Sam defines lack of quality had created a crisis, When the government shut it down because it was not meeting quality standards, Sam brought back a TQM programme that had restored quality. Although Sam’s weapons worked well, the government questions the company’s quality practices and policies. To solve these problems Sam defence went through an organisational transformation. The key elements were: (I) to minimise the dishonest behaviour on the part of the employees by keeping a close check on their activities.(ii) Empowering employees by giving them responsibility and accountability of their performance.(iii) To provide common direction to all activities,
Explain the importance of controlling highlighted in above key elements.
Ans: (I) Ensuring order and discipline.
(ii) improving employee’s motivation., (iii) facilitating coordination in action..
We have disabled - Right- Click - How about stay to read :)
Case Report vs Case-Control Study: A Simple Explanation
A case report is the description of the clinical story of a single patient, whereas a case-control study compares 2 groups of participants differing in outcome in order to determine if a suspected exposure in their past caused that difference.
| Case Report | Case-Control Study | |
|---|---|---|
| A case report describes the medical case of 1 particular patient | A case-control study requires 2 groups: 1. Cases: a group of participants who have the outcome (eg. diseased individuals) 2. Controls: a group of participants who do not have the outcome (eg. nondiseased individuals) | |
| Goal | To report an interesting or unusual case of a patient | To look into the past records of these cases and controls in order to determine if the development of the outcome (eg. disease) has to do with an exposure to some risk factor |
| Study type | Observational (because the researcher only observes and describes the patient’s case and does not manipulate or control the events) | Observational (because the researcher does not influence who gets the exposure and who doesn’t) |
| Follow-up over time | Yes, sometimes the case report involves following the patient over a period of time | No, a case-control study is retrospective, meaning that it looks backwards in time to collect information about exposures that happened in the past |
| Example | In 1991, Fred Kern, Jr. reported the case of an 88-year-old man who has been eating 20-30 eggs each day for almost 15 years. The man had a normal cholesterol level as his body adapted to his unusual diet. [ ] | In 1993, Brent et al. compared 67 cases of adolescent suicide with 67 controls (adolescents who were demographically similar to the cases but did not commit suicide) and found that depression, bipolar disorder, substance abuse and conduct disorder were important predictors of adolescent suicide. [ ] |
| Advantages | and : as it involves following 1 patient only | – : because participants are not followed over time – : unlike other designs where we wait for participants to develop the disease, a case-control study works retrospectively: first the cases are chosen, then data about the exposure is collected |
| Limitations | Is considered a weak design because: – It represents a single story that to other cases. – Conclusions based on case reports (because the observed patient is not chosen at random from the population) by some unmeasured factors. | Is a weak design for assessing a causal relationship between exposure and outcome because of: – : the selection of a control group is a complicated task that can easily go wrong and bias the study. – : as the study depends on the memory of the participants to collect information about their exposure. |
| Has the lowest level of evidence of all study designs | A case-control design provides better evidence than the case report (see the evidence pyramid below) |
Here’s the evidence pyramid showing the level of evidence for different study designs:

Further reading
- Case Report: A Beginner’s Guide with Examples
- Case Report vs Cross-Sectional Study
- Cohort vs Cross-Sectional Study
- How to Identify Different Types of Cohort Studies?
- Matched Pairs Design
- Randomized Block Design
- Open access
- Published: 20 June 2024
Association of interleukin-2 and interleukin-10 with the pathophysiology and development of generalized anxiety disorder: a case-control study
- Nisat Sarmin 1 na1 ,
- A. S. M. Roknuzzaman 2 na1 ,
- Rapty Sarker 1 na1 ,
- Mamun -or-Rashid 1 ,
- MMA Shalahuddin Qusar 3 ,
- Sitesh Chandra Bachar 4 ,
- Eva Rahman Kabir 5 ,
- Md. Rabiul Islam 5 &
- Zobaer Al Mahmud 1
BMC Psychiatry volume 24 , Article number: 462 ( 2024 ) Cite this article
Metrics details
Generalized anxiety disorder (GAD) is a devastating mental health condition characterized by constant, uncontrolled worrying. Recent hypotheses indicate that pro-inflammatory cytokines and chemokines are potential contributors to the pathogenesis of GAD. Here, we aimed to assess the role of interleukin-2 (IL-2) and interleukin-10 (IL-10) in the pathophysiology and development of GAD.
This study recruited 50 GAD patients diagnosed according to the DSM-5 criteria and 38 age-sex-matched healthy controls (HCs). A qualified psychiatrist evaluated all study subjects. The socio-demographic and clinical characteristics of the study population were determined using pre-structured questionnaires or interviews, and cytokine serum levels were estimated using commercially available ELISA kits.
We observed reduced serum IL-10 levels in GAD patients compared to HCs (33.69 ± 1.37 pg/ml vs. 44.12 ± 3.16 pg/ml). Also, we observed a significant negative correlation between altered IL-10 levels and GAD-7 scores ( r =-0.315, p = 0.039). Moreover, IL-10 serum measurement exhibited good predictive value in receiver operating characteristics (ROC) analysis with an area under the curve (AUC) value of 0.793 ( p < 0.001) with 80.65% sensitivity and 62.79% specificity at a cutoff value of 33.93 pg/ml. Conversely, we noticed elevated serum IL-2 levels in GAD patients than in HCs (14.81 ± 2.88 pg/ml vs. 8.08 ± 1.1 pg/ml); however, it failed to maintain any significant association with GAD-7 scores, implying that IL-2 might not be involved in GAD pathogenesis. The lower AUC value (0.640; p > 0.05) exhibited by IL-2 serum measurement in ROC analysis further supported that IL-2 might not be associated with GAD.
This study provides new insights into the complex interplay between anti-inflammatory cytokines and GAD pathogenesis. Based on the present findings, we can assume that IL-10 but not IL-2 may be associated with the pathophysiology and development of GAD. However, further research with a larger population size and longitudinal design is required to confirm the potential diagnostic efficacy of IL-10.
Peer Review reports
Generalized anxiety disorder (GAD) is a chronic neuropsychiatric disorder characterized by persistent and excessive uncontrollable fear or worry (occurs for at least 6 months) about various aspects/activities of daily life, affecting the educational, occupational, or social lives of the affected people [ 1 ]. If a person is excessively worried about anything for most days over at least 6 months, he/she is considered to have GAD. Though currently the prevalence rate of GAD is 3–6% worldwide [ 1 , 2 , 3 ], the prevalence is increasing day by day due to the complexity of modern lifestyles and thus warrants attention from national and international authorities to take interventions for mitigating and managing this disorder properly. If it remains undiagnosed or untreated, the uncontrollable and persistently intense anxiety can lead to a marked reduction in cognitive functions or a reduced capacity to work properly in all spheres of life, including educational, family, social, and individual routine work. As such, chronic GAD leads to a reduced quality of life and thereby poses a significant mental health concern globally.
Despite its high prevalence, significant morbidity, and socioeconomic burden, GAD remains poorly characterized in terms of its pathophysiology or effective treatment options. Though the precise cause and mechanism of pathogenesis are still unknown, evidence suggests that multiple factors, including disrupted serotonergic, dopaminergic, and GABAergic neurotransmission and excessive glutamatergic neurotransmission in the brain, genetic factors, family or environmental stress, chronic diseases, hyperthyroidism, childhood trauma, and special personality traits, are linked to GAD. Alterations in monoaminergic neurotransmissions in limbic systems (cingulate gyrus, hippocampus, amygdala, thalamus, and hypothalamus) due to the lower synaptic availability of serotonin, norepinephrine, and dopamine are thought to be associated with anxiety symptoms. Besides, decreased GABA-mediated inhibitory neurotransmission in the amygdala or excessive activation of excitatory glutamatergic neurotransmission are also suggested to be involved in GAD pathology.
Currently, available pharmacotherapies for GAD include selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), pregabalin, and benzodiazepines, which act by reversing these altered monoaminergic neurotransmitter systems. Alongside these drug treatments, non-pharmacological therapies such as several psychological interventions, including cognitive-behavioral therapy, and the acquisition and application of stress management skills, including relaxation and mindfulness skills are also widely used for the management of GAD. However, currently, available pharmacotherapies (SSRIs, SNRIs, pregabalin, and benzodiazepines) have failed to demonstrate the required efficacy in treating anxiety disorders, as 50% of patients failed to respond to these drugs, and at least in 30% of cases, there is a recurrence of the disease following the pharmacological treatment [ 1 , 4 , 5 ]. Moreover, studies reported a higher rate of discontinuity from these pharmacotherapies with low patient adherence or compliance due to the adverse effects, including sexual dysfunction for SSRIs and SNRIs, nausea and dizziness for pregabalin, demonstrating an urgent need for searching for novel anxiolytics [ 3 ]. These findings raised questions about the validity of the currently available mechanism of pathogenesis and suggested that the altered monoaminergic neurotransmitter system might not fully explain the molecular mechanism of GAD development, suggesting other pathophysiological factors might be involved in GAD. Recently, dysregulated immune systems have attracted great interest as an important pathophysiological factor for the development of GAD [ 4 , 6 , 7 , 8 ]. Several clinical and preclinical studies suggest a link between the altered immune system and GAD pathology. Preclinical studies in mice also demonstrated that administration of pro-inflammatory cytokines (including IL-1β, TNF-α, and IL-6) in mice resulted in anxiety-like behaviors that were attenuated or normalized after injecting either anti-inflammatory cytokines or antagonists for the concerned cytokines [ 9 , 10 , 11 , 12 , 13 ]. A recent prospective cohort study conducted by Hou et al., (2019) demonstrated that administration of selective serotonin reuptake inhibitors (escitalopram or sertraline) resulted in a significant reduction in peripheral pro-inflammatory cytokines, and the authors suggested that the anxiolytic effects of these SSRIs might partly be based on their acute anti-inflammatory activities [ 14 ], implicating a significant association between dysregulated peripheral immune systems and GAD development. The development of anxiety-like symptoms in IL-4 gene knock-out mice, reduced levels of IL-4 in anxious mice, and the significant attenuation of anxiety-like behaviors following IL-4 injection demonstrated a positive association between anti-inflammatory cytokines, IL-4 levels, and anxiety pathology [ 15 , 16 , 17 , 18 ]. This immune hypothesis of GAD development is further potentiated by findings from several clinical studies that reported that GAD patients showed significantly higher levels of pro-inflammatory cytokines ( IL-1Ra, IL-1, IL-6, TNF-α, etc.) compared to healthy controls (HCs) [ 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 ] along with decreased levels of anti-inflammatory cytokines, including IL-4 and IL-10 [ 25 ]. Besides, pro-inflammatory cytokines such as TNF-α, and IL-6 were significantly associated with anxiety scores [ 29 ]. Consistent with this, a randomized clinical trial in humans demonstrated that LPS administration resulted in enhanced anxiety scores, and the authors suggested a significant correlation between pro-inflammatory cytokine levels and anxiety severity [ 30 ]. LPS-mediated microglia activation causes enhanced release of excessive pro-inflammatory cytokines in the basolateral amygdala, which ultimately leads to neuroinflammation in mice, resulting in the development of anxiety and depression-like behaviors by modulating neuronal plasticity. The authors found that anxiety pathogenesis was due to the excessive release of excitatory neurotransmitter glutamate from presynaptic axonal terminals of the prefrontal cortex, leading to neuroplasticity [ 31 ]. However, some studies reported either no significant variation in pro-inflammatory or anti-inflammatory cytokine serum levels between GAD patients and HCs [ 32 ] or that pro-inflammatory cytokines including IL-1, IL-2, and IL-6 were significantly reduced in GAD patients than HCs [ 33 , 34 ]. This discrepancy in altered levels of inflammatory cytokines across clinical studies necessitates a further examination of the role of these cytokines in GAD pathophysiology.
Interleukin-2 (IL-2) is one of the major pro-inflammatory cytokines implicated in T cell activation, proliferation, and differentiation and is thus linked to excessive neuro-inflammatory processes [ 35 ]. IL-2 has been shown to impair synaptic plasticity and cause neuroinflammation, which ultimately leads to neuronal damage in neurocircuits associated with fear and anxiety signal transduction. IL-2 was also reported to act as a potent modulator of NMDA and kainite-mediated excitability in mesolimbic or mesostriatal systems [ 36 , 37 , 38 ] and thus affect neuroplasticity. As IL-2 was found to be positively associated with major depressive disorder [ 38 , 39 ], probably, IL-2 might also be correlated with anxiety disorders like GAD, as MDD and GAD are highly co-morbid themselves and thus might share common pathophysiological factors. Recently, a preclinical study conducted by Gilio et al., (2022) observed that IL-2 administration in experimentally healthy mice triggered marked anxiety and depression-like behaviors, and the authors suggested that inhibition of GABA-mediated synaptic inhibitory neurotransmission was involved in the pathology of anxiety [ 40 ].
Interleukin-10 (IL-10) is one of the major anti-inflammatory cytokines that is secreted from Treg cells, Th2 cells, CD4 + T cells, CD8 + T cells, monocytes, macrophages, dendritic cells, B cells, neutrophils in the peripheral nervous system, and from microglia, astrocytes in the central nervous system (CNS) [ 41 ]. IL-10 signaling triggers anti-inflammatory, immunosuppressive, and immunoregulatory activities, including downregulating the production and secretion of pro-inflammatory cytokines and chemokines from activated macrophages, neutrophils, mast cells, Th1 cells, and DCS, decreasing the expression of MHC class II and co-stimulatory molecules on macrophages, and thereby suppressing the antigen presentation capacity of APCS [ 42 , 43 , 44 , 45 , 46 ]. In the CNS, it inhibits the production of such cytokines and chemokines by activated microglia and thereby counteracts cellular and tissue damage in response to excessive neuroinflammation [ 47 , 48 ]. IL-10 has also been shown to stimulate axonal regeneration and activate wound healing through tissue repair [ 48 ]. Research also indicates its role as an inhibitor for microglial hyperactivation in response to LPS-induced inflammatory stimulus [ 49 ]. Based on its anti-inflammatory and immunoregulatory functions, researchers suggested an intricate role for IL-10 in several auto-immune and neuropsychiatric disorders. For example, Mesquita et al., (2008) observed that IL-10 KO mice developed markedly enhanced depressive-like behavior, which was attenuated after IL-10 administration, and that overexpression of IL-10 resulted in reduced depressive behaviors in mice [ 50 ]. Moreover, administration of IL-10 into rats attenuated the pro-inflammatory cytokine IL-1β-induced anxiety-like symptoms in male rats [ 10 ], demonstrating that IL-10 possesses anxiolytic activities. Preclinical research using an experimental animal model also suggests that the observed anxiolytic effect of several anti-anxiety drugs, including 3’-deoxyadenosine (3’-dA), imipramine, fluoxetine, and chlordiazepoxide, stems from their ability to upregulate anti-inflammatory cytokine (IL-4, IL-10) expression in the prefrontal cortex and locus coeruleus and simultaneous down-regulation of proinflammatory cytokine gene expression, leading to a correction of the imbalance between proinflammatory and anti-inflammatory states [ 51 , 52 ]. Though several preclinical studies suggest a potential link between IL-10 levels and anxiety disorder, there is a scarcity of clinical studies aimed at evaluating such an association between IL-10 and GAD development [ 10 ].
Currently, there is no objective and cost-effective diagnostic or prognostic biomarker for GAD, which poses challenges in early diagnosis or risk prediction and leads to misdiagnosis or underdiagnosis, hampering the proper management of the disease. Currently available diagnostic tools, including self-reported symptoms and scoring severity based on the patient’s response to the 7-item questionnaire (GAD-7 scores), are subjective. Though neuroimaging techniques such as positron emission tomography (PET) and functional MRI can be used for the proper and objective diagnosis of GAD, due to their high cost and sophistication or complexities, these diagnostic tools are not suitable for either mass-level screening or are not easy to conduct multiple times to monitor the disease progression or therapeutic drug response. As such, the investigation of cost-effective objective biomarkers for GAD is one of the major focuses of current research on GAD. Finding a suitable biomarker is essential for early diagnosis and initiating psychotherapy and pharmacotherapy as early as possible [ 3 ]. Several studies were performed investigating the potential association between altered pro-inflammatory cytokines or anti-inflammatory cytokines and the pathogenesis of GAD. However, the actual role of inflammatory cytokines in GAD patients is not well explained. Therefore, the present study aims to explore the role of pro-inflammatory cytokines (IL-2) and anti-inflammatory cytokines (IL-10) in the pathophysiology and development of GAD. Also, we aim to find the potential associations of IL-2 and IL-10 with the severity of GAD patients. We believe the present study results would help to understand the pathophysiology and development of GAD.
Study population
We recruited 88 participants for this case-control study (50 GAD patients and 38 HCs matched by age and sex). Patients were collected from the Department of Psychiatry, Bangabandhu Sheikh Mujib Medical University Hospital, Dhaka, Bangladesh, and HCs from nearby areas of Dhaka city. A professional psychiatrist diagnosed patients and evaluated HCs based on DSM-5 criteria. We applied a 7-item GAD scale to assess the severity of anxiety symptoms [ 53 ]. The total scores range from 0 to 21, and it classifies the anxiety severity into four categories: minimal anxiety (0–4 scores), mild anxiety (5–9 scores), moderate anxiety (10–14 scores), and severe anxiety (15–21 scores). We excluded subjects with a co-morbidity of other psychiatric disorders, such as MDD, panic disorder, post-traumatic stress disorder, and social phobia, from the study. Additional exclusion criteria for participants were chronic liver and kidney diseases, infectious diseases, and alcohol or substance abuse. We also excluded patients who were exposed to anxiolytics or antidepressant medications within at least two weeks prior to the study that might have an impact on cytokine levels. We recorded the sociodemographic profile of the study population using a pre-designed questionnaire. The objectives of the study were explained to each participant, and informed written consent was obtained from them before their participation in this study. The study was conducted in accordance with the Declaration of Helsinki.
Blood sample collection and serum isolation
A 5 ml blood sample was collected from the cephalic vein of each participant. The blood samples were kept at room temperature for 1 hour to ensure coagulation and were then subjected to centrifugation at 3000 rpm for 15 minutes at room temperature to collect serum samples. The collected serum was then placed in the Eppendorf tube and stored at -80 °C until further analysis.
Estimation of serum cytokine levels
We estimated the serum levels of IL-2 and IL-10 by ELISA methods (Boster Bio, USA). We followed the manufacturer’s protocol for the ELISA assays. At first, we added 100 µl of standard cytokine solution, samples, and controls to each well of a pre-coated 96-well microplate. The microplates were covered with a plate sealer and incubated for 90 min at 37⁰C. After that, the cover was removed, and the liquid in each well was discarded. Subsequently, 100 µl of biotinylated anti-IL-2 antibody or anti-IL-10 antibody was incorporated into each well and incubated for 60 min at 37⁰C. After discarding the liquid from each well and washing it three times with 300 µl of wash buffer, 100 µl of avidin-biotin-peroxidase complex was added to each well, and the microplate was then again incubated for 30 min at 37⁰C. After the incubation period, the liquid was again discarded, and the plate was washed again with 300 µl of wash buffer five times. Following the addition of 90 µl color-developing reagent (TMB) into each well, the plate was incubated in a dark place for 30 min at RT, followed by the addition of 90 µl of stop solution to each well to stop the reaction process. We measured the absorbance with a microplate reader at 450 nm. We calculated the cytokine levels using standard curves and expressed them as pg/ml.
Data presentation and statistical analysis
GraphPad Prism (version 8.0.1) and Statistical Package for the Social Sciences (version 24.0) were used for data analysis. We used descriptive statistics to find the variations in sociodemographic profiles and clinical characteristics between the groups. A T-test and a Chi-square test were employed to determine the statistical level of significance between the mean differences for variables across patients versus HC groups in the case of continuous variables and categorical variables, respectively. We used boxplot graphs for comparisons of analyzed cytokines between patients and HCs. We also generated scatter plot graphs for several clinical variables in GAD patients to show the correlations among the clinical parameters. A correlation analysis was performed to assess the potential association between several demographic and clinical variables in GAD patients. Receiver operating characteristics (ROC) analysis was conducted to determine the diagnostic efficacy of serum IL-2 or IL-10 levels in discriminating GAD patients from HCs. In all cases, statistical significance was considered at p < 0.05.
Sociodemographic characteristics of the study population
The sociodemographic characteristics of the study population are presented in Table 1 . The GAD patients and HCs were similar in terms of their age, sex, and BMI. Among the participants, about 60% were male and from urban areas. The majority of patients (60.00%) and HCs (68.42%) were unmarried. There was no significant variation between patients and HCs for their education level, occupation, economic status, or smoking status. In contrast, there was a difference between patients and HCs for their family history and previous history of the disease. In GAD patients, 20.00% had a family history, and 40.00% had a previous history of the disease.
Clinical characteristics and laboratory findings
Clinical characteristics and laboratory analysis results are presented in Table 2 . GAD patients displayed markedly higher serum levels of IL-2 (14.81 ± 2.88 pg/ml) compared to HCs (8.08 ± 1.10 pg/ml), and the difference reached the statistically significant level ( p = 0.037, two-tailed unpaired t-test) (Table 2 ; Fig. 1 ). Though male GAD patients exhibited markedly higher levels of IL-2 compared to male HCs ( p = 0.048), there was no significant variation in IL-2 levels between female patients and female HCs ( p > 0.05) (Fig. 1 ). Though some 1.8-fold higher IL-2 serum levels were observed in male GAD patients compared to female GAD patients, the difference did not reach the statistical significance level ( p = 0.198, two-tailed unpaired t-test). In contrast to the results obtained for IL-2, IL-10 showed a statistically significant ( p < 0.001) reduction in GAD patients (33.69 ± 1.37 pg/ml) compared to HCs (44.12 ± 3.16 pg/ml) (Fig. 1 ). Similar to the results obtained for IL-2, IL-10 levels showed a statistically significant difference between patients versus HCs when male people were considered (Fig. 1 ). In contrast, there was no significant variation in IL-10 levels between female GAD patients and female HCs ( p > 0.05).

Distribution of serum IL-2 ( a i ) and IL-10 ( b i ) levels in GAD patients and healthy controls. Comparison of IL-2 and IL-10 levels between GAD patients and their counterparts in control subjects are showed in a i and b i . Comparison of IL-2 and IL-10 levels between male or female GAD patients and their counterparts in control subjects are presented in a ii and b ii
Correlation analysis among different study parameters
We then performed a series of correlation analyses to investigate the association of altered cytokine serum levels with several demographic and clinical variables, such as age, BMI, DSM-5, and GAD-7 scores (Table 3 ). Serum IL-2 levels did not show any positive or negative association with either DSM-5 or GAD-7 scores ( p > 0.05), suggesting that despite its significant enhancement in GAD patients compared to HCs, IL-2 may not associate with GAD pathophysiology. We also observed no significant association between the ages of the patients and IL-2 serum levels. In contrast, the IL-2 levels of GAD patients maintained a significant and positive correlation with BMI levels of patients ( r = 0.390, p < 0.05) which is consistent with the intricate relationship between body mass and enhanced pro-inflammatory responses. Contrary to the results obtained for IL-2, reduced serum IL-10 levels maintained a significant but negative association with both DSM-5 scores ( r =-0.300, p = 0.045) and GAD-7 scores ( r =-0.315, p = 0.039), implicating that altered IL-10 levels are linked to GAD development or pathogenesis. However, the age and BMI levels of GAD patients failed to show any positive or negative association with IL-10 serum levels. Analysis also showed a significant and strong positive association between IL-2 and IL-10 serum levels ( r = 0.471, p = 0.011) in GAD patients, which might be due to the compensatory enhancement of anti-inflammatory cytokine, IL-10 in response to elevated pro-inflammatory cytokine, IL-2 levels. Also, we displayed these correlations among several clinical variables of GAD patients by scatter plot graphs (Fig. 2 ).

Scatter plot graphs for several clinical variables of GAD patients showing existence or absence of correlation between the clinical parameters. Scatter plot for serum IL-2 levels versus GAD-7 scores ( a ) or DSM-5 scores ( b ) expressing no significant association between IL-2 and both clinical parameters. Scatter plot graphs showing significant association between IL-2 levels and BMI ( c ), IL-10 levels and GAD-7 scores ( d ), IL-10 levels and DSM-5 scores and IL-10 and IL-2 levels ( f )
Receiver operating characteristic curve analysis
Serum IL-10 measurement showed a good performance in differentiating GAD patients from HCs, which was evidenced by its significantly higher area under the curve (AUC) value of 0.793 ( p < 0.001) with 80.65% sensitivity and 62.79% specificity at a cut-off value of 33.93 pg/ml, in which the cytokine levels below this point indicate disease states (Table 4 ; Fig. 3 ). ROC analysis of serum IL-2 levels failed to discriminate GAD patients from HCs as the AUC value was below the acceptable range (AUC: 0.640; p = 0.108) with 54.17% sensitivity and 68.18% specificity at a cut-off value of 8.83 pg/ml) (Fig. 3 ; Table 4 ).

Receiver operating characteristic curve (ROC) for serum IL-2 ( a ) and IL-10 levels ( b )
To the best of our knowledge, this is the first case-control study to investigate the potential association between the pathophysiology of GAD and the pro-inflammatory cytokine, IL-2, and the anti-inflammatory cytokine, IL-10, among the Bangladeshi population. We observed that IL-10 serum levels were significantly lower in GAD patients than in HCs, and this reduction was found to be significantly but negatively associated with both DSM-5 scores and GAD-7 scores, demonstrating potential involvement of this anti-inflammatory cytokine in disease severity and symptoms. Our results of a significant reduction in IL-10 levels in GAD patients are in good agreement with those observed in other studies [ 23 , 25 ]. In contrast, our results diverge from those reported by others [ 33 , 54 ] who either reported no significant variation in IL-10 levels between GAD patients and HCs or that IL-10 levels were enhanced in GAD patients compared to HCs. ROC analysis also demonstrated the good predictive value of IL-10 serum measurement in discriminating diseased patients from HCs, suggesting that IL-10 serum level might be a potential biomarker for diagnosis, anti-anxiety drug response monitoring, or disease progression monitoring. Recently, Hou et al. (2019) demonstrated that peripheral serum levels of the pro-inflammatory cytokine IL-6 could be used to monitor the treatment response of SSRIs in GAD [ 14 ]. Similarly, IL-10 might be used as a marker for therapeutic drug monitoring in GAD. However, further longitudinal studies are required to find any causal relationship between IL-10 and disease severity or pathogenesis. On the other hand, serum IL-2 levels were significantly elevated in GAD patients compared to HCs, but they failed to demonstrate any significant association with either DSM-5 scores or GAD-7 scores in Pearson correlation analysis, implying that IL-2 levels might not be associated with the pathophysiology and development of GAD. Consistent with this, ROC analysis showed that IL-2 levels have no significant diagnostic efficacy in differentiating GAD patients from HCs. Further analysis with a larger population size is required to explore the role of IL-2 in the context of GAD severity. Our results are consistent with those reported by Tang et al. (2018), who also observed that GAD patients exhibited significantly higher serum levels of IL-2 compared to HCs [ 19 ]. However, our results are not in agreement with those reported by others who observed either no significant variation in IL-2 levels [ 54 ] or a significant reduction in GAD patients compared to HCs [ 25 , 33 , 34 , 55 ]. We also observed a significant positive correlation between IL-2 and IL-10 levels in GAD patients, which indicates a compensatory mechanism [ 56 ].
Our study provides some valuable insights into the complex and intricate relationship between the dysregulated immune system and GAD. The observed reduction in IL-10 levels in GAD patients in our study suggests a potential immunoregulatory imbalance in GAD, with IL-10 playing a role in modulating anxiety severity. The lack of a significant association between IL-2 serum levels and anxiety severity highlights the nuanced nature of immune dysregulation in GAD, warranting further exploration into the specific mechanisms involved. Elevated levels of pro-inflammatory cytokine, IL-2, and decreased levels of anti-inflammatory cytokine, IL-10, in GAD patients compared to HCs indicate that GAD individuals of the Bangladeshi cohort are characterized by heightened inflammatory responses derived from the imbalance between pro-inflammatory and anti-inflammatory states. Our study finding provides further support for the cytokine hypothesis of anxiety disorder, which proposes that pro-inflammatory cytokine-mediated neuroinflammatory processes can lead to anxiety symptoms or behaviors by downregulating serotonin biosynthesis or enhancing the reuptake of serotonin, resulting in an altered serotonergic neurotransmitter system in the CNS [ 15 ]. The observed significant negative correlation between IL-10 and DSM-5 scores or GAD-7 scores suggests that lowering IL-10 levels might be involved in the pathogenesis of GAD. One of the major implications of our study findings is that IL-10 signaling might be targeted to explore potential novel immunological/immunomodulatory therapies against GAD. The diminished IL-10 levels and their negative correlation with GAD severity suggest a potential avenue for therapeutic intervention. IL-10 might also be used as an anti-inflammatory adjunctive therapy with other pharmacotherapies including SSRIs/SNRIs. However, at this moment, we don’t know the exact mechanism by which lowered levels of IL-10 are linked to higher anxiety severity in GAD patients.
As IL-10 has anti-inflammatory and immunoregulatory activities such as suppression of production of pro-inflammatory cytokines (IL-1β, IL-6, and TNF-α) from microglia and astrocytes, reduction in IL-10 levels in GAD patients in our study led to an imbalance between pro-inflammatory and anti-inflammatory states and resulted in enhanced pro-inflammatory responses, which might be the cause of enhanced anxiety symptoms as inflammatory cytokine-mediated neuroinflammation was reported to be linked with disrupted monoaminergic neurotransmission in the brain. Besides, elevated levels of IL-10 were shown to attenuate anxiety-like behaviors by modulating GABAergic neurotransmission in the amygdala (Patel et al., 2021). IL-10 was also reported to display some neuroprotective activities and has been shown to inhibit neuronal apoptosis and promote neurite outgrowth, axonal outgrowth, and synapse formation in the brain by the JAK1-STAT3 signaling pathway [ 57 ]. In a preclinical study, IL-4 has been shown to cause the shifting of microglia and macrophages from pro-inflammatory to anti-inflammatory neuroprotective phenotypes characterized by excessive production of arginase-1 and PPARγ receptor expression in microglia and macrophage and thereby attenuating brain-injury-mediated anxiety by inhibiting neuronal loss and nerve tracts in the limbic system [ 58 ]. A similar mechanism might be involved in IL-10-mediated anxiety symptom improvement in GAD patients. Further research is required to unravel the exact mechanisms of IL-10-mediated anxiety symptom attenuation in GAD patients.
In terms of diagnostic marker development, as IL-10 serum level measurement demonstrated good performance in discriminating GAD patients from HCs and as IL-10 levels maintained a significant and negative correlation with disease severity, IL-10 serum level raised the possibility of being an objective biomarker for GAD. However, the diagnostic efficacy of this cytokine should be investigated thoroughly using a range of longitudinal studies. Despite this, at this time we can conclude that IL-10 might be used as a risk indicator for assessment of susceptibility to anxiety disorder, resulting in early detection of the disease and prompting the initiation of intervention strategies. This early detection will reduce treatment costs and decrease the prevalence and morbidity associated with this chronic disorder.
The strength of our study is that we designed a set of inclusion and exclusion criteria for the recruitment of participants and followed those criteria in such a way that homogenous population data could be obtained. The strict study design helped us enormously to minimize the potential impact of several confounding variables, including age, sex, BMI, co-morbid diseases, and immunomodulatory drugs, on cytokine levels. However, our study also has some limitations that should be acknowledged. The major limitation of this study is the smaller sample size. We recruited 50 patients and 38 HCs, which does not represent the whole Bangladeshi demographic. It would be better if we could enroll an equal number of cases and controls. For example, we observed that cytokine levels maintained a statistically significant difference between male GAD patients and male HCs. In contrast, no significant variation in cytokine levels was observed when female data were considered. As we have included more male participants (60%) than female participants (40%), the lower sample size of female participants might generate a higher background noise, resulting in lower statistical power, warranting further studies recruiting a larger population size to investigate sex-specific differences in cytokine levels in GAD patients. Our case-control study design is inherently correlational and thus not able to evaluate the causal relationship between altered cytokine levels and GAD. So, at this moment, we cannot conclude whether the altered levels of serum cytokines are the causes of anxiety development or just the outcome of pathophysiological changes.
Longitudinal studies are required to investigate whether altered cytokine levels precede GAD or if it’s just a mere reflection of GAD pathology. Though we have restricted the impacts of several co-variates, other confounding variables, including genetic polymorphism in cytokine genes, the effect of lifestyle or xenobiotics, and dietary habits, were not considered, which might have modulatory effects on serum cytokine levels.
The study provides valuable insights for understanding the pathogenesis of GAD. Despite having elevated IL-2 levels in GAD patients compared to HCs, it failed to demonstrate a significant association with anxiety severity as assessed by GAD-7 scores. In contrast, serum IL-10 levels were significantly reduced in GAD patients compared to HCs and showed a significant negative correlation with anxiety severity, implicating a potential link with the GAD pathophysiology. Our results support the immune hypothesis of GAD development. Our study findings also suggest that IL-10 serum level measurement might offer an objective blood-based biomarker or risk assessment indicator for GAD. We recommend further research employing a larger population size and homogenous data from different areas of Bangladesh to confirm our study findings.
Data availability
All the relevant data and information will be available from the corresponding author upon reasonable request.
Abbreviations
Body mass index
Chronic energy deficiency
Confidence interval
Central nervous system
Diagnostic and statistical manual for mental disorders, 5th edition
Enzyme-linked immunosorbent assay
- Generalized anxiety disorder
Generalized anxiety disorder 7-item scores
Healthy control
- Interleukin-2
- Interleukin-10
Receiver operating characteristic
Standard error mean
Statistical package for social science
Fagan HA, Baldwin DS. Pharmacological treatment of generalised anxiety disorder: current practice and future directions. Expert Rev Neurother. 2023;23(6):535–48. https://doi.org/10.1080/14737175.2023.2211767 .
Article CAS PubMed Google Scholar
Strawn JR, Geracioti L, Rajdev N, Clemenza K, Levine A. Pharmacotherapy for generalized anxiety disorder in adult and pediatric patients: an evidence-based treatment review. Expert Opin Pharmacother. 2018;19(10):1057–70. https://doi.org/10.1080/14656566.2018.1491966 .
Article CAS PubMed PubMed Central Google Scholar
Maron E, Nutt D. Biological markers of generalized anxiety disorder. Dialogues Clin Neurosci. 2017;19(2):147–58. https://doi.org/10.31887/DCNS.2017.19.2/dnutt .
Article PubMed PubMed Central Google Scholar
Costello H, Gould RL, Abrol E, Howard R. Systematic review and meta-analysis of the association between peripheral inflammatory cytokines and generalised anxiety disorder. BMJ Open. 2019;9:e027925. https://doi.org/10.1136/bmjopen-2018-027925 .
Ansara ED. Management of treatment-resistant generalized anxiety disorder. Ment Health Clin. 2020;5(6):326–34. https://doi.org/10.9740/mhc.2020.11.326 .
Article Google Scholar
Michopoulos V, Powers A, Gillespie CF, Ressler KJ, Jovanovic T. Inflammation in fear- and anxiety-based disorders: PTSD, GAD, and beyond. Neuropsychopharmacology. 2017;42:254–70. https://doi.org/10.1038/npp.2016.146 .
Renna ME, O’Toole MS, Spaeth PE, Lekander M, Mennin DS. The association between anxiety,traumatic stress, and obsessive-compulsive disorders and chronic inflammation: A systematic review and meta-analysis. Depress Anxiety. 2018;;35(11):1081–1094. doi: 10.1002/da.22790.
Hou R, Baldwin DS. A neuroimmunological perspective on anxiety disorders. Hum Psychopharmacol. 2012;27(1):6–14.
Zhu CB, Lindler KM, Owens AW, Daws LC, Blakely RD, Hewlett WA. Interleukin-1 receptor activation by systemic lipopolysaccharide induces behavioral despair linked to MAPK regulation of CNS serotonin transporters. Neuropsychopharmacology. 2010;35:2510–20.
Munshi S, Parrilli V, Rosenkranz JA. Peripheral anti-inflammatory cytokine Interleukin-10 treatment mitigates interleukin-1β - induced anxiety and sickness behaviors in adult male rats. Behav Brain Res. 2019;17:372:112024. https://doi.org/10.1016/j.bbr.2019.112024 .
Article CAS Google Scholar
Bercik P, Verdu EF, Foster JA, Macri J, Potter M, Huang X, et al. Chronic gastrointestinal inflammation induces anxiety-like behavior and alters central nervous system biochemistry in mice. Gastroenterology. 2010;139(6):2102–e21121. https://doi.org/10.1053/j.gastro.2010.06.063 .
Gentile A, Fresegna D, Musella A, Sepman H, Bullitta S, De Vito F et al. Interaction between interleukin-1β and type-1 cannabinoid receptor is involved in anxiety-like behavior in experimental autoimmune encephalomyelitis. J Neuroinflammation. 2016;13(1):231. Published 2016 Sep 2. https://doi.org/10.1186/s12974-016-0682-8 .
Haji N, Mandolesi G, Gentile A, Sacchetti L, Fresegna D, Rossi S, et al. TNF-α-mediated anxiety in a mouse model of multiple sclerosis. Exp Neurol. 2012;237(2):296–303. https://doi.org/10.1016/j.expneurol.2012.07.010 .
Hou R, Ye G, Liu Y, Chen X, Pan M, Zhu F, et al. Effects of SSRIs on peripheral inflammatory cytokines in patients with generalized anxiety disorder. Brain Behav Immun. 2019;81:105–10. https://doi.org/10.1016/j.bbi.2019.06.001 .
Quagliato LA, Nardi AE. Cytokine profile in drug-naïve panic disorder patients. Transl Psychiatry. 2022;12(1):75. https://doi.org/10.1038/s41398-022-01835-y . Published 2022 Feb 22.
Lee HJ, Park HJ, Starkweather A, An K, Shim I. Decreased Interleukin-4 release from the neurons of the Locus Coeruleus in response to immobilization stress. Mediators Inflamm. 2016;2016:3501905. https://doi.org/10.1155/2016/3501905 .
Gao T, Li B, Hou Y, Luo S, Feng L, Nie J, et al. Interleukin-4 signalling pathway underlies the anxiolytic effect induced by 3-deoxyadenosine. Psychopharmacology. 2019;236(10):2959–73. https://doi.org/10.1007/s00213-019-5186-7 .
Moon ML, Joesting JJ, Blevins NA, Lawson MA, Gainey SJ, Towers AE, et al. IL-4 knock out mice display anxiety-like Behavior. Behav Genet. 2015;45(4):451–60. https://doi.org/10.1007/s10519-015-9714-x .
Tang Z, Ye G, Chen X, Pan M, Fu J, Fu T, et al. Peripheral proinflammatory cytokines in Chinese patients with generalised anxiety disorder. J Affect Disord. 2018;225:593–8. https://doi.org/10.1016/j.jad.2017.08.082 .
Yang CJ, Liu D, Xu ZS, Shi SX, Du YJ. The pro-inflammatory cytokines, salivary cortisol and alpha-amylase are associated with generalized anxiety disorder (GAD) in patients with asthma. Neurosci Lett. 2017;656:15–21. https://doi.org/10.1016/j.neulet.2017.07.021 .
Vogelzangs N, Beekman AT, de Jonge P, Penninx BW. Anxiety disorders and inflammation in a large adult cohort. Transl Psychiatry. 2013;3(4):e249. https://doi.org/10.1038/tp.2013.27 .
Vieira MM, Ferreira TB, Pacheco PA, Barros PO, Almeida CR, Araújo-Lima CF, et al. Enhanced Th17 phenotype in individuals with generalized anxiety disorder. J Neuroimmunol. 2010;229(1–2):212–8. https://doi.org/10.1016/j.jneuroim.2010.07.018 .
Hou R, Garner M, Holmes C, Osmond C, Teeling J, Lau L, et al. Peripheral inflammatory cytokines and immune balance in generalised anxiety disorder: case-controlled study. Brain Behav Immun. 2017;62:212–8. https://doi.org/10.1016/j.bbi.2017.01.021 .
Copeland WE, Shanahan L, Worthman C, Angold A, Costello EJ. Generalized anxiety and C-reactive protein levels: a prospective, longitudinal analysis. Psychol Med. 2012;42(12):2641–50. https://doi.org/10.1017/S0033291712000554 .
Ferreira TB, Kasahara TM, Barros PO, Vieira MM, Bittencourt VC, Hygino J, et al. Dopamine up-regulates Th17 phenotype from individuals with generalized anxiety disorder. J Neuroimmunol. 2011;238(1–2):58–66. https://doi.org/10.1016/j.jneuroim.2011.06.009 .
Bankier B, Barajas J, Martinez-Rumayor A, Januzzi JL. Association between C-reactive protein and generalized anxiety disorder in stable coronary heart disease patients. Eur Heart J. 2008;29(18):2212–7. https://doi.org/10.1093/eurheartj/ehn326 .
Maes M, Song C, Lin A, De Jongh R, Van Gastel A, Kenis G, et al. The effects of psychological stress on humans: increased production of pro-inflammatory cytokines and a Th1-like response in stress-induced anxiety. Cytokine. 1998;10(4):313–8. https://doi.org/10.1006/cyto.1997.0290 .
Lu H, Yang Q, Zhang Y. The relation of common inflammatory cytokines with anxiety and depression and their values in estimating cardiovascular outcomes in coronary heart disease patients. J Clin Lab Anal. 2022;36(6):e24404. https://doi.org/10.1002/jcla.24404 .
Pitsavos C, Panagiotakos DB, Papageorgiou C, Tsetsekou E, Soldatos C, Stefanadis C. Anxiety in relation to inflammation and coagulation markers, among healthy adults: the ATTICA study. Atherosclerosis. 2006;185(2):320–6. https://doi.org/10.1016/j.atherosclerosis.2005.06.001 .
Lasselin J, Elsenbruch S, Lekander M, Axelsson J, Karshikoff B, Grigoleit JS, et al. Mood disturbance during experimental endotoxemia: predictors of state anxiety as a psychological component of sickness behavior. Brain Behav Immun. 2016;57:30–7. https://doi.org/10.1016/j.bbi.2016.01.003 .
Article PubMed Google Scholar
Zheng ZH, Tu JL, Li XH, Hua Q, Liu WZ, Liu Y, et al. Neuroinflammation induces anxiety- and depressive-like behavior by modulating neuronal plasticity in the basolateral amygdala. Brain Behav Immun. 2021;91:505–18. https://doi.org/10.1016/j.bbi.2020.11.007 .
Mongan D, Raj SS, Föcking M, Byrne JF, Zammit S, Cannon M, et al. Associations between plasma inflammatory markers and psychotic disorder, depressive disorder and generalised anxiety disorder in early adulthood: a nested case-control study. Brain Behav Immun. 2023;111:90–100. https://doi.org/10.1016/j.bbi.2023.03.025 .
Shen Z, Cui L, Mou S, Ren L, Yuan Y, Shen X, et al. Combining S100B and cytokines as neuro-inflammatory biomarkers for diagnosing generalized anxiety disorder: a proof-of-Concept Study based on machine learning. Front Psychiatry. 2022;13:881241. https://doi.org/10.3389/fpsyt.2022.881241 . Published 2022 Jun 22.
Wagner EN, Strippoli MF, Ajdacic-Gross V, Gholam-Rezaee M, Glaus J, Vandeleur C, et al. Generalized anxiety disorder is prospectively Associated with decreased levels of Interleukin-6 and Adiponectin among individuals from the community. J Affect Disord. 2020;270:114–7. https://doi.org/10.1016/j.jad.2020.03.123 .
Ross SH, Cantrell DA. Signaling and function of Interleukin-2 in T lymphocytes. Annu Rev Immunol. 2018;36:411–33. https://doi.org/10.1146/annurev-immunol-042617-053352 .
Ye JH, Tao L, Zalcman SS. Interleukin-2 modulates N-methyl-D-aspartate receptors of native mesolimbic neurons. Brain Res. 2001;894(2):241–8. https://doi.org/10.1016/s0006-8993(01)02056-x .
Ye JH, Zalcman SS, Tao L. Kainate-activated currents in the ventral tegmental area of neonatal rats are modulated by interleukin-2. Brain Res. 2005;1049(2):227–33. https://doi.org/10.1016/j.brainres.2005.05.016 .
Suhee FI, Shahriar M, Islam SMA, Bhuiyan MA, Islam MR. Elevated serum IL-2 levels are Associated with Major Depressive disorder: a case-control study. Clin Pathol. 2023;16:2632010X231180797. https://doi.org/10.1177/2632010X231180797 .
Köhler CA, Freitas TH, Maes M, de Andrade NQ, Liu CS, Fernandes BS, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–87. https://doi.org/10.1111/acps.12698 .
Gilio L, Fresegna D, Gentile A, Guadalupi L, Sanna K, De Vito F, et al. Preventive exercise attenuates IL-2-driven mood disorders in multiple sclerosis. Neurobiol Dis. 2022;172:105817. https://doi.org/10.1016/j.nbd.2022.105817 .
Carlini V, Noonan DM, Abdalalem E, Goletti D, Sansone C, Calabrone L, et al. The multifaceted nature of IL-10: regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions. Front Immunol. 2023;14:1161067. https://doi.org/10.3389/fimmu.2023.1161067 . Published 2023 Jun 8.
Fiorentino DF, Bond MW, Mosmann TR. Two types of mouse T helper cell. IV. Th2 clones secrete a factor that inhibits cytokine production by Th1 clones. J Exp Med. 1989;170(6):2081–95. https://doi.org/10.1084/jem.170.6.2081 .
Fiorentino DF, Zlotnik A, Mosmann TR, Howard M, O’Garra A. IL-10 inhibits cytokine production by activated macrophages. J Immunol. 1991;147(11):3815–22.
Fiorentino DF, Zlotnik A, Vieira P, Mosmann TR, Howard M, Moore KW, et al. IL-10 acts on the antigen-presenting cell to inhibit cytokine production by Th1 cells. J Immunol. 1991;146(10):3444–51.
Bogdan C, Vodovotz Y, Nathan C. Macrophage deactivation by interleukin 10. J Exp Med. 1991;174(6):1549–55. https://doi.org/10.1084/jem.174.6.1549 .
Murray PJ. The primary mechanism of the IL-10-regulated antiinflammatory response is to selectively inhibit transcription. Proc Natl Acad Sci U S A. 2005;102(24):8686–91. https://doi.org/10.1073/pnas.0500419102 .
Lobo-Silva D, Carriche GM, Castro AG, Roque S, Saraiva M. Balancing the immune response in the brain: IL-10 and its regulation. J Neuroinflammation. 2016;13(1):297. https://doi.org/10.1186/s12974-016-0763-8 .
Saraiva M, Vieira P, O’Garra A. Biology and therapeutic potential of interleukin-10. J Exp Med. 2020;217(1):e20190418. https://doi.org/10.1084/jem.20190418 .
Shemer A, Scheyltjens I, Frumer GR, Kim JS, Grozovski J, Ayanaw S, et al. Interleukin-10 prevents pathological Microglia Hyperactivation following Peripheral Endotoxin Challenge. Immunity. 2020;53(5):1033–e10497. https://doi.org/10.1016/j.immuni.2020.09.018 .
Mesquita AR, Correia-Neves M, Roque S, Castro AG, Vieira P, Pedrosa J, et al. IL-10 modulates depressive-like behavior. J Psychiatr Res. 2008;43(2):89–97. https://doi.org/10.1016/j.jpsychires.2008.02.004 .
Obuchowicz E, Bielecka AM, Paul-Samojedny M, Pudełko A, Kowalski J. Imipramine and fluoxetine inhibit LPS-induced activation and affect morphology of microglial cells in the rat glial culture. Pharmacol Rep. 2014;66(1):34–43. https://doi.org/10.1016/j.pharep.2013.08.002 .
Blatteau JE, de Maistre S, Lambrechts K, Abraini J, Risso JJ, Vallée N. Fluoxetine stimulates anti-inflammatory IL-10 cytokine production and attenuates sensory deficits in a rat model of decompression sickness. J Appl Physiol (1985). 2015;119(12):1393–9. https://doi.org/10.1152/japplphysiol.00602.2015 .
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092 .
Tofani T, Mannelli LD, Zanardelli M, et al. An immunologic profile study in drug-naive generalized anxiety non depressed patients: a pilot study. Eur Neuropsychopharmacol. 2015;25(suppl 2):S226.
Koh KB, Lee BK. Reduced lymphocyte proliferation and interleukin-2 production in anxiety disorders. Psychosom Med. 1998;60(4):479–83.
Inaba A, Tuong ZK, Zhao TX, et al. Low-dose IL-2 enhances the generation of IL-10-producing immunoregulatory B cells. Nat Commun. 2023;14(1):2071. https://doi.org/10.1038/s41467-023-37424-w . Published 2023 Apr 12.
Chen H, Lin W, Zhang Y, Lin L, Chen J, Zeng Y, et al. IL-10 promotes neurite outgrowth and synapse formation in cultured cortical neurons after the oxygen-glucose deprivation via JAK1/STAT3 pathway. Sci Rep. 2016;6:30459. https://doi.org/10.1038/srep30459 . Published 2016 Jul 26.
Pu H, Wang Y, Yang T, Leak RK, Stetler RA, Yu F, et al. Interleukin-4 mitigates anxiety-like behavior and loss of neurons and fiber tracts in limbic structures in a microglial PPARγ-dependent manner after traumatic brain injury. Neurobiol Dis. 2023;180:106078. https://doi.org/10.1016/j.nbd.2023.106078 .
Download references
Acknowledgements
The authors are thankful to all the participants of this study. They are also thankful to the staff and physicians at the Department of Psychiatry, BSMMU, for their technical and administrative support. The authors are also thankful for the laboratory support provided by the Department of Pharmacy, University of Asia Pacific, Dhaka Bangladesh.
This research received no specific grant from any funding agency. However, we received partial funding from University of Dhaka, Bangladesh (Centennial Research grant (2nd Phase) for the year of 2020–2021, project title: “Investigation of peripheral pro-inflammatory and anti-inflammatory cytokines and immune balance in Bangladeshi patients with Generalized Anxiety Disorder”).
Author information
Nisat Sarmin, A. S. M. Roknuzzaman and Rapty Sarker contributed equally to this work.
Authors and Affiliations
Department of Clinical Pharmacy and Pharmacology, Faculty of Pharmacy, University of Dhaka, Dhaka, 1000, Bangladesh
Nisat Sarmin, Rapty Sarker, Mamun -or-Rashid & Zobaer Al Mahmud
Department of Pharmacy, University of Asia Pacific, Dhaka, 1205, Bangladesh
A. S. M. Roknuzzaman
Department of Psychiatry, Bangabandhu Sheikh Mujib Medical University, Shahabagh, Dhaka, 1000, Bangladesh
MMA Shalahuddin Qusar
Department of Pharmacy, Faculty of Pharmacy, University of Dhaka, Dhaka, 1000, Bangladesh
Sitesh Chandra Bachar
School of Pharmacy, BRAC University, Kha 224 Bir Uttam Rafiqul Islam Avenue, Merul Badda, Dhaka, 1212, Bangladesh
Eva Rahman Kabir & Md. Rabiul Islam
You can also search for this author in PubMed Google Scholar
Contributions
NS, ASMR, RS, MRI, and ZAM: Conceptualization, Data curation, Investigation, Writing – original draft. MR, MMASQ, SCB, and ZAM: Funding acquisition, Project administration, Validation. ERK, MRI, and ZAM: Conceptualization, Formal analysis, Methodology, Supervision, Writing – review & editing.
Corresponding authors
Correspondence to Md. Rabiul Islam or Zobaer Al Mahmud .
Ethics declarations
Ethics approval and consent to participate.
The research protocol was approved by the Research Ethics Committee (REC) of the University of Asia Pacific, Dhaka, Bangladesh (Ref: UAP/REC/2023/202-S). We briefed the objectives of the study to the participants, and informed consent was obtained from each of them. We conducted this investigation following the Helsinki Declaration’s guiding principles.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Sarmin, N., Roknuzzaman, A.S.M., Sarker, R. et al. Association of interleukin-2 and interleukin-10 with the pathophysiology and development of generalized anxiety disorder: a case-control study. BMC Psychiatry 24 , 462 (2024). https://doi.org/10.1186/s12888-024-05911-z
Download citation
Received : 31 December 2023
Accepted : 13 June 2024
Published : 20 June 2024
DOI : https://doi.org/10.1186/s12888-024-05911-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Mental disorders
BMC Psychiatry
ISSN: 1471-244X
- Submission enquiries: [email protected]
- General enquiries: [email protected]
- Share full article
For more audio journalism and storytelling, download New York Times Audio , a new iOS app available for news subscribers.

- Apple Podcasts
- Google Podcasts
America’s Top Doctor on Why He Wants Warning Labels on Social Media
The surgeon general says parents should be aware that using the platforms might harm adolescents’ mental health..

Hosted by Sabrina Tavernise
Produced by Lynsea Garrison , Rob Szypko , Alex Stern and Rikki Novetsky
Edited by Lexie Diao and Michael Benoist
Original music by Dan Powell and Chelsea Daniel
Engineered by Alyssa Moxley
Listen and follow The Daily Apple Podcasts | Spotify | Amazon Music | YouTube
Warning: This episode contains mentions of bullying and suicide.
A rising tide of mental health problems among teenagers has sent parents, teachers and doctors searching for answers. This week, the U.S. surgeon general, Dr. Vivek H. Murthy, offered one: social media.
Today, Dr. Murthy discusses his proposal to require platforms such as YouTube, TikTok and Instagram to include warning labels, like those that appear on tobacco and alcohol products.
On today’s episode
Dr. Vivek H. Murthy , the U.S. surgeon general.

Background reading
Dr. Murthy cannot unilaterally impose warnings on social media; the action requires approval by Congress .
Read a guest essay by Dr. Murthy: Why I’m Calling for a Warning Label on Social Media Platforms .
There are a lot of ways to listen to The Daily. Here’s how.
We aim to make transcripts available the next workday after an episode’s publication. You can find them at the top of the page.
The Daily is made by Rachel Quester, Lynsea Garrison, Clare Toeniskoetter, Paige Cowett, Michael Simon Johnson, Brad Fisher, Chris Wood, Jessica Cheung, Stella Tan, Alexandra Leigh Young, Lisa Chow, Eric Krupke, Marc Georges, Luke Vander Ploeg, M.J. Davis Lin, Dan Powell, Sydney Harper, Mike Benoist, Liz O. Baylen, Asthaa Chaturvedi, Rachelle Bonja, Diana Nguyen, Marion Lozano, Corey Schreppel, Rob Szypko, Elisheba Ittoop, Mooj Zadie, Patricia Willens, Rowan Niemisto, Jody Becker, Rikki Novetsky, John Ketchum, Nina Feldman, Will Reid, Carlos Prieto, Ben Calhoun, Susan Lee, Lexie Diao, Mary Wilson, Alex Stern, Sophia Lanman, Shannon Lin, Diane Wong, Devon Taylor, Alyssa Moxley, Summer Thomad, Olivia Natt, Daniel Ramirez and Brendan Klinkenberg.
Our theme music is by Jim Brunberg and Ben Landsverk of Wonderly. Special thanks to Sam Dolnick, Paula Szuchman, Lisa Tobin, Larissa Anderson, Julia Simon, Sofia Milan, Mahima Chablani, Elizabeth Davis-Moorer, Jeffrey Miranda, Maddy Masiello, Isabella Anderson, Nina Lassam and Nick Pitman.
An earlier version of this episode misstated one of Donald Sutherland’s most notable roles. He starred in the film M*A*S*H, not the television series that followed.
How we handle corrections
Advertisement
Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Article Menu

- Subscribe SciFeed
- Recommended Articles
- Google Scholar
- on Google Scholar
- Table of Contents
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
JSmol Viewer
A comparison between 2-octyl cyanoacrylate and conventional suturing for the closure of epiblepharon incision wounds in children: a retrospective case–control study.

1. Introduction
2. materials and methods, 2.1. technique, 2.2. postoperative care instructions, 2.3. patient-reported outcomes, 2.4. statistical analysis, 4. discussion, 5. conclusions, supplementary materials, author contributions, institutional review board statement, informed consent statement, data availability statement, conflicts of interest.
- Johnson, C.C. Epiblepharon. Am. J. Ophthalmol. 1968 , 66 , 1172–1175. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Levitt, J.M. Epiblepharon and congenital entropion. Am. J. Ophthalmol. 1957 , 44 , 112–113. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Sundar, G.; Young, S.M.; Tara, S.; Tan, A.M.; Amrith, S. Epiblepharon in East Asian patients: The singapore experience. Ophthalmology 2010 , 117 , 184–189. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Kim, N.M.; Jung, J.H.; Choi, H.Y. The effect of epiblepharon surgery on visual acuity and with-the-rule astigmatism in children. Korean J. Ophthalmol. 2010 , 24 , 325–330. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Khwarg, S.I.; Lee, Y.J. Epiblepharon of the lower eyelid: Classification and association with astigmatism. Korean J. Ophthalmol. 1997 , 11 , 111–117. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Quickert, M.H.; Rathbun, E. Suture repair of entropion. Arch. Ophthalmol. 1971 , 85 , 304–305. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Greene, D.; Koch, R.J.; Goode, R.L. Efficacy of octyl-2-cyanoacrylate tissue glue in blepharoplasty. A prospective controlled study of wound-healing characteristics. Arch. Facial Plast Surg. 1999 , 1 , 292–296. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Leung, G.Y.; Peponis, V.; Varnell, E.D.; Lam, D.S.; Kaufman, H.E. Preliminary in vitro evaluation of 2-octyl cyanoacrylate (dermabond) to seal corneal incisions. Cornea 2005 , 24 , 998–999. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Farion, K.; Osmond, M.H.; Hartling, L.; Russell, K.; Klassen, T.; Crumley, E.; Wiebe, N. Tissue adhesives for traumatic lacerations in children and adults. Cochrane Database Syst. Rev. 2002 , 2002 , Cd003326. [ Google Scholar ] [ CrossRef ]
- Tandon, S.; Smale, M.; Pacilli, M.; Nataraja, R.M. Tissue adhesive and adhesive tape for pediatric wound closure: A systematic review and meta-analysis. J. Pediatr. Surg. 2021 , 56 , 1020–1029. [ Google Scholar ] [ CrossRef ]
- Collin, T.W.; Blyth, K.; Hodgkinson, P.D. Cleft lip repair without suture removal. J. Plast. Reconstr. Aesthet. Surg. 2009 , 62 , 1161–1165. [ Google Scholar ] [ CrossRef ]
- Singer, A.J.; Hollander, J.E.; Quinn, J.V. Evaluation and management of traumatic lacerations. N. Engl. J. Med. 1997 , 337 , 1142–1148. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Gierek, M.; Merkel, K.; Ochała-Gierek, G.; Niemiec, P.; Szyluk, K.; Kuśnierz, K. Which Suture to Choose in Hepato-Pancreatic-Biliary Surgery? Assessment of the Influence of Pancreatic Juice and Bile on the Resistance of Suturing Materials-In Vitro Research. Biomedicines 2022 , 10 , 1053. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Regula, C.G.; Yag-Howard, C. Suture Products and Techniques: What to Use, Where, and Why. Dermatol. Surg. 2015 , 41 (Suppl. S10), S187–S200. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Meskin, S.W.; Ritterband, D.C.; Shapiro, D.E.; Kusmierczyk, J.; Schneider, S.S.; Seedor, J.A.; Koplin, R.S. Liquid bandage (2-octyl cyanoacrylate) as a temporary wound barrier in clear corneal cataract surgery. Ophthalmology 2005 , 112 , 2015–2021. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Warder, D.; Kratky, V. Fixation of extraocular muscles to porous orbital implants using 2-ocetyl-cyanoacrylate glue. Ophthalmic. Plast. Reconstr. Surg. 2015 , 31 , 275–277. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Haslinda, A.R.; Azhany, Y.; Noor-Khairul, R.; Zunaina, E.; Liza-Sharmini, A.T. Cyanoacrylate tissue glue for wound repair in early posttrabeculectomy conjunctival bleb leak: A case series. Int. Med. Case Rep. J. 2015 , 8 , 145–150. [ Google Scholar ] [ CrossRef ]
- Okabe, M.; Kitagawa, K.; Yoshida, T.; Koike, C.; Katsumoto, T.; Fujihara, E.; Nikaido, T. Application of 2-octyl-cyanoacrylate for corneal perforation and glaucoma filtering bleb leak. Clin. Ophthalmol. 2013 , 7 , 649–653. [ Google Scholar ] [ CrossRef ]
- McKinley, S.H.; Yen, M.T. Octyl-2-cyanoacrylate tissue adhesive in external dacryocystorhinostomy. Ophthalmic. Plast. Reconstr. Surg. 2005 , 21 , 197–200. [ Google Scholar ] [ CrossRef ]
- Woo, K.I.; Yi, K.; Kim, Y.D. Surgical correction for lower lid epiblepharon in Asians. Br. J. Ophthalmol. 2000 , 84 , 1407–1410. [ Google Scholar ] [ CrossRef ]
- Quinn, J.V.; Drzewiecki, A.E.; Stiell, I.G.; Elmslie, T.J. Appearance scales to measure cosmetic outcomes of healed lacerations. Am. J. Emerg. Med. 1995 , 13 , 229–231. [ Google Scholar ] [ CrossRef ]
- Peñarrocha-Oltra, D.; Candel-Martí, E.; Peñarrocha-Diago, M.; Martínez-González, J.M.; Aragoneses, J.M.; Peñarrocha-Diago, M. Palatal positioning of implants in severely atrophic edentulous maxillae: Five-year cross-sectional retrospective follow-up study. Int. J. Oral Maxillofac. Implant. 2013 , 28 , 1140–1146. [ Google Scholar ] [ CrossRef ]
- US Food and Drug Administration. FDA Dermabond Approval Order. Available online: http://www.accessdata.fda.gov/cdrh_docs/pdf/P960052b.pdf (accessed on 10 February 2024).
- Sanders, L.; Nagatomi, J. Clinical applications of surgical adhesives and sealants. Crit. Rev. Biomed. Eng. 2014 , 42 , 271–292. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Mertz, P.M.; Davis, S.C.; Cazzaniga, A.L.; Drosou, A.; Eaglstein, W.H. Barrier and Antibacterial Properties of 2-Octyl Cyanoacrylate-Derived Wound Treatment Films. J. Cutan. Med. Surg. 2003 , 7 , 1–6. [ Google Scholar ] [ CrossRef ]
- Bruns, T.B.; Simon, H.K.; McLario, D.J.; Sullivan, K.M.; Wood, R.J.; Anand, K.J. Laceration repair using a tissue adhesive in a children’s emergency department. Pediatrics 1996 , 98 , 673–675. [ Google Scholar ]
- Quinn, J.V.; Drzewiecki, A.; Li, M.M.; Stiell, I.G.; Sutcliffe, T.; Elmslie, T.J.; Wood, W.E. A randomized, controlled trial comparing a tissue adhesive with suturing in the repair of pediatric facial lacerations. Ann. Emerg. Med. 1993 , 22 , 1130–1135. [ Google Scholar ] [ CrossRef ]
- Resch, K.L.; Hick, J.L. Preliminary experience with 2-octylcyanoacrylate in a pediatric emergency department. Pediatr. Emerg. Care 2000 , 16 , 328–331. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Taravella, M.J.; Chang, C.D. 2-Octyl cyanoacrylate medical adhesive in treatment of a corneal perforation. Cornea 2001 , 20 , 220–221. [ Google Scholar ] [ CrossRef ]
- Reyniers, R.; Boekhoorn, S.; Veckeneer, M.; van Meurs, J. A case-control study of beneficial and adverse effects of 2-octyl cyanoacrylate tissue adhesive for episcleral explants in retinal detachment surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2012 , 250 , 311–312. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Ricci, B.; Ricci, F. Octyl 2-cyanoacrylate tissue adhesive in experimental scleral buckling. Acta Ophthalmol. Scand. 2001 , 79 , 506–508. [ Google Scholar ] [ CrossRef ]
- Gupta, B.K.; Edward, D.; Duffy, M.T. 2-Octyl cyanoacrylate tissue adhesive and muscle attachment to porous anophthalmic orbital implants. Ophthalmic. Plast Reconstr. Surg. 2001 , 17 , 264–269. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Perin, L.F.; Helene, A., Jr.; Fraga, M.F. Sutureless closure of the upper eyelids in blepharoplasty: Use of octyl-2-cyanoacrylate. Aesthet. Surg. J. 2009 , 29 , 87–92. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- James, R.; Alejandro-Rodriquez, M.; Perez, E.; Mangel, J. 2-octyl cyanoacrylate skin adhesive for topical skin incision closure in female pelvic surgery. Open J. Obstet. Gynecol. 2015 , 5 , 280–285. [ Google Scholar ] [ CrossRef ]
- US Food and Drug Administration. FDA Surgiseal Topical Skin Adhesive Approval. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/K161011.pdf (accessed on 8 November 2023).
- Petrie, E. Cyanoacrylate Adhesives in Surgical Applications. Rev. Adhes. Adhes. 2014 , 2 , 253–310. [ Google Scholar ] [ CrossRef ]
- Lee, D.P.; Kim, S.D.; Hu, Y.J. Change of visual acuity and astigmatism after operation in epiblepharon children. J. Korean Ophthalmol. Soc. 2001 , 42 , 223–227. [ Google Scholar ]
- Kim, M.S.; Lee, D.S.; Woo, K.I.; Chang, H.R. Changes in astigmatism after surgery for epiblepharon in highly astigmatic children: A controlled study. J. AAPOS 2008 , 12 , 597–601. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Ahn, H.B.; Shin, D.M.; Roh, M.S.; Jeung, W.J.; Park, W.C.; Rho, S.H. A comparison of 2-octyl cyanoacrylate adhesives versus conventional suture materials for eyelid wound closure in rabbits. Korean J. Ophthalmol. 2011 , 25 , 121–127. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Leahey, A.B.; Gottsch, J.D. Symblepharon associated with cyanoacrylate tissue adhesive. Arch. Ophthalmol. 1993 , 111 , 168. [ Google Scholar ] [ CrossRef ]
- Strempel, I. Complications by liquid plastics in ophthalmic surgery. Histopathologic study. Dev. Ophthalmol. 1987 , 13 , 137–146. [ Google Scholar ] [ CrossRef ]
- Cavanaugh, T.B.; Gottsch, J.D. Infectious keratitis and cyanoacrylate adhesive. Am. J. Ophthalmol. 1991 , 111 , 466–472. [ Google Scholar ] [ CrossRef ]
- Tsai, Y.-C.; Huang, D.-W.; Chou, Y.-Y.; An, Y.-C.; Cheng, Y.-S.; Chen, P.-H.; Tzeng, Y.-S. Comparative Evaluation of Tissue Adhesives and Sutures in the Management of Facial Laceration Wounds in Children. J. Pers. Med. 2023 , 13 , 1350. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Martín-García, R.F.; Janer, A.L.; Rullán, F.V. Octyl-2-cyanoacrylate liquid bandage as a wound dressing in facial excisional surgery: Results of an uncontrolled pilot study. Dermatol. Surg. 2005 , 31 , 670–673. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Fontana, S.; Schiestl, C.M.; Landolt, M.A.; Staubli, G.; von Salis, S.; Neuhaus, K.; Mohr, C.; Elrod, J. A Prospective Controlled Study on Long-Term Outcomes of Facial Lacerations in Children. Front. Pediatr. 2020 , 8 , 616151. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Osmond, M.H.; Klassen, T.P.; Quinn, J.V. Economic comparison of a tissue adhesive and suturing in the repair of pediatric facial lacerations. J. Pediatr. 1995 , 126 , 892–895. [ Google Scholar ] [ CrossRef ] [ PubMed ]
Click here to enlarge figure
| Characteristic | Group A | Group B | p Value |
|---|---|---|---|
| Gender | |||
| Male | 5 | 5 | |
| Female | 5 | 5 | |
| Mean age at operation (years) | 7.9 ± 2.2 | 7.2 ± 4.2 | 0.303 |
| Average body mass index (kg/m ) | 18.97 ± 4.18 | 17.55 ± 4.85 | 0.335 |
| Side of epiblepharon | |||
| Unilateral | 0 | 2 | |
| Bilateral | 10 | 8 | |
| Mean operation time (per eye) (minutes) | 27.6 ± 7.7 | 30.9 ± 10.0 | 0.334 |
| Associated ocular disease (eyes) | |||
| Amblyopia | 2 (3) | 3 (6) | |
| Strabismus | 0 | 2 (4) | |
| Congenital ptosis | 0 | 1 (1) | |
| Astigmatism (>1 diopter) | 6 (10) | 8 (15) | |
| High astigmatism (>3 diopter) | 1 (2) | 2 (4) | |
| Myopia | 4 (8) | 4 (8) | |
| Preoperative BCVA (logMAR) | 0.19 ± 0.21 | 0.18 ± 0.07 | 0.568 |
| Postoperative BCVA (logMAR) | 0.05 ± 0 | 0.11 ± 0.03 | 0.442 |
| Mean follow-up time (months) | 1.5 ± 0.9 | 5.8 ± 6.9 | 0.463 |
| Group A | Group B | Z * | p Value | |
|---|---|---|---|---|
| Esthetic outcomes | 9 ± 0.82 | 8.9 ± 0.74 | −0.284 | 0.776 |
| Symptom relief | 9.6 ± 0.52 | 9.5 ± 0.53 | −0.438 | 0.661 |
| Ease of postoperative care | 9.1 ± 0.74 | 6.9 ± 0.99 | −3.629 | <0.001 |
| General satisfaction | 9.1 ± 0.32 | 8.1 ± 0.57 | −3.482 | <0.001 |
| The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Share and Cite
Hsu, C.-C.; Lee, L.-C.; Chang, H.-C.; Chen, Y.-H.; Hsieh, M.-W.; Chien, K.-H. A Comparison between 2-Octyl Cyanoacrylate and Conventional Suturing for the Closure of Epiblepharon Incision Wounds in Children: A Retrospective Case–Control Study. J. Clin. Med. 2024 , 13 , 3475. https://doi.org/10.3390/jcm13123475
Hsu C-C, Lee L-C, Chang H-C, Chen Y-H, Hsieh M-W, Chien K-H. A Comparison between 2-Octyl Cyanoacrylate and Conventional Suturing for the Closure of Epiblepharon Incision Wounds in Children: A Retrospective Case–Control Study. Journal of Clinical Medicine . 2024; 13(12):3475. https://doi.org/10.3390/jcm13123475
Hsu, Chia-Chen, Lung-Chi Lee, Hsu-Chieh Chang, Yi-Hao Chen, Meng-Wei Hsieh, and Ke-Hung Chien. 2024. "A Comparison between 2-Octyl Cyanoacrylate and Conventional Suturing for the Closure of Epiblepharon Incision Wounds in Children: A Retrospective Case–Control Study" Journal of Clinical Medicine 13, no. 12: 3475. https://doi.org/10.3390/jcm13123475
Article Metrics
Article access statistics, supplementary material.
ZIP-Document (ZIP, 115 KiB)
Further Information
Mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
- Open access
- Published: 12 June 2024
Risk factors for neonatal hypoxic ischemic encephalopathy and therapeutic hypothermia: a matched case-control study
- Suoma Roto 1 ,
- Irmeli Nupponen 2 ,
- Ilkka Kalliala 1 &
- Marja Kaijomaa ORCID: orcid.org/0000-0003-2180-1483 1
BMC Pregnancy and Childbirth volume 24 , Article number: 421 ( 2024 ) Cite this article
222 Accesses
2 Altmetric
Metrics details
Peripartum asphyxia is one of the main causes of neonatal morbidity and mortality. In moderate and severe cases of asphyxia, a condition called hypoxic-ischemic encephalopathy (HIE) and associated permanent neurological morbidities may follow. Due to the multifactorial etiology of asphyxia, it may be difficult prevent, but in term neonates, therapeutic cooling can be used to prevent or reduce permanent brain damage. The aim of this study was to assess the significance of different antenatal and delivery related risk factors for moderate and severe HIE and the need for therapeutic hypothermia.
We conducted a retrospective matched case-control study in Helsinki University area hospitals during 2013–2017. Newborn singletons with moderate or severe HIE and the need for therapeutic hypothermia were included. They were identified from the hospital database using ICD-codes P91.00, P91.01 and P91.02. For every newborn with the need for therapeutic hypothermia the consecutive term singleton newborn matched by gender, fetal presentation, delivery hospital, and the mode of delivery was selected as a control. Odds ratios (OR) between obstetric and delivery risk factors and the development of HIE were calculated.
Eighty-eight cases with matched controls met the inclusion criteria during the study period. Maternal and infant characteristics among cases and controls were similar, but smoking was more common among cases (aOR 1.46, CI 1.14–1.64, p = 0.003). The incidence of preeclampsia, diabetes and intrauterine growth restriction in groups was equal. Induction of labour (aOR 3.08, CI 1.18–8.05, p = 0.02) and obstetric emergencies (aOR 3.51, CI 1.28–9.60, p = 0.015) were more common in the case group. No difference was detected in the duration of the second stage of labour or the delivery analgesia.
Conclusions
Smoking, induction of labour and any obstetric emergency, especially shoulder dystocia, increase the risk for HIE and need for therapeutic hypothermia. The decisions upon induction of labour need to be carefully weighed, since maternal smoking and obstetric emergencies can hardly be controlled by the clinician.
Peer Review reports
Peripartum asphyxia, generally referred to as birth asphyxia, is one of the main causes of neonatal mortality worldwide [ 1 ]. Approximately three to five newborns per 1000 live births in developed countries are affected by birth asphyxia [ 2 ]. This condition of hypoxia and acidemia can develop gradually during pregnancy and lead to an emergency cesarean section when detected. It can also develop abruptly when complications during labour occur [ 3 ].
The pathophysiology of birth asphyxia and its multifactorial antecedents are well studied and recognized: An increased risk is associated with maternal health problems such as diabetes mellitus, cholestasis of pregnancy, anemia, and hypertension, as well as fetal conditions like intrauterine growth restriction and infections [ 4 , 5 ]. Extensive effort is made to screen and follow-up these mothers and pregnancies with known obstetric risk factors for development of birth asphyxia.
The clinical signs associated with birth asphyxia may be transient and reversible or lead to permanent neurological impairment or death [ 6 ]. A condition called hypoxic-ischemic encephalopathy may follow and, if diagnosed, can further be divided in mild, moderate, and severe [ 7 ]. A quick recovery, normal level of consciousness, mild neurological signs and absence of seizures are typical to a mild HIE, whereas moderate and severe HIE include presence of seizures, multiorgan failure, primitive reflexes and altered level of consciousness and tone [ 7 ]. The diagnosis of severe birth asphyxia is set when the neonate presents with a five-minute Apgar score of 0 to 3 and a pH of 7.0 or less in the umbilical artery blood sample [ 4 ].
In the severe cases of birth asphyxia, HIE predisposes the resuscitated neonate to permanent neurologic morbidities such as cerebral palsy, epilepsy, and developmental delays. The medical intervention to reduce brain damage in term neonates with moderate and severe HIE is therapeutic hypothermia, i.e., cooling of the neonates to around 33 °C for three days [ 8 ].
Despite the high-quality maternal care and the recognition of antenatal risks, birth asphyxia and HIE remain a challenge in perinatal care. Due to the multifactorial nature of fetal distress [ 9 , 10 ], the adverse outcome is not always predictable in risk pregnancies. In addition, many cases of HIE occur unanticipated in low-risk pregnancies.
The aim of this study was to assess the importance of different obstetric risk factors associated with moderate and severe HIE and the need for therapeutic hypothermia in term neonates delivered at the hospitals of Helsinki University Hospital area. We particularly focused on the management protocols of pregnancy and delivery.
This was a retrospective, matched case-control study concerning pregnancies and deliveries in the Helsinki University Hospital area. The same guidelines for follow-up and treatment of pregnancy and delivery are used in all Helsinki University area hospitals. The neonatal intensive care is centralized at the Neonatal Intensive Care Unit (NICU) in Helsinki University Hospital Women’s Clinic. The study period was from January 1, 2013, to December 31, 2017. The treatment of deliveries in the Helsinki University Hospital area was re-organized after a closure of one delivery hospital in late 2017 and the patient record systems was changed in early 2020. Due to the possible bias caused by these factors, years after 2017 were excluded from the study.
The study group consisted of patients who gave birth to asphyxiated singleton neonates with aforementioned symptoms of moderate or severe HIE. Each neonate was born term (one case of 36 6/7 gestation weeks), was admitted to the NICU and offered therapeutic hypothermia for neuroprotection. The indications for hypothermia were admitted from the international guidelines and previous research [ 2 ].
After each delivery with an asphyxiated newborn, the consecutive term singleton, matched by the delivery hospital, fetal gender, presentation (occipital vs. breech), and the mode of delivery (vaginal, assisted vaginal, elective, emergency, and crash cesarean delivery), was selected as a control. An emergency cesarean was defined as a decision-to-delivery-interval of 30 min and a crash cesarean as an immediate delivery after the decision to deliver. Subgroups were formed based on the mode and onset (spontaneous vaginal delivery, induced vaginal delivery, failed induction and cesarean, cesarean) of delivery.
The data for the study was collected from the hospital database (Siemens Obstetrix). All available information concerning fetal and maternal well-being during pregnancy and delivery was collected. This included maternal age and health (pregestational body mass index (BMI), chronic illnesses, medication), gestation at delivery, parity and previous births, and information concerning hospital visits during the ongoing pregnancy. Data on the time of hospital admission and the time of birth in relation to midwife work shifts was also obtained. We considered and tested multiple previously suggested risk factors for HIE or birth asphyxia [ 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 ] and analyzed their possible interactions.
Statistics/analyses
SPSS version 25.0.0 (IBM SPSS Statistics, Armonk, New York) was used to analyze the data. Independent samples t-test and Chi-square test were used for comparing continuous and categorical variables within subgroups, and for testing the independence of variables. Interactions between variables were further assessed with a stratified analysis. ( S10 )
Crude and adjusted odds ratios (OR and aOR respectively) were calculated using logistic regression to estimate associations between different independent variables and the outcome. From the univariate logistic regression, variables with a p < 0.1 were exported to the multivariable logistic regression analysis. A forward stepwise logistic regression analysis was used to suggest multivariable models. Statistical significance was declared at p < 0.05 and the CIs were set to 95%. Due to the novel study design and small sample sizes, we saw fit to try out and present two different approaches to the multivariate logistic regression analysis.
We used Benjamini-Hochberg corrected p -values (q-values) in the univariate logistic regression to account for multiple testing [ 25 ]. Missing values of > 5% per category were imputed using the fully conditional specification method and with maximum iterations of 10.
During the study period, 98 355 deliveries took place in Helsinki University area hospitals, the average being 19 671 per year. One hundred and twelve term neonates (including one case of 36 + 6 gestational weeks) presented with moderate to severe HIE and were admitted to the NICU to receive therapeutic hypothermia. The study period incidence of therapeutic hypothermia for signs of moderate to severe HIE in our obstetric population was 1.0/1000.
After excluding twin pregnancies, ninety-seven singleton pregnancies with neonatal HIE and therapeutic hypothermia made up the primary study group. Due to the failure to find matched controls, nine more pregnancies were excluded, leaving us with the final study group of eighty-eight cases.
Altogether, 45.5% of the neonates (40/88) in the study group were born vaginally and 65% (26/40) of them were ventouse-assisted. Two neonates were vaginally born in breech position. Cesarean deliveries constituted 54.5% (48/88) of study group deliveries, including elective, emergency, and crash procedures with the proportion of 2.0% (1/48), 29.2% (14/48), and 68.8% (33/48) respectively. Four emergency cesarean sections were preceded by a failed instrumental delivery. Due to the matching by delivery mode, the proportions were equal in the control group (Fig. 1 : The mode of delivery among cases of HIE and therapeutic hypothermia). The mortality in the study group was 10.2% (9/88). There were no neonatal deaths in the control group.

The mode of delivery (%) among cases of hypoxic ischemic encephalopathy and therapeutic hypothermia
Approximately the same proportion of patients in the groups were nulliparous (62.5% vs. 59.1%, p = 0.576), and no difference was observed in mean maternal age (31.99 vs. 32.96, p = 0.239) and BMI (24.20 vs. 23.96, p = 0.467). The mean number of daily cigarettes (1.9 vs. 0.4) was higher ( p = 0.001) in the study group. No difference was detected in the mean gestational age at delivery (38.89 vs. 40.21 gestational weeks, p = 0.160) and newborn weight (3458.61 vs. 3472.33 g, p = 0.898). Post term pregnancy was more common (3.41% vs. 13.64%, p = 0.024) in the control group (Table 1 ).
There was no difference in the incidence of the most common antenatal complications, such as hypertension or preeclampsia (10.23% vs. 12.50%, p = 0.797), intrauterine growth restriction (5.68% vs. 7.95%, p = 0.552), gestational (13.64% vs. 15.91, p = 0.671) diabetes, type I diabetes (4.55% vs. 3.41%, p = 0.701) or suspected chorionamniotis (7.95% vs. 6.82%, p = 0.773). There were no cases of diabetes type II in the study group (0% vs. 2.27%, p = 0.497) and cholestasis of pregnancy in the control group (3.41% vs. 0%, p = 0.246) (Table 2 ).
We detected a higher incidence of labour induction in the study group (21.59% vs. 9.09%, p = 0.025), but no difference was detected in the incidence of cesarean after a failed induction (4.55% vs. 11.36%, p = 0.106) or the phase II duration of delivery (35.44 min vs. 46.38 min, p = 0.098). The overall incidence of any obstetric emergency, i.e., shoulder dystocia, placental abruption, or uterine rupture, was higher ( p = 0.038) in the study group (20.45% vs. 10.23%), driven by a markedly higher incidence of shoulder dystocia (6.82% vs. 0%, p = 0.029).
There was no difference in the use of epidural (56.82% vs. 68.18%, p = 0.121), spinal (31.82% vs. 29.55%, p = 0.744) or oral opioid (20.45% vs. 23.86%, p = 0.586) anesthesia of deliveries, whereas the use of oxytocin augmentation (27.27% vs. 57,95%, p < 0.001) and nitrous oxide (38.64% vs. 53.41%, p = 0.050) was more common in the control group.
Midwife shift change during the active phase of delivery (45.45% vs. 60.23%, p = 0.051) was somewhat more frequent in the control group and the incidence of delivery during the night shift insignificantly more common in the study group (48.86% vs. 37.50%, p = 0.070) (Table 2 ).
The univariate analysis showed that nine independent variables were associated ( p < 0.1) with either the presence or absence of moderate to severe HIE: Smoking, post term pregnancy, induction of delivery, duration of phase II, any obstetric emergency, augmentation of delivery by oxytocin (all stages of labour, including induction), use of nitrous oxide, shift change of midwives during active delivery, and delivery during night shift (10 pm. to 8 am.).
In the multivariate regression model with four to eight variables in the same model, obstetric emergencies, labour induction and smoking significantly increased the odds of HIE (Table 3 , Supporting information Tables S1 - S9 ). We were able to repeat these results in most of the tried models. Induction of labour had a significant association with HIE ( p = 0.02) in all tried models, but there was no significant association with HIE and the subgroups of induction methods (balloon catheter, vaginal misoprostol, amniotomy followed by oxytocin-infusion), when entered separately to the regression analysis. In fact, in just 33% of cases only one induction method was used.
In the stratified analysis, the association of induction of labour with HIE was even stronger when oxytocin augmentation was used, OR 9.2 (2.71–31.21). Also, the midwife shift change in induced labours resulted in higher OR for HIE (4.5, 1.73–12.20) (Supporting information, Table S10 ). When adjusted with other variables in logistic regression, the significant association of oxytocin use and HIE was still strong, while shift change, duration of the second phase of delivery, and delivery during night shift lost their statistical significance (Table 3 ).
To reveal any common features in different modes of delivery, results were further analyzed in four subgroups: spontaneous and assisted vaginal delivery, and emergency and crash cesarean (Supporting information, Table S11 ). Mothers without preceding active labour or medical intervention, were omitted from the crash cesarean subgroup.
We also made efforts to deeper analyze the cases of shoulder dystocia and induced labours.
There were six cases of shoulder dystocia in the study group, but none in the control group, which made the regression analysis inapplicable for this specific variable. However, the analyses of all obstetric emergencies (placental abruption, uterine rupture, shoulder dystocia) as a surrogate variable showed a statistically significant association with obstetric emergencies and HIE. The increase in odds of HIE with placental abruption and uterine rupture was insignificant or nonexistent. Aforementioned obstetric emergencies altogether presented an OR of 2.57 and aOR of 3.51 ( p < 0.05) (Table 3 ). Other obstetric emergencies, such as cord prolapse and eclampsia, were not present in our data. The analysis of induced labours showed that even though newborns in the study group were heavier (3790 g vs. 3314 g, p = 0.030), they were more often born vaginally (84.2% vs. 37.5%, p = 0.027) (Supporting information, Table S12 ).
When analyzed by the mode of delivery, induction was more common in the study group in vaginal (OR 2.75, 95% 1.13–6.68, p = 0.016) and assisted (ventouse) vaginal deliveries ( p = 0.017) (Supporting information, Table S11 ). The midwife shift change was more common in the control groups of the emergency ( p = 0.008) and crash ( p = 0.044) caesarean sections and smoking was more common ( p = 0.039) in the study group of the crash cesarean subgroup. Five of the six study group cases with shoulder dystocia occurred in the ventouse delivery subgroup ( p = 0.051) (Supporting information Table S11 ).
In this study, maternal smoking, induction of labour and obstetric emergencies appeared to be independent risk factors for HIE. There was a clear dose-dependent association with maternal smoking and HIE. This finding prevailed in the multivariate analysis, although the increase in odds remained quite small. There were more induced labours in the study group and the association with labour induction was most pronounced in the subgroup that received oxytocin, accounting for the use during and after induction. Also shoulder dystocia, a poorly predictable obstetric emergency, increased the risk for HIE. Other previously stated antecedents, e.g., nulliparity, gestational age, maternal weight [ 22 ], prematurity [ 15 ] and chorionamnionitis [ 6 ] appeared mostly not to associate with HIE in this study. Furthermore, post term pregnancy, nitrous oxide, and the use of oxytocin as an independent variable had a seemingly opposite association with HIE.
Smoking is known to be a major risk factor for birth asphyxia and HIE. It is strongly associated with antecedents for asphyxia, i.e., fetal growth restriction [ 26 ] and the risk of placental abruption [ 6 , 27 , 28 ]. Smoking increases oxidative stress and reduces endogenous defenses in the fetus, which may play a role in the pathogenesis [ 29 ]. Even though the harmful effect of smoking is quite indisputable, some bias in the results has to be recognized. The proportion of missing data was substantial, and the imputed data may have skewed the results towards HIE. Also, the frequency, cessation and continuity of smoking was self-reported and susceptible to social desirability bias. It may be, however, safe to assume that the effect of smoking is at least what is presented by the unimputed data (OR 1.21, 95% CI 0.99–1.46, p = 0.06).
The association between labour induction and HIE requires careful analysis. Significant multicollinearity between induction of labour and other supposed risk factors (obstetric emergency, oxytocin augmentation, shift change, nitrous oxide, and gestational diabetes) was noticed (Supporting information, Table S13 ). The induced labours in the study group ended more frequently in vaginal delivery than in the control group. There were no differences in the indications of labour induction. When these factors are weighed in, the independence of induction of labour as a risk factor for HIE can be considered a complex issue.
The role of induction is, however, worth serious consideration, since these pregnancies may include mothers or fetuses with multiple risk factors. In Finland the rate of induced labours has increased from 17.5% in 2007 to 33.9% in 2021 [ 30 ]. In addition, the proportion of elective inductions without a medical indication are also increasing [ 31 ]. In this study, the risk for HIE was most pronounced among patients with induction of labour together with the use of oxytocin during labour. The oxytocin associated increase in the incidence of encephalopathy was also described in the recent review and meta-analysis by Burgod et al. [ 32 ]. It is also worth noticing that even though newborns in the study group of induced labours were heavier, they were more often born vaginally and the number of ventouse deliveries was twice the proportion in the control group. Compared to zero cases in the study group, in approximately one third of control group cases, a crash cesarean followed a failed ventouse delivery. It can be speculated whether some anchoring bias in decision making is involved and the higher proportions of ventouse and vaginal deliveries in the study group and crash cesareans following ventouse trials in the control group reflect the clinicians’ decisions that are associated with the outcome of the newborn. The number of cases is however too small to draw conclusions.
Shoulder dystocia is an obstetric emergency, that results in prolongation of head-to-body delivery, traction of the brachial plexus, and possible birth trauma [ 33 , 34 ]. The shoulder dystocia incidence reported in studies is approximately 0.7% [ 35 ]. Fetal macrosomia is known to increase the risk of shoulder dystocia more than tenfold [ 35 ] and in these situations, a planned delivery at early term has been demonstrated to reduce the risk of shoulder dystocia [ 34 ]. In this study, six cases of shoulder dystocia were detected in the study group (6.8%) compared to none in the control group. This made the regression analysis inapplicable for this variable. Even though the analysis of all obstetric emergencies (placental abruption, uterine rupture, shoulder dystocia) as a surrogate variable was associated with HIE, the association of HIE with placental abruption and uterine rupture alone was less clear.
As stated, the use of oxytocin in general (irrespective of induction) and nitrous oxide was significantly more common in the control group. However, as shown in the stratified analysis (supplementary information Table S10 ), in the subgroup of induced labours, oxytocin use was more common in the study group. As the need for induction of labour itself may indicate increased risks in the pregnancy, these variables together increase the risk for adverse outcome. In contrast, spontaneous deliveries with oxytocin augmentation were more frequent in the control group. We suggest that the seemingly protective association of oxytocin augmentation in relation to HIE in the regression models could be explained by the asymmetric distribution of these different subgroups. The same can be speculated for the negative association of the administration of nitrous oxide.
The higher incidence of post-term pregnancies in the control group also needs additional attention. It can be speculated that the need for interventions in control group pregnancies was lower and post term was reached more often. It is also of note, that there was significant collinearity between post term pregnancy and oxytocin administration, midwife shift change and delivery during night shift.
In our study population, 54.5% of patients had a cesarean section and the incidences of emergency and crash cesarean were 15.9% and 37.5%. This describes the underlying existence of ante- and intrapartum complications in the study cohort, since the overall incidences of cesarean sections in the Finnish population were 16.7%, 9.2% and 0.9%, respectively [ 30 ]. For example, the rates of pre-eclampsia and pregnancy-induced hypertension in the study were 10.2% and 12.5% compared to our national and worldwide incidences of 5% and 7% [ 36 ].
The purpose of this study was to find HIE risk factors that could be anticipated and avoided in the antenatal care and treatment of delivery. For some patients in the study group, the active labour surveillance, and early obstetric interventions, were never at hand. Our efforts in prevention of HIE should be targeted to patients, that during labour are under constant care and observation.
Compared to previous studies, the selection criteria for this study group were different. Although a similar approach with therapeutic hypothermia as surrogate outcome for severe birth asphyxia (and sequential HIE) has been used before [ 19 ], most case-control studies rest on a study group of neonates diagnosed with neonatal asphyxia, or with signs of birth asphyxia (low Apgar score and/or signs of acidemia in the peripartum blood samples) [ 16 , 18 , 20 , 21 , 24 , 27 , 37 ]. In this study, we chose to use the application of therapeutic hypothermia as the study group inclusion criteria, since it is a clearly defined clinical intervention and in our clinic the indications for use are standardized. The incidence of our inclusion criteria, therapeutic hypothermia (1.1/1000), is slightly higher than the incidence of moderate and severe HIE (0.67/1000) in the study by Liljeström et al. [ 22 ]. Although moderate and severe HIE are the main indications for therapeutic hypothermia, the direct comparison of these incidences should be done with caution. Since the exact severity of HIE may still be uncertain immediately after birth (which may have occurred in another hospital) and the decision concerning this undeniably beneficial treatment has to be made within six hours, the incidence of therapeutic hypothermia treatment may be somewhat higher than the exact incidence of diagnosed moderate and severe HIE.
The study setting could be considered a strength of this study. To the best of our knowledge, this was the first case-control study pairing the groups by the mode of delivery, sex, hospital, and fetal presentation at birth. This could partially explain the differences in our results compared to previous similar studies.
The limitations of this study were its retrospective nature and small sample sizes. It is also likely that the matched case control setting together with a small number of cases failed to show the risks associated with previously described risk factors like hypertension, diabetes, and intrauterine growth restriction. These limitations, as well as coincidence, may also explain the higher incidence of post term pregnancies in the control group. The multicollinearity of some studied risk factors also set limitations when interpreting the data.
There were also some restrictions regarding obtaining data. We didn’t have access to primary health care and antenatal outpatient data, and we relied on the history information of the maternity card and database information upon mothers’ admission to the hospital. Chronic illnesses, obstetric complications and infections were not always structurally recorded. Some information such as substance abuse may be underrepresented but unlikely affects our results.
Demographic risk factors, such as social and marital status, are not collected and had to be excluded. Some previously identified risk factors (urinary tract and viral infections) [ 17 , 23 , 38 , 39 ] had to be excluded because they are treated at the primary health care level.
After controlling for multiple testing, only two of the univariate logistic regression results (maternal smoking and use of oxytocin) remained statistically significant. When studying rare outcomes in limited sample size, one must be careful not to reject the null hypothesis too readily, while minding possibly important findings that fail to reach nominal statistical significance. We considered both these pitfalls and considered clinical applicability as best we could while interpreting these results, but conclusions based on the findings should still be done with caution.
According to our results, induction of labor may be an independent risk factor for HIE, and it should only be used in situations where it evidently improves the outcome of labour. Special vigilance is required from the obstetric team when deciding upon induction and when managing these patients during labour. The increased risk of HIE associated with smoking and obstetric emergencies is unfortunately mostly out of the clinician’s reach.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- Hypoxic-ischemic encephalopathy
Neonatal Intensive Care Unit
Lawn JE, Cousens S, Zupan J. 4 Million neonatal deaths: When? Where? Why? Vol. 365, Lancet.2005;365(9462):891–900.
Jacobs SE, Berg M, Hunt R, Tarnow-Mordi WO, Inder TE, Davis PG. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2013;2013(1):CD003311.
PubMed PubMed Central Google Scholar
Yli BM, Kjellmer I. Pathophysiology of foetal oxygenation and cell damage during labour. Best Pract Res Clin Obstet Gynaecol. 2016;30:9–21.
Article PubMed Google Scholar
Igboanugo S, Chen A, Mielke JG. Maternal risk factors for birth asphyxia in low-resource communities. A systematic review of the literature. J Obstet Gynaecol. 2020;40(8):1039–55.
Rossi AC, Prefumo F. Antepartum and intrapartum risk factors for neonatal hypoxic-ischemic encephalopathy: a systematic review with meta-analysis. Curr Opin Obstet Gynecol. 2019;31(6):410–17.
Sarnat HB, Sarnat MS. Neonatal Encephalopathy following fetal distress: a clinical and electroencephalographic study. Arch Neurol. 1976;33(10):696–705.
Article CAS PubMed Google Scholar
Morales P, Bustamante D, Espina-Marchant P, Neira-Peña T, Gutiérrez-Hernández MA, Allende-Castro C et al. Pathophysiology of perinatal asphyxia: can we predict and improve individual outcomes? EPMA J;2(2). p. 211–30.
Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353(15):1574–84.
Westgate JA, Gunn AJ, Gunn TR. Antecedents of neonatal encephalopathy with fetal acidaemia at term. Br J Obstet Gynaecol. 1999;106(8):774–82.
Seikku L, Gissler M, Andersson S, Rahkonen P, Stefanovic V, Tikkanen M, et al. Asphyxia, neurologic morbidity, and perinatal mortality in early- term and postterm birth. Pediatrics. 2016;137(6):e20153334.
Locatelli A, Incerti M, Paterlini G, Doria V, Consonni S, Provero C, et al. Antepartum and intrapartum risk factors for neonatal encephalopathy at term. Am J Perinatol. 2010;27(8):649–54.
Torres-Muñoz J, Rojas C, Mendoza-Urbano D, Marín-Cuero D, Orobio S, Echandía C. Risk factors associated with the development of perinatal asphyxia in neonates at the Hospital Universitario del Valle, Cali, Colombia, 2010–2011. Biomedica. 2017 1;37(0):51–6.
Lundgren C, Brudin L, Wanby AS, Blomberg M. Ante- and intrapartum risk factors for neonatal hypoxic ischemic encephalopathy. J Matern Fetal Neonatal Med. 2018;18(12):1595–601.
Article Google Scholar
Itoo BA, Al-Hawsawi ZM, Khan AH. Hypoxic ischemic encephalopathy. Incidence and risk factors in North Western Saudi Arabia. Neurosciences. 2003;8(2):113–9.
PubMed Google Scholar
Ayuk Widiani NN, Yuli Kurniati DP, Trisna Windiani IGA. Maternal and infant risk factors on the incidence of neonatal asphyxia in Bali: Case Control Study. Public Health Prev Med Arch. 2016;4(2):120–6.
Hall DR, Smith M, Smith J. Maternal factors contributing to asphyxia neonatorum. J Trop Pediatr. 1996;42(4):192–5.
Badawi N, Kurinczuk JJ, Keogh JM, Alessandri LM, O’Sullivan F, Burton PR, et al. Intrapartum risk factors for newborn encephalopathy: the western Australian case-control study. Br Med J. 1998;317(7172):1549–53.
Article CAS Google Scholar
Blume HK, Loch CM, Li CI. Neonatal encephalopathy and socioeconomic status: Population-based case-control study. Arch Pediatr Adolesc Med. 2007;161(7):663–8.
Nelson DB, Lucke AM, Mcintire DD, Sánchez PJ, Leveno KJ, Chalak LF. Obstetric antecedents to body cooling treatment of the Newborn Infant. Am J Obs Gynecol. 2014;211(2):155–6.
Nayeri F, Shariat M, Dalili H, Bani Adam L, Zareh Mehrjerdi F, Shakeri A. Perinatal risk factors for neonatal asphyxia in Vali-e-Asr hospital, Tehran-Iran. Iran J Reprod Med. 2012;10(2):137–40.
Heinonen S, Saarikoski S. Reproductive risk factors of fetal asphyxia at delivery: a population based analysis. J Clin Epidemiol. 2001;54(4):407–10.
Liljestrom L, Wikstrom AK, Agren J, Jonsson M. Antepartum risk factors for moderate to severe neonatal hypoxic ischemic encephalopathy: a Swedish national cohort study. Acta Obstet Gynecol Scand. 2018;97(5):615–23.
Martinez-Biarge M, Madero R, Gonzlez A, Quero J, Garca-Alix A. Perinatal morbidity and risk of hypoxic-ischemic encephalopathy associated with intrapartum sentinel events. Am J Obstet Gynecol. 2012;206(2):148.e1-148.e7.
Ellis M, Manandhar N, Manandhar DS, De L, Costello AM. Risk factors for neonatal encephalopathy in Kathmandu, Nepal, a developing country: unmatched case-control study. Br Med J. 2000;320(7244):1229–36.
Benjamini Y, Hochberg Y. Controlling the false Discovery rate: a practical and powerful Approach to multiple testing. J R Stat Soc Ser B. 1995;57(1):289–300.
Abraham M, Alramadhan S, Iniguez C, Duijts L, Jaddoe VWV, Den Dekker HT, et al. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE Public Libr Sci. 2017;12(2):e0170946.
Tikkanen M, Surcel HM, Bloigu A, Nuutila M, Ylikorkala O, Hiilesmaa V, et al. Self-reported smoking habits and serum cotinine levels in women with placental abruption. Acta Obstet Gynecol Scand. 2010;89(12):1538–44.
Downes KL, Shenassa ED, Grantz KL. Neonatal outcomes Associated with placental abruption. Am J Epidemiol. 2017;186(12):1319–28.
Article PubMed PubMed Central Google Scholar
Gitto E, Reiter RJ, Karbownik M, Tan D-x, Gitto P, Berberi S, et al. Causes of oxidative stress in the pre- and Perinatal Period. Neonatology. 2002;81(3):146–57.
Perinataalitilasto. – synnyttäjät, synnytykset ja vastasyntyneet - THL [Internet]. [cited 2020 Aug 6]. https://thl.fi/fi/tilastot-ja-data/tilastot-aiheittain/seksuaali-ja-lisaantymisterveys/synnyttajat-synnytykset-ja-vastasyntyneet/perinataalitilasto-synnyttajat-synnytykset-ja-vastasyntyneet .
Kruit H, Nuutila M, Rahkonen L. Lääkärilehti - Synnytyksen käynnistäminen, Kun raskaus on täysiaikainen. Lääkärilehti. 2016;71(25–32/2016):1845–51.
Google Scholar
Burgod C, Pant S, Morales MM, Montaldo P, Ivain P, Elangovan R, et al. Effect of intra-partum oxytocin on neonatal encephalopathy: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):1–7.
Collins KA, Popek E. Birth Injury: Birth Asphyxia and Birth Trauma. Academic Forensic Pathology. Volume 8. SAGE Publications Inc.; 2018. pp. 788–864.
Farrar D, Simmonds M, Bryant M, Sheldon TA, Tuffnel D, Golder S, et al. Treatments for gestational diabetes: a systematic review and meta-analysis. BMJ Open. 2017;7(6):e015557.
Hartiadystokia. - Duodecim Oppiportti [Internet]. [cited 2020 Aug 18]. https://www-oppiportti-fi.libproxy.helsinki.fi/op/njs15507/do?p_haku=hartiadystokia#q=hartiadystokia .
Rana S, Lemoine E, Granger J, Karumanchi SA, Preeclampsia. Pathophysiology, challenges, and perspectives. Circ Res. 2019;124(7):1094–112.
Milsom I, Ladfors L, Thiringer K, Niklasson A, Odeback A, Thornberg E. Influence of maternal, obstetric and fetal risk factors on the prevalence of birth asphyxia at term in a Swedish urban population. Acta Obstet Gynecol Scand. 2002;81(10):909–17.
Hayes BC, McGarvey C, Mulvany S, Kennedy J, Geary MP, Mattherws TG et al. A case-control study of hypoxic-ischemic encephalopathy in newborn infants at > 36 weeks gestation. Am J Obstet Gynecol. 2013;209(1):29.e1-29.e19.
Kapaya H, Williams R, Elton G, Anumba D. Can obstetric risk factors predict fetal acidaemia at Birth? A retrospective case-control study. J Pregnancy. 2018;2018:2195965.
Download references
Acknowledgements
We gratefully acknowledge the assistance of Paula Bergman, biostatistician at Biostatistics consulting, University of Helsinki, Finland, for her biostatistical advice.
Helsinki University State Research Funding.
Open Access funding provided by University of Helsinki (including Helsinki University Central Hospital).
Author information
Authors and affiliations.
Department of obstetrics and gynecology, Helsinki University Women’s Hospital, Haartmaninkatu 2, Helsinki, 00029, Finland
Suoma Roto, Ilkka Kalliala & Marja Kaijomaa
Children’s Hospital, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
Irmeli Nupponen
You can also search for this author in PubMed Google Scholar
Contributions
SR contributed to the literature search, figures, study design, data collection, data analysis, data interpretation and writing. IN contributed to the study design, data collection data interpretation and writing. IK contributed to the data interpretation and writing. MK contributed to the study design, data collection, data analysis, data interpretation, figures, and writing.
Corresponding author
Correspondence to Marja Kaijomaa .
Ethics declarations
Ethical approval.
The study was approved by the Helsinki University Hospital Institutional Review Board. (March 3, 2018, 1/2018).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Roto, S., Nupponen, I., Kalliala, I. et al. Risk factors for neonatal hypoxic ischemic encephalopathy and therapeutic hypothermia: a matched case-control study. BMC Pregnancy Childbirth 24 , 421 (2024). https://doi.org/10.1186/s12884-024-06596-8
Download citation
Received : 31 May 2023
Accepted : 20 May 2024
Published : 12 June 2024
DOI : https://doi.org/10.1186/s12884-024-06596-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Birth asphyxia
- Induction of labour
- Oxytocin treatment
- Shoulder dystocia
- Therapeutic hypothermia
BMC Pregnancy and Childbirth
ISSN: 1471-2393
- Submission enquiries: [email protected]
- General enquiries: [email protected]
- Open access
- Published: 19 June 2024
The impact of temperature, humidity and closing school on the mumps epidemic: a case study in the mainland of China
- Xiaoqun Li 1 na1 ,
- Lianyun Zhang 1 na1 ,
- Changlei Tan 2 ,
- Ziheng Zhang 4 ,
- Juan Ding 5 &
- Yong Li 1
BMC Public Health volume 24 , Article number: 1632 ( 2024 ) Cite this article
30 Accesses
Metrics details
To control resurging infectious diseases like mumps, it is necessary to resort to effective control and preventive measures. These measures include increasing vaccine coverage, providing the community with advice on how to reduce exposure, and closing schools. To justify such intervention, it is important to understand how well each of these measures helps to limit transmission.
In this paper, we propose a simple SEILR (susceptible-exposed-symptomatically infectious-asymptomatically infectious-recovered) model by using a novel transmission rate function to incorporate temperature, humidity, and closing school factors. This new transmission rate function allows us to verify the impact of each factor either separately or combined. Using reported mumps cases from 2004 to 2018 in the mainland of China, we perform data fitting and parameter estimation to evaluate the basic reproduction number \({\mathfrak R}_0\) . As a wide range of one-dose measles, mumps, and rubella (MMR) vaccine programs in China started only in 2008, we use different vaccination proportions for the first Stage I period (from 2004 to 2008) and the second Stage II period (from 2009 to 2018). This allows us to verify the importance of higher vaccine coverage with a possible second dose of MMR vaccine.
We find that the basic reproduction number \({\mathfrak R}_0\) is generally between 1 and 3. We then use the Akaike Information Criteria to assess the extent to which each of the three factors contributed to the spread of mumps. The findings suggest that the impact of all three factors is substantial, with temperature having the most significant impact, followed by school opening and closing, and finally humidity.
We conclude that the strategy of increasing vaccine coverage, changing micro-climate (temperature and humidity), and closing schools can greatly reduce mumps transmission.
Peer Review reports
Mumps is an acute infection caused by the mumps virus (MuV). Mumps virus, parainfluenza, measles, respiratory syncytial virus and so on belong to paramyxoviruses, which are an RNA-type [ 1 , 2 ]. The virus diameter is 85–300 nm, with an average of 140 nm [ 3 , 4 ]. Mumps is a highly infectious disease, with more than 300,000 young people in China infected each year. Mumps can cause severe complications such as orchitis, oophoritis, pancreatitis, encephalitis, meningitis, and deafness [ 5 , 6 , 7 , 8 , 9 ]. Its primary route of early transmission is the virus carried by sneezing and coughing droplets of patients, inhaled, and deposited in the respiratory tract [ 3 , 10 ]. Most patients are children and teenagers aged 2 and 24 with intense contact [ 5 , 11 , 12 , 13 ]. The incubation period for mumps is about 15 to 24 days, of which 19 days is a median [ 3 , 14 , 15 ]. The most common strategy to prevent infection is mumps vaccination, which is usually part of a combination vaccine for measles, rubella, and mumps (MMR) [ 16 , 17 ]. Many developed countries have adopted two doses of the mumps in their national immunization schedules. Though vaccinated people may still be infected with mumps, their risk for mumps has been reduced by about 78% for people who received one dose of MMR vaccine and about 88% for people who received two doses of MMR vaccine [ 9 , 18 , 19 ]. China started to introduce a dose of MMR vaccine to 18-month-old children in our free health insurance program in 2008 which has significantly reduced the mumps cases [ 2 , 20 ].
Studies have found that the number of infectious diseases in the population changes periodically, and the incidence shows seasonal patterns [ 21 , 22 , 23 , 24 , 25 ], such as measles, chickenpox, rabies, influenza, etc. Like these infectious diseases, mumps cases showed strong seasonal patterns. Ukraine had more mumps cases in winter and spring [ 26 ]. Jordan also reported more mumps cases in winter and spring [ 27 ]. Mumps was found to have a significant peak in April in the United States [ 25 ]. In China, a significant peak was in April-July with another small peak in November and December [ 28 , 29 ].
To have a better understanding of the spread and control of infectious diseases like mumps, mathematical models are commonly used to assess the impact of different factors including vaccine and population heterogeneity on the transmission of mumps. Qu et al. proposed a SVEILHR ( S : susceptible, V : vaccinated, E : exposed, I : mild infectious, L : severe infectious, H : hospitalized, R : recovered) model with a seasonal varying transmission rate to simulate the seasonal outbreak of mumps, they found that improving vaccine coverage played an essential role in curbing the epidemics and recommended two doses of MMR vaccine in China [ 17 ]. Li et al. obtained the same finding from their SVEILR ( S : susceptible, V : vaccinated, E : exposed, I : severely infectious, L : mildly infectious, R : recovered) model [ 16 ]. Nurbek et al. studied the effects of population heterogeneity and vaccine failure on mumps spread. They found that vaccine failure, changes in seasonality, and age structure were all associated with the mumps recurrence in Jiangsu Province [ 18 ]. Liu et al. also investigated the effects of population heterogeneity by constructing a multi-group SVEIAR ( S : susceptible, V : vaccinated, E : exposed, I : symptomatically infected, A : asymptomatically infected, R : recovered) [ 30 ].
Rather than using a compartment model, a few researchers have used statistical regression models to analyze the association of temperature and humidity with the seasonal patterns of mumps [ 2 , 7 , 15 , 28 ], where both temperature and humidity were considered independent factors. Hu et al. used a distributed hysteresis nonlinear model (DLNM) to evaluate the relationship between meteorological factors and the incidence of mumps in Fujian Province. They concluded that the lowest temperature and the highest relative humidity levels may increase mumps risk [ 2 ]. Yang et al. used the Poisson regression model combined with DLNM to evaluate the correlation of mumps incidence in Guangzhou, China, from 2005 to 2012 and concluded that the incidence of mumps increased with the increase of mean temperature and relative humidity [ 15 ]. Li et al. used the generalized additive model to quantify the relationship between meteorological factors and mumps in Jining, Shandong Province and concluded that the relationship between temperature and the incidence of mumps was J-shaped, with 4℃ corresponding to the minimum risk [ 28 ]. Ho et al. investigated the relationship between meteorological factors and the incidence of mumps in Taiwan, China, by using Poisson regression analysis and case-crossover and found that there was an inverted V-shaped relationship between the number of mumps cases and temperature. That is, the incidence of mumps began to rise when the temperature was 20℃ and began to decline again when the temperature was higher than about 25℃ [ 7 ].
In this paper, we propose a simple SEILR model by using a novel transmission rate function to incorporate temperature, humidity, and closing school. To our knowledge, this is the first paper to analyze the impact of all three factors together using a compartment dynamic model. There is a detailed description of our model in " Model building " section. He et al. used an SIR model to assess the seasonal patterns of the spread of influenza A in Canada [ 23 ] with a similar transmission rate \(\beta\left(t\right)\) including temperature, humidity, and closing school factors.
The purpose of this study is to analyze the factors affecting mumps (temperature, humidity, and school opening and closing) based on a dynamic model and verify the applicability of the model by fitting the monthly case numbers of 31 districts, including 22 provinces, 5 autonomous regions, and 4 municipalities directly in the mainland of China (excluding Hong Kong, Macao, Taiwan) from 2004 to 2018, and finally calculate the basic reproduction number of each province, and then give some reliable measures. The structure of this article is as follows. In " Problem-driven and data-driven mumps model " section, we first introduce the area studied in this paper and the data sources needed for the research. Then, we establish the SEILR model and give the basic formula for calculating the basic reproduction number of this model. In " Methods " section, we focus on the methods used in this study, including data fitting methods, criteria for model selection, and methods for parameter sensitivity analysis. In " Results " section, we compare the \({\mathfrak R}_0\) in the three temperature zones, analyze the provinces with higher \({\mathfrak R}_0\) , select the most appropriate model through the Akaike Information Criterion ( AIC ), explore the effects of temperature, humidity, and school opening and closing on the spread of mumps, interpret the parameters of the model, and analyze the sensitivities of the model parameters through the partial rank correlation coefficients (PRCC). In " Discussion " section, we recommend some preventive measures for controlling mumps epidemics, and conclude with a brief summary.
Problem-driven and data-driven mumps model
China (73°33′ ∼ 135°05′E, 3°51′ ∼ 53°33′N), with a land area of about 9.6 million square kilometers and a marine land area of about 4.73 million square kilometers [ 31 ], according to the results of China’s seventh population census, has about 1.443 billion people [ 32 ]. Its terrain and climate changes dramatically from the west to the east, as mumps cases are available only from the mainland of China, this study here excludes Hong Kong, Macao, and Taiwan.
The Mainland of China has 31 districts, including 22 provinces, 5 autonomous regions, and 4 municipalities directly under the Central Government, based on their geographical location and climate [ 33 ], we group 31 districts into the following 3 temperate zones, see Fig. 1 .

Three temperature zones of the mainland of China. ((I) Subtropical: Hainan, Guangdong, Guangxi, Yunnan, Jiangxi, Hunan, Chongqing, Guizhou, Fujian, Zhejiang, Hubei, Jiangsu, Sichuan, Anhui, Shanghai (Hainan is actually tropical, but because there is only one Hainan in the tropics, Hainan is classified as subtropical here for the convenience of discussion); (II) Temperate: Shandong, Beijing, Tianjin, Shanxi, Hebei, Henan, Shaanxi, Gansu, Xinjiang, Ningxia, Jilin, Heilongjiang, Liaoning, and Inner Mongolia; (III) The vertical temperature zone: Tibet and Qinghai.)
Data sources
The study uses monthly mumps case data in the mainland of China during the 2004–2018 period. It is from the Public Health Science Data Center [ 4 ]. The monthly average temperature and humidity data is from the Chinese Bureau of Statistics [ 34 ]. Although each school semester’s opening and closing dates varied province by province, city by city, in general, the first semester of each year starts in September, and the winter vacation started in the middle of January of the following year. The second semester began in mid-February, and the summer vacation starts in July [ 35 ]. Here, schools include kindergarten, primary schools, middle schools, high schools, and universities to cover most mumps patients who were aged 2 to 24 years old in China.
Model building
To make the model more effective, we make the following assumptions:
Assume that the populations we study are homogeneous, thus ignoring differences in gender, physical condition, etc., in each age group in each district.
According to relevant studies, mumps patients are predominantly adolescents, so our susceptible people only consider the proportion of the population aged 0–24 years. In this part, we obtain the annual population data of each district through the annual China Statistical Yearbook [ 34 ] and obtain the proportion of the population aged 0–24 years to obtain the relevant data of susceptible people ( S ) and the relevant data of overt patients ( I ) are obtained from Chinese Health Organizations.
Since the measles, rubella, and mumps vaccines are the same MMR vaccines, here we ignore the impact of other diseases and only consider mumps.
Our model is a simple SEILR (susceptible-exposed-symptomatically infectious- asymptomatically infectious-recovered). We divided the total population into five compartments: susceptible S , exposed E , symptomatic patients I , asymptomatic patients L , and recovered R . Total population N = S + E + I + L + R . A population size of \(\Lambda\) enters the system, and the mortality rate of each compartment is specified as \(\mu\) . For the population of susceptible people ( S ), there are two ways of flow: one is death, and the other is the exposed ( E ) population with a transmission rate \(\beta\left(t\right)\) . There are two types of susceptible people ( S ): one is the vaccinated population, assuming its proportion is \(q\) ; the other is the non-vaccinated population, then its proportion is (1 -q ), the infection capacity of vaccinated people is lower than that of non-vaccinated people, so we use \(\gamma\) to represent the reduced ability of vaccinated individuals to become infected. There are two ways of flow for the exposed population ( \(E\) ): the first is to become a symptomatic patient ( \(I\) ), the second is to become an asymptomatic patient ( \(L\) ); we use \(\alpha\) to present the rate of progression to infectious ( \(I\) ) per month. For this portion of the population, we use \(p\) to represent the proportion of symptomatic patients ( \(I\) ). For symptomatic patients ( \(I\) ), their primary flow is recovery ( \(R\) ), where we use \(\delta\) to represent the rate of symptomatic ( \(I\) ) to recovered patients ( \(R\) ) per month. There are two main flows of asymptomatic infected persons ( \(L\) ), where we denote by \(\eta\) the rate of not symptomatic infected persons ( \(L\) ) to symptomatic infected persons ( \(I\) ), then ( \(1 - \eta\) ) persons flow to recovered persons ( \(R\) ), and we denote by \(\sigma\) the rate of not symptomatic ( \(L\) ) to symptomatic ( \(I\) ) or recovered ( \(R\) ). The flowchart of this dynamics is shown in Fig. 2 .

Flowchart of mumps transmission in a population
According to Fig. 2 , we establish a system of ordinary differential equations to model the spread of mumps:
As a wide range of one-dose free MMR vaccine programs in China started only in 2008 [ 2 ], we divide the study period into two stages to use different vaccination rates for each stage. Stage I: January 2004 to December 2008 has not yet been introduced. Stage II: January 2009 to December 2018. Vaccination rate \(q\) is defined as follows:
The transmission rate \(\beta \left( t \right)\) plays an essential role in the spread of mumps epidemics. As mumps outbreak shows strong seasonal patterns by following a school calendar, a number of researchers have used a simple sinusoidal function \(\beta \left( t \right)\) = \(\beta \left( 0 \right)\) + \(\sin \left( {\omega t + \phi } \right)\) for the seasonal varying transmission rate [ 17 , 18 ]. Rather than using a compartment model, a few researchers have used statistical regression models to analyze the association of temperature and humidity with the seasonal patterns of mumps [ 2 , 15 , 24 , 28 ], where both temperature and humidity were considered independent factors.
Unlike previous studies, in this article, we will concretize \(\beta \left( t \right)\) and consider the specific influencing factors on \(\beta \left( t \right)\) . To investigate the impact of temperature, humidity, and school opening and closing on the seasonal patterns of mumps cases in the mainland of China, we choose \(\beta \left( t \right) = {\beta_0}{f_1}{f_2}{f_3}\) . Where \({f_1}\) is a function of temperature, \({f_2}\) is a function of humidity, and \({f_3}\) is a function of school opening and closing.
Now, we discuss how to choose functions \(f_1,\;f_2\) and \(f_3\) :
1) Temperature function \(f_1\) : Mumps is a seasonal infectious disease [ 25 , 36 , 37 ], and it is greatly affected by temperature. Relevant studies show that the number of cases of mumps will increase with the increase in temperature, and when it increases to a certain height, it will decrease with the increase in temperature. It becomes an inverted V-shape [ 7 , 15 ]. So we introduce \({c_T}\) parameters as the optimal temperature, take the normal distribution function as the temperature function in this model.
2) Humidity function \(f_2\) : As humidity and temperature are strongly correlated to each other, Lin et al. showed that the number of mumps cases began to increase at a relative humidity of 65% to 69%. Several studies have also used exponential functions to explore the relationship between humidity and influenza transmission [ 24 , 38 , 39 ], so in this paper, we also assume to use an exponential function as the humidity function \(f_2\) , with humidity as the independent variable.
3) School vacation function \(f_3\) : In school vacations, students have less contact with other people, so its transmission rate should be smaller than the rate in school days [ 24 ]. Our data also show that the mumps cases decreased after school vacations started. Therefore, we use \(\varepsilon\) as a reduction factor for the transmission of mumps during school winter vacation, and \(\theta\) as a reduction factor for the transmission of mumps during school summer vacation. Now our school vacation function:
This completes the construct of time varying \(\beta \left( t \right)\) with seasonal patterns. Table 1 summarizes all parameters in our model.
Calculation of basic reproduction number
As total population \(N = S + E + I + L + R\) , summarizing the left-hand side and right-hand side of the model (1) separately yields
The biologically feasible region of model (1) is
which can be verified as positively invariant (i.e., given non-negative initial values in \(\Omega\) , all solutions to model (1) have non-negative components and stay in \(\Omega\) for \(t \geqslant 0\) ) and globally attractive in \({\mathbb{R}}_+^5\) concerning model (1). Therefore, we restrict our attention to the dynamics of model (1).
It is easy to see that model (1) always has a disease-free equilibrium \({P_0}\) ,
By using the next-generation matrix and the concept of basic reproduction number [ 40 , 41 ], we have the basic reproduction number, for details, see Appendix A.
where \({T_0}\) is the total time.
- Data fitting
In this section, we first use model (1) to simulate the reported mumps data of most districts in the mainland of China, predict the disease trend, and obtain the influence of temperature, humidity, and school opening and closing on mumps. Data on mumps cases mainly come from the China Public Health Science Data Center [ 4 ]. We then must estimate the other 17 parameters and 5 initial values (See " Analysis of parameters " section for detailed ranges of parameters):
By calculating the minimum sum of the Chi-square error [ 42 , 43 , 44 ]:
Where \(n\) represents the total number of months of simulation time in each province, \(I\left( {t_i} \right)\) , \(i = 1,2,3, \cdots ,n\) represents the true number of cases per month. \(\mathop {I({t_i}}\limits^\sim )\) , \(i = 1,2,3, \cdots ,n\) represents the fitted value of monthly cases. MATLAB tool Particle swarm function [ 45 , 46 , 47 ] is used to solve the multidimensional unconstrained linear optimization problem, and the minimum value of the multivariable unconstrained function \(H\left( \varpi \right)\) is found by the derivative-free method to determine the optimal parameter value \(\varpi\) . The data fitting for each district is shown in Supplementary Information.
Selection criteria for epidemiological models
In epidemiological modeling studies, there are usually criteria to explore the plausibility of the models. Among them, the Akaike Information Criterion ( \(AIC\) ) and Bayesian Information Criterion ( \(BIC\) ) are the two most commonly used methods to measure the goodness-of-fit and complexity of statistical models [ 48 , 49 ]. Although \(AIC\) and \(BIC\) are tools for choosing between different models, the results of the two criteria for the same model may differ due to their trade-offs and the degree of penalty for complexity. \(BIC\) penalizes model complexity more strictly and is sensitive to sample size, so it is generally used to select simple models with fewer parameters. \(AIC\) punishes model complexity more leniently and is not particularly sensitive to sample size. That is, it can tolerate the complexity of the model to a certain extent, so it is generally used in situations where the sample is relatively large. Our model has a large sample size and is more suitable for \(AIC\) [ 50 ]. This criterion measures the relative goodness-of-fit of a mathematical model, penalizes overfitting, encourages the selection of models that fit well with the data, and compares the strengths and weaknesses of multiple competing models. However, if you want the number of parameters of the fitted mathematical model to include a more significant penalty, you need to use the \(AIC\) version by modification, also known as \(AICc\) [ 51 , 52 , 53 ]. At the same time, since \(AIC\) and \(AICc\) are of an arbitrary scale and difficult to explain, it can also be obtained that different competing models have relative support in the same data by calculating the value of \({\Delta_j}\) [ 52 ]. Another helpful way to measure a model’s support for data is the Akaike weight \({\omega_i}\) [ 52 ]. Based on these information criteria, a model is given:
Where \(n\) represents the number of data points in the dataset, \(k\) represents the number of fitted parameters plus one, and \(SSE\) is the least squares error. \(AI{C_j}\) is the \(AIC\) of the \(jth\) model, and \(AI{C_{\min }}\) is the optimal \(AIC\) model. \({\Delta_j}\) represents the difference between the \(AIC\) value of \({\text{mode}}{{\text{l}}_j}\) and the \(AIC\) value of the optimal model. \({\omega_i}\) represents the weight of \({\text{mode}}{{\text{l}}_i}\) , measuring the relative contribution of each model to data interpretation. When the \(SSE\) is smaller and the \(AIC\) is smaller, the better the \(AICc\) model fits. The smaller \({\Delta_j}\) , the closer the surface \({\text{mode}}{{\text{l}}_j}\) is to the optimal model on the fitted data. The criteria for \({\Delta_j}\) are shown in Table 2 . For the Akaike weight \({\omega_i}\) , if the Akaike weight \({\omega_i}\) of the fitted model is more significant than other models, the model is relatively supported in the data.
Partial rank correlation coefficients
Sensitivity analysis (SA) is a method to identify and quantify the effect of parameter uncertainty on the basic reproduction number \({\Re_0}\) . The model’s predictability is improved by controlling the critical parameters identified that significantly impact the model output. Here, we assume that each parameter is a random variable with a uniform distribution and analyze the model’s sensitivity through the uncertainty of Latin hypercube sampling. At present, this method has been applied to many epidemiological models [ 54 , 55 ].
We first use Latin hypercube sampling to sample the parameters that appear in the basic reproduction number \({\Re_0}\) , and then calculate the partial rank correlation coefficients (PRCC) based on the LHS matrix to analyze the sensitivity of the parameters to \({\Re_0}\) and the model to determine the extent and way these parameters affect \({\Re_0}\) . Therefore, to examine the sensitivity of \({\Re_0}\) when the parameter changes, we use Latin hypercube sampling to examine the dependence of the parameters on \({\Re_0}\) .
Data fitting and model selection
To explore the degree of influence of temperature, humidity, and closing school from a mechanical perspective, we have taken into account the following sub-models: ( \({U_1}\) ) All three factors of temperature, humidity, and closing school are taken into account ( \(\beta \left( t \right) = {\beta_0}{f_1}{f_2}{f_3}\) ). ( \({U_2}\) ) The temperature factor is removed ( \({f_1} = 1\) ). ( \({U_3}\) ) The humidity factor is removed ( \({f_2} = 1\) ). ( \({U_4}\) ) The school opening and closing factor is removed ( \({f_3} = 1\) ). Here, we only select the reported cases in Jiangsu Province for discussion, and the discussion in other provinces is similar, and a plot of the effects of \({f_1}\) , \({f_2}\) , and \({f_3}\) can be seen in Fig. 3 .

Temperature function \({f_1}\left( t \right)\) , the relative humidity function \({f_2}\left( t \right)\) , the school opening and closing function \({f_3}\left( t \right)\) , and the transmission rate function \(\beta \left( t \right)\) in the model \({U_1}\)
We want to select the model from four groups of models ( \({U_1}\) ) -( \({U_4}\) ) that best describe the fitting effect of the data based on the method of judging the strength of the model (The fit of the four sets of models can be seen in Fig. 4 ).

The fitting effects of four models ( \({U_1}\) - \({U_4}\) )
Based on the Akaike Information Criterion ( \(AIC\) ), Table 3 shows that \(SSE\) , \(AIC\) , and \(AICc\) of model \({U_1}\) are the smallest in \({U_1} - {U_4}\) , and \({\Delta_1} < 2\) , that is to say, when all three factors are considered, the data support for the model is the highest, \({U_3}\) has relatively little support, while \({U_2}\) and \({U_4}\) are essentially unsupported relative to each other. At the same time, \({\omega_1} > {\omega_3} > {\omega_4} > {\omega_2}\) , it can also be seen that the impact of these three factors on the degree of mumps from large to small in the order of temperature, school opening and closing, and humidity.
Analysis of parameters
We analyze the parameters of the model \({U_1}\) , some of which have been estimated by WHO, some of which have been evaluated by mumps researchers and predecessors, and others which remain uncertain. The following parameters are analyzed in detail (The data for these parameters can be detailed in Table 4 ).
1) The natural mortality rate \(\mu\) is numerically equal to the inverse of life expectancy at birth. The average age from 2004 to 2018 is 76.63 [ 34 ], i.e., \(\mu\) = 1/(76.63 \(\times\) 12), therefore \(\mu\) = 0.0011.
2) The rate of monthly conversion from exposed ( \(E\) ) to the patient ( \(I\) and \(L\) ) \(\alpha\) : the incubation period of mumps is usually 15–24 days [ 14 , 15 ], we studied monthly data, and the reciprocal of \(\alpha\) indicates the incubation period, so we assume \(\alpha\;\in\;\lbrack1.25,\;2\rbrack\) , according to parameter estimation \(\alpha = 1.3063\) , the incubation period of mumps is \({\raise0.7ex\hbox{${30}$} \!\mathord{\left/ {\vphantom {{30} \alpha }}\right.\kern-0pt}\!\lower0.7ex\hbox{$\alpha $}} = 23\) days.
3) The proportion of monthly conversion from exposed patients ( \(E\) ) to symptomatic patients ( \(I\) ) \(p\) : we set \(p\in\left[0,1\right]\) , according to parameter estimation \(p = 0.0563\) , about \(5.63\%\) of exposed patients will turn into symptomatic patients every month, and about. \(1 - p = 94.37\%\) of exposed patients will turn into asymptomatic patients every month.
4) Rate of symptomatic ( \(I\) ) to recovered patients ( \(R\) ) per month \(\delta\) : symptomatic patients usually recover in about 10 days, considering that we study monthly case data from 31 districts in the mainland of China for a total of 180 months from 2004–2018, which involves a large range of recovery time of 7–30 days, so we set \(\delta\in\lbrack1,\ {\raise0.7ex\hbox{${30}$} \!\mathord{\left/ {\vphantom {{30} 7}}\right.\kern-0pt}\!\lower0.7ex\hbox{$7$}}]\) .
5) Rate of progression from asymptomatic patients ( \(L\) ) to symptomatic patients ( \(I\) ) or recovered patients ( \(R\) ) \(\sigma\) : similar to \(\delta\) , we also set \(\sigma\;\in\;\lbrack1,30/7\rbrack\) , according to the parameter estimate \(\sigma = 2.1093\) , the asymptomatic patients ( \(L\) ) will become symptomatic patients ( \(I\) ) or recovered patients ( \(R\) ) after about \({\raise0.7ex\hbox{${30}$} \!\mathord{\left/ {\vphantom {{30} \sigma }}\right.\kern-0pt}\!\lower0.7ex\hbox{$\sigma $}} = 14\) days [ 56 ].
6) The proportion of asymptomatic patients ( \(L\) ) transformed into symptomatic patients ( \(I\) ) \(\eta\) : most asymptomatic patients with mumps will recover [ 56 ], thus, we set \(\eta \in [0,0.5]\) . According to the parameter estimation \(\eta = 0.2575\) , it can be seen that about \(25.75\%\) of asymptomatic patients are transformed into patients every month, and \(1 - 25.75\% = 74.25\%\) of asymptomatic patients will recover.
7) Vaccine coverage rate \(q\) , we make the following subsections: 2004–2008 vaccine is not free, the vaccination situation in this period is not clear, so we set \(q_1\;\in\;\lbrack0.01,1\rbrack\) , 2009–2018 this period China will be the mumps vaccine into the relevant health insurance plan [ 2 , 20 ], according to China’s relevant school enrollment policy [ 57 ], school children must be vaccinated against relevant vaccines, including the mumps vaccine, through China’s population data we find that the age of the population of 0–12 years old is at least 20% [ 34 ], so we set \(q_2\in\lbrack0.2,1\rbrack\) . According to the parameter estimation, \({q_1} = 0.1935\) and \({q_2} = 0.8395\) , it can be concluded that after the popularization of MMR vaccine in China in 2008, the vaccination rate has significantly increased, and the vaccination rate also has a specific effect on the prevention and control of mumps.
8) \(\gamma\) and \(\rho\) denote the infection reduction factor and propagation reduction factor respectively. Cases that can be diagnosed and categorized by laboratory pathology are unknown, so we set \(\gamma , \rho \in [0,1]\) .
Parameter sensitivity analysis
We set the sample volume to \(n = 2000\) and take the parameters in the analog as an input variable and the value of \({\Re_0}\) as an output variable. The PRCC on the 10 parameters is shown in Fig. 5 . Among them, the effect of parameters on the result is mainly reflected in the absolute value of PRCC values for \({\Re_0}\) can be seen on Table 5 . The greater the absolute value of the PRCC of the parameter, the more significant its impact on the change of \({\Re_0}\) , and the positive or negative influence is positive or negative. In our experiments, we assume that the parameters of the p-value less than or equal to 0.01 have a significant impact, at the same time, focus on analyzing the parameters of the absolute value of its PRCC > 0.2. We can easily see that different parameters affect \({\Re_0}\) . Among them, \(\beta , \eta , \gamma , \rho\) significantly actively affect \({\Re_0}\) , while \(\delta , \sigma\) , and \({q_1}\) significantly negatively affect \({\Re_0}\) . Figure 5 shows that the contact rate \(\beta\) (PRCC = 0.6727) has the most significant effect on \({\Re_0}\) , then followed by the rate of not symptomatic to symptomatic or recovered per month \(\sigma\) (PRCC = -0.6349) and by the rate of symptomatic to recovered patients per month \(\delta\) (PRCC = -0.5430). Meanwhile, Fig. 6 shows that we also analyze PRCC of every parameter over continuous time. In " Discussion " section, we will analyze the parameters that have a more significant impact by the sensitivity analysis and propose some measures to cope with mumps.

Show the PRCC of parameters with \({\Re_0}\)

PRCC of parameters in continuous time
Comparative analysis of \({\Re_0}\)
The respective temperature and humidity of Zone I-III are shown in Table 6 . And the basic reproduction number \({\Re_0}\) for the 31 districts in the mainland of China is shown in Fig. 7 . It is found fitting that \({\Re_0}\) of subtropical has roughly distributed around 1–3. It should be noted that \({\Re_0}\) in Guizhou Province is relatively high, and its value is 4.2413. Zhang et al. proposed in the relationship between meteorological factors and mumps based on the Boosted regression tree model that with the increase of temperature, the occurrence of mumps shows an upward trend, and 4℃ corresponds to the minimum risk [ 5 ]. Hence, the lower the temperature below 4℃, the greater the \({\Re_0}\) ; the higher the temperature above 4℃, the more likely the \({\Re_0}\) is to be larger. While the lowest temperature in Guizhou Province is -1.5℃, the maximum temperature is 24.3℃, and the average temperature is 14.67℃, we consider that \({\Re_0}\) in Guizhou Province is affected by temperature. Yang et al. proposed that the relationship between meteorological factors and mumps incidence in Guangzhou from 2005 to 2012 that the higher the relative humidity [ 15 ], the greater \({\Re_0}\) of mumps, while the lowest relative humidity in Guizhou Province is 0.65, the highest relative humidity is 0.92, the average relative humidity is 0.79. It can be found that the relative humidity in Guizhou is still relatively high. We consider that \({\Re_0}\) of Guizhou is greatly affected by relative humidity. Therefore, \({\Re_0}\) in Guizhou may be related to the low temperature, humidity, and vaccination rate in Guizhou. \({\Re_0}\) in temperate regions is also roughly around 1–3, and it should also be noted that the basic reproduction number \({\Re_0}\) in Gansu Province is slightly larger, is 4.0485. Check the data to discover the particularity of the natural environment of Gansu Province. Gansu Province has a subtropical monsoon climate, temperate monsoon climate, temperate continental (arid) climate, plateau alpine climate, and four other major climate types. Hamami et al., in studying weakened immunity and mumps outbreaks, concluded that the weakening of human immunity is the main factor in the outbreak of various epidemics [ 58 ], so here we consider that mumps in Gansu Province is not only related to temperature, humidity, school holidays, etc. but may also be related to its complex climate type and low vaccination rate. \({\Re_0}\) is about 3 in the vertical temperature zone, which is relatively consistent.

The value of \({\Re_0}\) for each province in the mainland of China
Through calculations, we found that the average \({\Re_0}\) in the subtropical region is 1.7126, which is relatively the smallest; the average \({\Re_0}\) in the temperate region is 2.1429, which is in the middle position; the average value of \({\Re_0}\) in the vertical temperature zone of the Qinghai-Tibet Plateau is 3.4252, which is relatively the largest. Considering its relationship with temperature, we guess that the mumps virus activity may be more potent at low temperature, which is also the problem we will explore later. For threshold systems, if \({\Re_0}\) < 1, mumps can be eliminated, and the disease can be controlled. If \({\Re_0}\) > 1, the condition will remain at the epidemic level, and specific isolation measures need to be taken to control the spread of mumps effectively. In the Netherlands, Wales, and England, \({\Re_0}\) of mumps was about 11–14 from 1960 to 1980, \({\Re_0}\) by the state in the United States is roughly distributed in 4–7 [ 59 ]. However, \({\Re_0}\) of mumps in China is relatively small [ 59 ]. By consulting the relevant literature, \({\Re_0}\) of mumps in China in recent years is estimated to be about 6.5428 [ 17 ]. Li et al. estimated the prevalence of mumps in the mainland of China at 4.28 [ 16 ], and Nurbek et al. estimated the prevalence of mumps in Jiangsu Province from 2005 to 2019 at 1–2 [ 18 ]. There may be some variation in the results of \({\Re_0}\) in each country and region due to the influencing factors studied in the selected case data. \({\Re_0}\) of mumps in the mainland of China learned here was estimated to be 4.5933. It can be seen that mumps has been better controlled than before. However, the \({\Re_0}\) > 1 here indicates that mumps is still at the epidemic level, so isolation, prevention, and control still need to be strengthened.
The findings in this study show that vaccination is still one of the most effective strategies to prevent mumps epidemics, as \({\Re_0}\) (Stage I) > \({\Re_0}\) (Stage II). For most provinces and cities in China, only one dose of free MMR vaccine is available, while the most developed countries have implemented two doses of MMR vaccine program. The American Academy of Pediatrics recommends that children receive the first dose of the MMR vaccine at 12 to 15 months of age and the second dose is at 4 to 6 years of age [ 6 ]. Since the 1980s, most European countries have routinely immunized children against mumps [ 60 ]. Therefore, China should maintain the current one dose of MMR vaccine program and encourage more children to receive a second dose. We fit the data for each of the 31 districts and calculate \({\Re_0}\) , and find that \({\Re_0}\) for most districts are concentrated in 1–3. We also get the basic reproduction number for the three temperature zones and find that the \({\Re_0}\) of the Qinghai-Tibet Plateau > middle temperate zone \({\Re_0}\) > subtropical zone \({\Re_0}\) , which clearly shows that the temperature and humidity have an impact on the spread of mumps.
We use Akaike Information Criteria to evaluate the four models \({U_1}\) - \({U_4}\) and find that temperature has the most significant effect on mumps, followed by closing school, and humidity has the lowest impact on mumps epidemics.
Our results show that mumps is a resurging disease. The three parameters \(\beta , \delta\) , and \(\sigma\) have the greatest influence on \({\Re_0}\) . We can reduce \({\Re_0}\) by decreasing \(\beta\) and increasing \(\delta\) and \(\sigma\) so that we can prevent mumps. \(\beta \left( t \right)\) is related to temperature, humidity, and the closing school. We suggest that in the early stage of mumps outbreaks, it can be prevented by increasing vaccination, personal hygiene, and closing schools; at the peak of mumps outbreaks, attention should be paid to the effects of temperature and humidity on mumps; when the temperature is too high, we can help cool it down by sprinkler watering and planting greenery; when the humidity is too high, attention should be paid to the opening of windows to ventilate the room and air conditioning and dehumidifiers can be used to lower the humidity; in the peak of mumps outbreaks, attention should also be given to the contact among students, and certain isolation measures should be taken if necessary; and when the peak is over, disinfection should be paid attention to, and attention should be paid to personal protection. \(\delta\) denotes the rate of symptomatic patients to recovery and \(\sigma\) denotes the recovery rate of asymptomatic patients in this paper, an effective measure to increase \(\delta\) and \(\sigma\) is to strengthen the immune system, which can be achieved through vaccination and physical exercise. So we recommend strengthening the second dose of mumps vaccination, and more importantly, educating raising awareness of the preparedness to deal with mumps, and if necessary, isolation measures to deal with mumps [ 61 ].
Our findings show that mumps is still a disease of great impact in China. More importantly, mumps control measures should be intensified in the high-risk areas of the vertical temperature zone including the Qinghai-Tibet Plateau, especially, in the school term periods. Apart from increasing vaccination coverage, we only study the impact of three factors of temperature, humidity, and closing schools on the mumps in the mainland of China, other factors like social economics, public health resources, and population heterogeneity may also have a social economic impact on mumps outbreaks, we will investigate these factors in future.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
Mumps virus
Measles-Mumps-Rubella
Distributed Lag Nonlinear Model
Latin hypercube sampling
Akaike Information Criterion
Akaike Information Criterion corrected
Bayesian Information Criterion
Sum of Squared Errors
Sensitivity analysis
Partial Rank Correlation Coefficient
World Health Organization
Arithmetic Mean
Standard Deviation
Rubin S, Eckhaus M, Rennick LJ, Bamford CG, Duprex WP. Molecular biology, pathogenesis and pathology of mumps virus. J Pathol. 2015;235(2):242–52.
Article CAS PubMed PubMed Central Google Scholar
Hu W, Li Y, Han W, Xue L, Zhang W, Ma W, Bi P. Meteorological factors and the incidence of mumps in Fujian Province, China, 2005–2013: Non-linear effects. Sci Total Environ. 2018;619:1286–98.
Article PubMed Google Scholar
Hviid A, Rubin S, Mühlemann K. Mumps. The Lancet. 2008;371(9616):932–44.
Article Google Scholar
Public Health Science Data Center, Mumps, https://www.phsciencedata.cn/Share/ky_sjml.jsp?id=6e476dc3-1575-4d53-90c9-4982c99c0444 , Accessed 18 Aug 2023 (2023).
Zhang D, Guo Y, Rutherford S, Qi C, Wang X, Wang P, Zheng Z, Xu Q, Li X. The relationship between meteorological factors and mumps based on Boosted regression tree model. Sci Total Environ. 2019;695:133758.
Article CAS PubMed Google Scholar
Centers for Disease Control and Prevention, Mumps, https://www.cdc.gov/mumps/vaccination.html , Accessed 17 Sep 2021 (2021).
Ho Y-C, Su B-H, Su H-J, Chang H-L, Lin C-Y, Chen H, Chen K-T. The association between the incidence of mumps and meteorological parameters in Taiwan. Hum Vaccin Immunother. 2015;11(6):1406–12.
Article PubMed PubMed Central Google Scholar
Galazka AM, Robertson SE, Kraigher A. Mumps and mumps vaccine: a global review. Bull World Health Organ. 1999;77(1):3.
CAS PubMed PubMed Central Google Scholar
Watson-Creed G, Saunders A, Scott J, Lowe L, Pettipas J, Hatchette TF. Two successive outbreaks of mumps in Nova Scotia among vaccinated adolescents and young adults. Can Med Assoc J. 2006;175(5):483–8.
Johnson CD, Goodpasture EW, et al. The Etiology of Mumps, American. J Hygiene. 1935;21:46–57.
Google Scholar
Whyte D, O’Dea F, Mcdonnell C, O’Connell N, Callinan S, Brosnan E, Powell J, Monahan R, FitzGerald R, Mannix M, Greally T, Dee A, O’Sullivan P. Mumps epidemiology in the mid-west of Ireland 2004–2008: increasing disease burden in the university/college setting. Euro Surveill. 2009;14(16):19182.
Park SH. Resurgence of mumps in Korea. Infection and Chemotherapy. 2015;47(1):1–11.
Association for the Study of Infectious Disease. A retrospective survey of the complications of mumps. J R Coll Gen Pract. 1974;24(145):552–6.
Richardson M, Elliman D, Maguire H, Simpson J, Nicoll A. Evidence base of incubation periods, periods of infectiousness and exclusion policies for the control of communicable diseases in schools and preschools. Pediatr Infect Dis J. 2001;20(4):380–91.
Yang Q, Yang Z, Ding H, Zhang X, Dong Z, Hu W, Liu X, Wang M, Hu G, Fu C. The relationship between meteorological factors and mumps incidence in Guangzhou, China, 2005–2012: a distributed lag nonlinear time-series analysis. Hum Vaccin Immunother. 2014;10(8):2421–32.
Li Y, Liu X, Wang L. Modelling the transmission dynamics and control of mumps in mainland China. Int J Environ Res Public Health. 2018;15(1):33.
Qu Q, Fang C, Zhang L, Jia W, Weng J, Li Y. A mumps model with seasonality in China. Infect Dis Model. 2017;2(1):1–11.
Azimaqin N, Peng Z, Ren X, Wei Y, Liu X. Vaccine failure, seasonality and demographic changes associate with mumps outbreaks in Jiangsu Province, China: Age-structured mathematical modelling study. J Theor Biol. 2022;544:111125.
Latner DR, Hickman CJ. Remembering mumps. PLoS Pathog. 2015;11(5):e1004791.
Chinese Center for Disease Control and Prevention, Mumps, https://www.chinacdc.cn/nip/kpyd/bdxcrb/lxxsy/ Accessed 8 March 2021 (2021).
London WP, Yorke JA. Recurrent outbreaks of measles, chickenpox and mumps: I. Seasonal variation in contact rates, American Journal of Epidemiology. 1973;98(6):453–68.
Zhang J, Jin Z, Sun GQ, Sun XD, Ruan S. Modeling seasonal rabies epidemics in China. Bull Math Biol. 2012;74(5):1226–51.
He D, Dushoff J, Eftimie R, Earn DJ. Patterns of spread of influenza A in Canada. Proceedings of the Royal Society B: Biological Sciences. 2013;280(1770):20131174.
Article PubMed Central Google Scholar
He D, Dushoff J, Day T, Ma J, Earn DJ. Inferring the causes of the three waves of the 1918 influenza pandemic in England and Wales. Proceedings of the Royal Society B: Biological Sciences. 2013;280(1766):20131345.
Shah AP, Smolensky MH, Burau KD, Cech IM, Lai D. Seasonality of primarily childhood and young adult infectious diseases in the United States. Chronobiol Int. 2006;23(5):1065–82.
Hrynash Y, Nadraga A, Dasho M. Effectiveness of a vaccination program against mumps in Ukraine. Eur J Clin Microbiol Infect Dis. 2008;27(12):1171–6.
Batayneh N, Bdour S. Mumps: immune status of adults and epidemiology as a necessary background for choice of vaccination strategy in Jordan. APMIS. 2002;110(7–8):528–34.
Li R, Lin H, Liang Y, Zhang T, Luo C, Jiang Z, Xu Q, Xue F, Liu Y, Li X. The short-term association between meteorological factors and mumps in Jining. China, Science of the Total Environment. 2016;568(15):1069–75.
Cui A, Zhu Z, Chen M, Zheng H, Liu L, Wang Y, Ma Y, Wang C, Fang X, Li P, Epidemiologic and genetic characteristics of mumps viruses isolated in China from, et al. to 2010. Infect Genet Evol. 1995;21(2014):384–90.
Liu Z, Hu J, Wang L. Modelling and analysis of global resurgence of mumps: A multi-group epidemic model with asymptomatic infection, general vaccinated and exposed distributions. Nonlinear Anal Real World Appl. 2017;37:137–61.
The Central People’s Government of the People’s Republic of China, China’s national conditions, https://www.gov.cn/guoqing/index.htm Accessed 20 Aug 2023 (2023).
The Central People’s Government of the People’s Republic of China, Bulletin of the Seventh National Population Census, https://www.gov.cn/guoqing/2021-05/13/content_5606149.htm Accessed 13 May 2021 (2021).
The Central People’s Government of the People’s Republic of China, Air temperature and temperature band, https://www.gov.cn/test/2005-06/24/content_9217.htm Accessed 20 Aug 2023 (2023).
National Bureau of Statistics 2018, China Statistical Yearbook, http://www.stats.gov.cn/sj/ndsj/2018/indexch.htm Accessed 2018 (2018).
People’s Government of Anshun City, Notice of the Office of the Provincial Department of Education on the Schedule of the School Calendar for Primary and Secondary Schools (Kindergartens) in the Province for the Academic Year 2023–2024, http://www.anshun.gov.cn/zwgk/zdlyxx/jyxx1/jcjy/202305/t20230525_79896162.html?isMobile=false Accessed 2023 (2023).
Anderson LJ, Seward JF. Mumps epidemiology and immunity: the anatomy of a modern epidemic. Pediatr Infect Dis J. 2008;27(10):S75–9.
Onozuka D, Hashizume M. Effect of weather variability on the incidence of mumps in children: a time-series analysis. Epidemiol Infect. 2011;139(11):1692–700.
Earn DJ, He D, Loeb MB, Fonseca K, Lee BE, Dushoff J. Effects of school closure on incidence of pandemic influenza in Alberta. Canada, Annals of Internal Medicine. 2012;156(3):173–81.
Shaman J, Kohn M. Absolute humidity modulates influenza survival, transmission, and seasonality. Proc Natl Acad Sci. 2009;106(9):3243–8.
Diekmann O, Heesterbeek JAP, Metz JA. On the definition and the computation of the basic reproduction ratio in models for infectious diseases in heterogeneous populations. J Math Biol. 1990;28:365–82.
Van den Driessche P, Watmough J. Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease transmission. Math Biosci. 2002;180(1–2):29–48.
Zhang X, Zhao Y, Neumann AU. Partial immunity and vaccination for influenza. J Comput Biol. 2010;17(12):1689–96.
Li Y, Wang L-W, Peng Z-H, Shen H-B. Basic reproduction number and predicted trends of coronavirus disease 2019 epidemic in the mainland of China. Infect Dis Poverty. 2020;9(1):1–13.
Li Y, Liu X, Yuan Y, Li J, Wang L. Global analysis of tuberculosis dynamical model and optimal control strategies based on case data in the United States. Appl Math Comput. 2022;422: 126983.
Sierra MR, Coello Coello A. Improving PSO-based multi-objective optimization using crowding, mutation and dominance. In: International Conference on Evolutionary Multi-Criterion Optimization. Springer; 2006. p. 505–19.
Marini F, Walczak B. Particle swarm optimization (PSO). A tutorial, Chemometrics and Intelligent Laboratory Systems. 2015;149:153–65.
Article CAS Google Scholar
Huang C-L, Dun J-F. A distributed PSO–SVM hybrid system with feature selection and parameter optimization. Appl Soft Comput. 2008;8(4):1381–91.
M. Martcheva, An introduction to mathematical epidemiology, Vol. 61, Springer, 2015.
Tan C, Li S, Li Y, Peng Z. Dynamic modeling and data fitting of climatic and environmental factors and people’s behavior factors on hand, foot, and mouth disease (HFMD) in Shanghai, China. Heliyon. 2023;9(8).
Hirotugu Akaike, Information Theory and an Extension of the Maximum Likelihood Principle, https://api.semanticscholar.org/CorpusID:64903870 , 1973.
Hurvich CM, Tsai C-L. Regression and time series model selection in small samples. Biometrika. 1989;76(2):297–307.
Burnham K.P, Anderson D.R. Model Selection and Multimodel Inference A Practical Information-Theoretic Approach (Second Edition). Springer-Verlag; 1998.
Miao H, Dykes C, Demeter LM, Wu H. Differential equation modeling of HIV viral fitness experiments: model identification, model selection, and multimodel inference. Biometrics. 2009;65(1):292–300.
Wu Y, Huang M, Wang X, Li Y, Jiang L, Yuan Y. The prevention and control of tuberculosis: an analysis based on a tuberculosis dynamic model derived from the cases of Americans. BMC Public Health. 2020;20(1):1–16.
Lou P, Wang L, Zhang X, Xu J, Wang K, et al. Modelling seasonal brucellosis epidemics in Bayingolin Mongol autonomous prefecture of Xinjiang, China, 2010–2014. BioMed Res Int. 2016;2016:5103718.
Brenda L. Tesini, Mumps, https://www.msdmanuals.cn/home/children-s-health-issues/common-viral-infections-in-infants-and-children/mumps Accessed July 2021 (2021).
The Central People’s Government of the People’s Republic of China, Circular on the issuance of methods for the verification of vaccination certificates for children enrolled in nurseries and schools, https://www.gov.cn/zhengce/zhengceku/2021-02/09/content_5586296.htm Accessed 21 Jan 2021 (2021).
Hamami D, Cameron R, Pollock KG, Shankland C. Waning immunity is associated with periodic large outbreaks of mumps: a mathematical modeling study of Scottish data. Front Physiol. 2017;8:233.
Anderson RM, May RM. Infectious diseases of humans: dynamics and control. Oxford university press; 1991.
Book Google Scholar
European Centre for Disease Prevention and Control, Mumps, https://www.ecdc.europa.eu/en/mumps Accessed 21 Jan 2021 (2020).
Cardemil CV, Dahl RM, James L, Wannemuehler K, Gary HE, Shah M, Marin M, Riley J, Feikin DR, Patel M, et al. Effectiveness of a third dose of MMR vaccine for mumps outbreak control. N Engl J Med. 2017;377(10):947–56.
Download references
Acknowledgements
We would like to thank anonymous reviewers for constructive suggestions, which significantly improved this manuscript.
The work was partially supported by the National Natural Science Foundation of China (Nos. 11901059; 12326335), Undergraduate Training Program of Yangtze University for Innovation and Entrepreneurship (No. Yz2021286) and the Natural Science Foundation of Hubei Province, China (No. 2021CFB601).
Author information
Xiaoqun Li and Lianyun Zhang contributed equally to this work.
Authors and Affiliations
School of Information and Mathematics, Yangtze University, Nanhuan Road, Jingzhou, 434023, China
Xiaoqun Li, Lianyun Zhang & Yong Li
Information Engineering College, Hunan Applied Technology University, Shanjuan Road, Changde, 415100, China
Changlei Tan
Department of Operations Research and Information Engineering, Beijing University of Technology, Pingle Garden, Beijing, 100124, China
School of Environment, Education & Development (SEED), The University of Manchester, Oxford Road, M139PL, Manchester, UK
Ziheng Zhang
Jingzhou Hospital Affiliated to Yangtze University, Chuyuan Avenue, Jingzhou, 434023, China
You can also search for this author in PubMed Google Scholar
Contributions
Xiaoqun Li and Lianyun Zhang first gained an understanding of the transmission mechanism of mumps by reviewing relevant information. They then constructed the model, designed and conducted the experiments, collected and organized the data, and performed data analysis. They also wrote the code for data fitting and were responsible for writing and typesetting the paper's content, ultimately completing the initial draft. Changlei Tan and Yan Wu assisted in writing the code to validate its feasibility and provided technical support. Ziheng Zhang was responsible for verifying the authenticity of the fitting results. Juan Ding and Yong Li supervised and directed the planning, design, and execution of the entire project, ensuring the model's feasibility and the accuracy of the results. They also aided in the writing and revision of this paper.
Corresponding authors
Correspondence to Juan Ding or Yong Li .
Ethics declarations
Ethics approval and consent to participate.
Since no individual patient’s data was collected, the ethical approval or individual consent was not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., appendix a: the detailed calculation process of \({\re_0}\).
Following the discussion in Sect. " Calculation of basic reproduction number ", model (1) always has a disease-free equilibrium \({P_0}\) and \({P_0}\) is the solution of the algebraic equations:
We use the next generation matrix to derive basic reproduction number [ 40 , 41 ]. First, we change the order of model (1) by
The Jacobian matrix F and V of \(\mathfrak{F}\) and \(\mathfrak{V}\) at \({P_0}\) are:
the inverse of \(V\) is
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Li, X., Zhang, L., Tan, C. et al. The impact of temperature, humidity and closing school on the mumps epidemic: a case study in the mainland of China. BMC Public Health 24 , 1632 (2024). https://doi.org/10.1186/s12889-024-18819-w
Download citation
Received : 28 November 2023
Accepted : 09 May 2024
Published : 19 June 2024
DOI : https://doi.org/10.1186/s12889-024-18819-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Basic reproduction number
- Temperature
- School opening and closing
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]
- Open access
- Published: 20 June 2024
Circulating small extracellular vesicles in Alzheimer’s disease: a case–control study of neuro-inflammation and synaptic dysfunction
- Rishabh Singh 1 ,
- Sanskriti Rai 1 ,
- Prahalad Singh Bharti 1 ,
- Sadaqa Zehra 1 ,
- Priya Kumari Gorai 2 ,
- Gyan Prakash Modi 3 ,
- Neerja Rani 2 ,
- Kapil Dev 4 ,
- Krishna Kishore Inampudi 1 ,
- Vishnu V. Y. 5 ,
- Prasun Chatterjee 6 ,
- Fredrik Nikolajeff 7 &
- Saroj Kumar 1 , 7
BMC Medicine volume 22 , Article number: 254 ( 2024 ) Cite this article
7 Altmetric
Metrics details
Alzheimer’s disease (AD) is a neurodegenerative disease characterized by Aβ plaques and neurofibrillary tangles. Chronic inflammation and synaptic dysfunction lead to disease progression and cognitive decline. Small extracellular vesicles (sEVs) are implicated in AD progression by facilitating the spread of pathological proteins and inflammatory cytokines. This study investigates synaptic dysfunction and neuroinflammation protein markers in plasma-derived sEVs (PsEVs), their association with Amyloid-β and tau pathologies, and their correlation with AD progression.
A total of 90 [AD = 35, mild cognitive impairment (MCI) = 25, and healthy age-matched controls (AMC) = 30] participants were recruited. PsEVs were isolated using a chemical precipitation method, and their morphology was characterized by transmission electron microscopy. Using nanoparticle tracking analysis, the size and concentration of PsEVs were determined. Antibody-based validation of PsEVs was done using CD63, CD81, TSG101, and L1CAM antibodies. Synaptic dysfunction and neuroinflammation were evaluated with synaptophysin, TNF-α, IL-1β, and GFAP antibodies. AD-specific markers, amyloid-β (1–42), and p-Tau were examined within PsEVs using Western blot and ELISA.
Our findings reveal higher concentrations of PsEVs in AD and MCI compared to AMC ( p < 0.0001). Amyloid-β (1–42) expression within PsEVs is significantly elevated in MCI and AD compared to AMC. We could also differentiate between the amyloid-β (1–42) expression in AD and MCI. Similarly, PsEVs-derived p-Tau exhibited elevated expression in MCI compared with AMC, which is further increased in AD. Synaptophysin exhibited downregulated expression in PsEVs from MCI to AD ( p = 0.047) compared to AMC, whereas IL-1β, TNF-α, and GFAP showed increased expression in MCI and AD compared to AMC. The correlation between the neuropsychological tests and PsEVs-derived proteins (which included markers for synaptic integrity, neuroinflammation, and disease pathology) was also performed in our study. The increased number of PsEVs correlates with disease pathological markers, synaptic dysfunction, and neuroinflammation.
Conclusions
Elevated PsEVs, upregulated amyloid-β (1–42), and p-Tau expression show high diagnostic accuracy in AD. The downregulated synaptophysin expression and upregulated neuroinflammatory markers in AD and MCI patients suggest potential synaptic degeneration and neuroinflammation. These findings support the potential of PsEV-associated biomarkers for AD diagnosis and highlight synaptic dysfunction and neuroinflammation in disease progression.
Peer Review reports
The progressive neurodegenerative condition known as Alzheimer’s disease (AD) is characterized by cognitive decline as a result of the formation of amyloid-β (Aβ) plaques, neurofibrillary tangles (NFTs), and chronic neuroinflammation that leads to neurodegeneration [ 1 , 2 , 3 ]. Synapse loss is a crucial pathophysiological event in disease progression, and synaptic proteins have been extensively studied due to earlier perturbations [ 4 , 5 ]. The pathological hallmark of AD, amyloid-β plaques, originates from the imprecise cleavage of the amyloid precursor protein (APP) by β-secretase (BACE1) and γ-secretase generating amyloid-β peptide forms [ 6 , 7 , 8 , 9 ]. Primary amyloid-β peptide forms are Aβ40 and Aβ42, where the majority of the amyloid-β plaques in AD brains are composed of Aβ42 [ 10 ]. Many point mutations in APP and γ-secretase cause familial early-onset AD, favoring Aβ42 formation, causing amyloid-β peptides prone to aggregate as fibrils and plaques [ 9 , 11 , 12 , 13 , 14 ]. Hyperphosphorylation of tau causes the formation of NFTs. The combined effect of accumulation of NFTs, amyloid-β fibrils, and plaques leads to neuronal function loss and cell death [ 15 , 16 ]. Aβ plaques activate immune receptors on microglia, thereby releasing pro-inflammatory cytokines and chemokines that mediate neuroinflammation, which, if it reaches a chronic level, causes damage to brain cells, including axonal demyelination and synaptic pruning [ 17 , 18 , 19 , 20 , 21 , 22 , 23 ]. In addition to these, other proteins, including the neurofilament light (NFL) protein, glial fibrillary acidic protein (GFAP), and synaptic proteins, have also been identified as AD biomarkers [ 24 , 25 , 26 , 27 , 28 ]. Understanding the intricate dynamics of AD in terms of its varied pathophysiological manifestations, such as neuroinflammation, synaptic loss, and proteinopathy, is essential for developing potential therapeutic interventions for AD and biomarker discovery. In clinical practice, cognitive assessment tools such as the Addenbrooke’s Cognitive Examination (ACE-III) and Mini-Mental State Examination (MMSE) are used to diagnose AD. These tools evaluate verbal fluency and temporal orientation, although results may be influenced by subject bias [ 29 , 30 , 31 ].
In recent years, small extracellular vesicles (sEVs) or exosomes have been acknowledged as crucial mediators of communication and signaling within the body, contributing significantly to the transmission of cellular cargo in various health and disease states. They also play a notable role in disseminating protein aggregates associated with neurodegenerative diseases [ 32 ]. sEVs are bi-layered membrane vesicles that have a heterogeneous group of (< 200 nm in diameter) that are found in different human body fluids, including blood, urine, saliva, and ascites, and that are actively released by all cell types [ 33 , 34 , 35 ]. For their functions in various physiological and pathological circumstances, sEVs are the most extensively researched type of EV [ 36 , 37 , 38 ]. sEVs exchange information between cells by transferring bioactive components (nucleic acids and proteins) [ 39 ]. As the sEVs’ composition bears the molecular signature of the secreting cell and bears an intrinsic property of transversing the blood–brain barrier (BBB) in both directions [ 40 , 41 ], they are a target of constant research in neurodegenerative disease. Furthermore, sEVs released by neuronal cells are crucial in transmitting signals to other nerve cells, influencing central nervous system (CNS) development, synaptic activity regulation, and nerve injury regeneration. Moreover, sEVs exhibit a dual function in neurodegenerative processes, as sEVs not only play an essential role in clearing misfolded proteins, thereby exerting detoxifying effects and providing neuroprotection [ 42 ]. On the other hand, they also have the potential to participate in the propagation and aggregation of misfolded proteins, particularly implicated in the pathological spread of Tau aggregates as indicated by both in vitro and in vivo studies [ 43 ]. As a protective mechanism, astrocytes (most abundant glial cells) accumulate at the locations where Aβ peptides are deposited, internalizing and breaking down aggregated peptides [ 44 ]. However, severe endosomal–lysosomal abnormalities arise in astrocytes when a significantly large amount of Aβ accumulates within astrocytes for a prolonged period without degradation [ 45 , 46 ]. Astrocytes then release engulfed amyloid-β (1-42) protofibrils through exosomes, leading to severe neurotoxicity to neighboring neurons [ 44 ]. Additionally, it has been found that the release of amyloid-β by microglia in association with large extracellular vesicles (Aβ-lEVs) damages synaptic plasticity and modifies the architecture of the dendritic spine [ 47 ]. Thus, sEVs can be a compelling subject for the investigation to understand AD’s inflammation and synaptic dysfunction [ 48 , 49 , 50 , 51 , 52 ].
In this study, we reported that protein levels are associated with AD pathology, neuroinflammation, and synaptic dysfunction in plasma-derived small extracellular vesicles (PsEVs). Our objective was to understand the pathophysiological process, neuroinflammation, synaptic dysfunction, and Aβ pathology through sEVs. Our study revealed a significant correlation between the concentration of cargo proteins derived from PsEVs and clinical diagnosis concerning ACE-III and MMSE scores. Furthermore, the levels of these studied proteins within PsEVs could differentiate between patients with MCI and AD. Thus, our study sheds light on the potential of PsEVs in understanding AD dynamics and offers insights into the underlying mechanisms of disease progression.
Subject recruitment
A total of n = 35 AD patients and n = 25 subjects with MCI were recruited from the Memory Clinic, Department of Geriatrics, All India Institute of Medical Sciences, New Delhi, India. Additionally, n = 30 healthy AMC (volunteers) were recruited. The inclusion criteria were as follows: a clinical diagnosis of MCI and AD patients using ACE-III and MMSE tests. The exclusion criteria encompass medical conditions such as cancer, autoimmune disorders, liver disease, hematological disorders, or stroke, as well as psychiatric conditions, substance abuse, or any impediment to participation. Controls were healthy, age-matched adults without neurological symptoms. AMC was 60–71, MCI was 65–79, and AD was 70–80 years of age range (Table 1 ). Neuropsychological scores, viz., ACE-III and MMSE, were recorded before subject selection.
Study ethical approval
The institutional ethics committee of All India Institute of Medical Sciences, New Delhi, India, granted the study ethical permission. The study has been granted the ethical approval number IECPG-670/25.08.2022. Following the acquisition of the written informed consent, all participants were enrolled.
Sample collection
One milliliter of blood was drawn from each participant using venipuncture, and blood collection vials were kept on ice during collection. The blood was centrifuged at 1700 g for 20 min at 4 °C to remove the cells, and the straw-colored plasma was collected. It was further clarified by centrifuging for 30 mi at 4 °C at 10,000 g. Finally, cleared plasma was stored at − 80 °C until further use. The samples were used for the downstream experiment after being thawed on ice and centrifuged at 10,000 g.
Isolation of PsEVs
The PsEVs were extracted by chemical-based precipitation from the plasma samples of AD patients, MCI patients, and AMC, as discussed previously [ 53 , 54 ]. In brief, 180 μL of plasma sample was used and filtered with 0.22 μm filter (SFNY25R, Axiva), followed by overnight incubation with the chemical precipitant (14% polyethylene glycol 6000) (807,491, Sigma). The samples underwent an hour-long, 13,000 g centrifugation at 4 °C the next day. Before being resuspended in 200 μL of 1X PBS (ML116-500ML, HiMedia), the pellet was first cleaned twice with 1X PBS. Before downstream experiments, the sEVs-enriched fraction was further filtered through a 100-kDa filter (UFC5100, Millipore).
Nanoparticle tracking analysis (NTA)
5000-fold dilution in 1X-PBS buffer was used for the NTA of PsEVs. In the ZetaView Twin system (Particle Metrix, Germany) sample chamber, 1 mL of diluted PsEVs sample was introduced. The following parameters were used throughout three cycles of scanning 11 cell locations each, and 60 frames per position were collected (video setting: high, focus: autofocus, shutter: 150, 488 nm internal laser, camera sensitivity: 80, cell temperature: 25 °C. CMOS cameras were used for recording, and the built-in ZetaView Software 8.05.12 (Particle Metrix, Germany) was used to analyze: 10 nm as minimum particle size, 1000 nm as maximum particle size, and 30 minimum particle brightness.
Transmission electron microscopy for morphological characterization
Transmission electron microscopy was employed to investigate PsEVs’ ultrastructural morphology. The resultant PsEVs pellet was diluted with PBS using 0.1 M phosphate buffer (pH 7.4). A carbon-coated copper grid of 300 mesh (01843, Ted Pella) was used to adsorb the separated PsEVs at room temperature for 30 min. After blot-drying, the adsorbed grids were dyed. For 10 s, 2% aqueous uranyl acetate solution (81,405, SRL Chem) as negative staining. After blotting the grids, they were inspected using a Talos S transmission electron microscope (ThermoScientific, USA).
Western blot
Based on the initial volume of biofluid input, all samples were normalized, i.e., 180 μL and the sample loading dye (2 × Laemmle Sample buffer) was mixed with PsEVs sample, and 20 μL equal volume was loaded to run on an 8–12% SDS PAGE [ 53 , 55 ]. After the completion of SDS-PAGE, protein from the gel was subjected to the Wet transfer onto the PVDF membrane of 0.22 μm (1,620,177, BioRad). The membrane-blocking with 3% bovine serum albumin (BSA) (D0024, BioBasic) in Tris (TB0194, BioBasic) base saline containing 0.1% of Tween 20 (65,296, SRL Chem) (TBST) using the BioRad Western blotting apparatus (BioRad, USA). Following this, overnight incubation of primary antibodies of CD63 (10628D, Invitrogen), CD81 (PA5-86,534, Invitrogen), TSG101 (MA1-23,296, Invitrogen), L1CAM (MA1-46,045, Invitrogen), synaptophysin (ADI-VAM-SV011-D, Enzo life sciences), GFAP (A19058, Abclonal), amyloid-β (1–42) oligomer (AHB0052, Invitrogen), phospho-Tau (s396) (35–5300, Invitrogen), interleukin 1β (IL-1β) (PA5-95,455, Invitrogen), tumor necrosis factor α (TNF-α) (E-AB-33121, Elabscience), and β-actin (AM4302, Invitrogen) were done at 4 °C. The membranes were washed with TBST buffer four times before at RT incubating with HRP-conjugated secondary antibodies, anti-rabbit (AB6721, Abcam), anti-mouse (31,430, Invitrogen). The Femto LUCENT™ PLUS-HRP kit (AD0023, GBiosciences) was used to develop the blot for visualizing the protein bands utilizing the method of enhanced chemiluminescence.
Enzyme-linked Immunosorbent Assay (ELISA)
According to the previous protocol, ELISA was carried out. [ 53 ]. PsEV samples were subjected to freeze–thaw cycles; next, PsEVs were ultrasonicated for two minutes, with a 30-s on-and-off cycle, at an amplitude of 25. Following this, they underwent a 10-min centrifugation at 10,000 g, at 4 °C, and the obtained supernatant was used. The samples were kept at 37 °C before loading into the ELISA plates. The bicinchoninic acid (BCA) protein assay kit (23,225, ThermoFisher Scientific) was used to quantify the total protein concentration using BSA (D0024, BioBasic) as a reference. The ELISA kit was used to detect the presence of protein in 100 μL of PsEV sample are as follows: amyloid-β (1–42) (E-EL-H0543, ELabsciences), p-Tau (s-396) (E-EL-H5314, ELabsciences), IL-1β (ITLK01270, GBiosciences), TNF-α (ITLK01190, GBiosciences), GFAP (E-EL-H6093, ELabsciences), and synaptophysin (E-EL-H2014, ELabsciences). The manufacturer’s instructions were followed for every step of the process. A 96-well microplate spectrophotometer (SpectraMax i3x Multi-Mode Microplate Reader, Molecular devices) was used to measure the absorbance at 450 nm.
Data and statistical analysis
The mean age values, ACE-III score, and MMSE score were ascertained using descriptive statistical analysis Table 1 . GraphPad Prism 8.0 was used for statistical data analysis, including NTA concentration, Western blotting densitometric analysis, and ELISA. Unpaired student t -test and ANOVA were used for group analysis, and statistical significance was determined. p < 0.05 was used to assess significance. The Image J software (NIH, USA) was used for the densitometry analysis. The receiver operating characteristic (ROC) curve was used to analyze the efficiency of distinguishing the case from controls. Correlation analysis was conducted between the concentration of PsEVs and the levels of ELISA proteins, including amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin, and additionally between the PsEVs-derived levels of amyloid-β (1–42) β1-42, p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin with ACE-III and MMSE values. ROC curve is a probability curve utilized to assess the accuracy of a test. The test’s ability to distinguish between groups is indicated by the area under the curve (AUC), which acts as a quantitative measure of separability. An outstanding test typically exhibits an AUC close to 1, signifying a high level of separability. Conversely, a subpar test tends to have an AUC closer to 0, indicating a poor ability to distinguish between the two classes.
Characterization and validation of isolated sEVs
PsEVs were isolated, characterized, and validated following Minimal Information for Studies of Extracellular Vesicles (MISEV) 2018 guidelines, which suggest a protocol for documenting work specifically with extracellular vesicles [ 56 ]. PsEVs from AMC, MCI, and AD subjects were morphologically characterized by transmission electron microscopy, and spherical lipid bi-layered vesicles were observed in the size range of sEVs (Fig. 1 A–C). In Fig. 1 D–F, the size distribution and concentration of PsEVs were observed in the size range of 30–200 nm in diameter by NTA, which is within the sEVs’ size range. The mean concentration of PsEVs in AMC, MCI, and AD patients were 5.12E + 10, 2.6E + 11, and 3.13E + 11 particle/ml, respectively, with higher concentrations of PsEVs in MCI and AD than in AMC ( p < 0.0001) (Fig. 1 G). To differentiate AD from AMC, ROC and AUC analyses were performed where the AUC = 0.9748, with a sensitivity of 97.14% and specificity of 70.01% (Fig. 1 H), while in AMC versus MCI, AUC = 0.987, sensitivity of 96% and specificity of 86.67% (Fig. 1 I). Furthermore, we could also differentiate between MCI and AD, AUC = 0.629, sensitivity of 60%, and specificity of 56% (Fig. 1 J). Validation of PsEVs was done using immunoblot for sEVs-specific markers (CD63, CD81, and TSG101), which showed a significant increase in expressions in MCI and AD than in AMC (CD63, p = 0.0489, 0.0478 (Additional File 1 : Fig. S1); CD81, p = 0.0172, 0.0133 (Additional File 1 : Fig. S2); TSG101 p = 0.0240, 0.0329 (Additional File 1 : Fig. S3)) for AD and MCI respectively (Fig. 2 A–D). Additionally, higher L1CAM (neuron-associated marker) expression was observed in MCI ( p = 0.0100) and AD ( p = 0.0184) (Additional File 1 : Fig. S4) compared to AMC (Fig. 2 E). All densitometric values were normalized against β-actin, which was used as a loading control (Additional File 1 : Fig. S7).

Isolation and analysis of PsEVs. The isolated PsEV morphology characterize by transmission electron microscopy from age-matched healthy controls (AMC) ( A ), mild-cognitive impairment (MCI) patients ( B ), and Alzheimer’s disease (AD) ( C ). The size distribution of PsEVs subpopulation (nm) versus the concentration (particle/ml) in AMC ( D ), individuals with MCI ( E ), and AD ( F ). Comparison of the sEVs concentration of AD, MCI, and AMC patients ( G ). Receiver operating characteristic (ROC) curve of PsEVs concentration in AMC v/s AD ( H ), AMC v/s MCI ( I ), and MCI v/s AD ( J ) (scale bar 100 nm)

Validation of PsEVs expression analysis of different markers in PsEVs in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease patients (AD) ( A ). Densitometric analysis of CD63 ( B ), densitometric analysis of CD81 ( C ), densitometric analysis of TSG101 ( D ), densitometric analysis of L1CAM ( E ), densitometric analysis of synaptophysin ( F ), densitometric analysis of GFAP ( G ), and densitometric analysis of amyloid-β (1–42) oligomer ( H ). All densitometric values were normalized against β-actin
Differential expression of amyloid-β (1–42), p-Tau, synaptophysin, GFAP markers, and levels of IL-1β and TNF-α in PsEVs
Using ELISA, we measured levels of amyloid-β (1–42) and p-Tau in PsEVs from AMC, MCI, and AD patients. The significant increase of amyloid-β (1–42) and p-Tau among the groups (Fig. 3 A–H). Amyloid-β (1–42) levels were higher in MCI compared to AMC ( p < 0.0001) and more significant in AD than in MCI and AMC ( p < 0.0001) (Fig. 3 A). Similarly, in comparison to MCI and AMC, p-Tau levels were significantly higher in AD ( p < 0.0001) (Fig. 3 E). Similar levels of both markers were found in their Western blots (Fig. 2 ). We checked GFAP (astrocytic marker) and proinflammatory cytokines (TNF-α and IL-1β) to evaluate neuroinflammation. For proinflammatory markers, IL-1β and TNF-α levels showed a significant increase among the three groups ( p < 0.0001 for IL-1β and TNF-α) (Fig. 3 I, M). When comparing AD to MCI and AMC, the GFAP concentration in PsEVs was significantly higher ( p < 0.0001) (Fig. 3 Q). Similar trends were observed with Western blot analysis (Fig. 2 , Additional File 1 : Fig. S6, S9). Their elevated levels suggest prominent neuroinflammatory conditions contributing to potential neuronal damage. The elevated levels of these neuroinflammatory markers could be due to the activation of astrocytes and microglia and the subsequent increase in the secretion of PsEVs containing proinflammatory proteins, which suggests prominent neuroinflammatory conditions that may contribute to neuronal damage [ 57 ]. While synaptophysin concentration in PsEVs was downregulated in AD and MCI compared to AMC ( p < 0.0001) in ELISA (Fig. 3 U), it shows synaptic dysfunction. We also checked synaptophysin levels in PsEVs in Western blotting, finding it was downregulated in AD compared to MCI and AMC ( p = 0.0045, 0.0142), indicating synaptic degeneration in AD (Fig. 2 , Additional File 1 : Fig. S5). In MCI, synaptophysin levels did not significantly differ from AMC (Fig. 2 F). This aligns with synaptic loss in AD, reflected in lower neuropsychological test scores indicating more pronounced cognitive impairment compared to MCI and AMC.

PsEVs derived amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin protein concentration was measured. ELISA results in A shows levels of PsEVs amyloid-β (1–42) in AMC, MCI, and AD and receiver operating characteristic (ROC) curve of PsEVs concentration in AMC v/s MCI ( B ), AMC v/s AD ( C ), and MCI v/s AD ( D ). Similarly, p-Tau concentration in AMC, MCI, and AD ( E ), ROC curve of PsEVs concentration in AMC v/s MCI ( F ), AMC v/s AD ( G ), and MCI v/s AD ( H ). PsEVs derived IL-1β concentration in AMC, MCI and AD ( I ), ROC curve of PsEVs concentration in AMC v/s MCI ( J ), AMC v/s AD ( K ), and MCI v/s AD ( L ). PsEVs derived TNF-α concentration in AMC, MCI and AD ( M ), ROC curve of PsEVs concentration in AMC v/s MCI ( N ), AMC v/s AD ( O ), and MCI v/s AD ( P ). Similarly, GFAP concentration in AMC, MCI, and AD ( Q ), ROC curve of PsEVs concentration in AMC v/s MCI ( R ), AMC v/s AD ( S ), and MCI v/s AD ( T ). For PsEVs-derived synaptophysin concentration in AMC, MCI, and AD ( U ), ROC curve of PsEVs concentration in AMC v/s MCI ( V ), AMC v/s AD ( W ), and MCI v/s AD ( X ). Abbreviations: AMC, age-matched control; MCI, mild-cognitive impairment patients; AD, Alzheimer’s disease patients; TNF-α, tumor necrosis factor-alpha; GFAP, glial fibrillary acidic protein
Determining the diagnostic potential of PsEVs-derived amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP and synaptophysin
We observed the levels of amyloid-β (1–42) and p-Tau in PsEVs, where the increase in amyloid-β (1–42) and p-Tau levels underscores their potential as biomarkers of MCI and AD. The diagnostic efficacy of amyloid-β (1–42) by ROC analysis was observed for AMC vs MCI [AUC = 0.9347, p < 0.0001, sensitivity (Sn) = 92%, specificity (Sp) = 80%] (Fig. 3 B), AMC vs AD (AUC = 0.9862, p < 0.0001, Sn = 91.43%, Sp = 96.67%) (Fig. 3 C), and MCI vs AD (AUC of 0.8457, p < 0.0001, Sn = 80%, and Sp = 72%) (Fig. 3 D). Similarly, diagnostic efficacy of p-Tau by ROC analysis was observed for AMC vs MCI (AUC = 0.8760, p < 0.0001, Sn = 88%, Sp = 83.33%) (Fig. 3 F), AMC vs AD (AUC = 0.9757, p < 0.0001, Sn = 94.29%, Sp = 83.33%) (Fig. 3 G), and MCI vs AD (AUC of 0.9074, p < 0.0001, Sn = 88.57%, and Sp = 92%) (Fig. 3 H). So, we observed that the pathological hallmarks of the disease, viz., amyloid-β (1–42) and p-Tau levels, are increased significantly in PsEVs cargo of AD and MCI groups.
Furthermore, we also checked GFAP, TNF-α, IL-1β, and synaptophysin in PsEVs from MCI and AD groups. The diagnostic efficacy of IL-1β by ROC analysis was observed for AMC vs MCI (AUC = 0.9520, p < 0.0001, Sn = 96%, Sp = 86.67%) (Fig. 3 J), AMC vs AD (AUC = 0.9857, p < 0.0001, Sn = 94.29%, Sp = 90%) compared to AMC (Fig. 3 K), MCI vs AD (AUC = 0.9114, p < 0.0001, Sn = 85.71%, Sp = 92%) (Fig. 3 L). Similarly, diagnostic efficacy of TNF-α by ROC analysis was observed for AMC vs MCI (AUC = 0.8920, p < 0.0001, Sn = 84%, Sp = 80%) (Fig. 3 N), AMC vs AD (AUC = 0.9848, p < 0.0001, Sn = 88.57%, Sp = 96.67%), and MCI vs AD (AUC = 0.9280, p < 0.0001, Sn = 88.57%, Sp = 96%) (Fig. 3 P). So, we observed an elevated expression of neuroinflammatory markers within the PsEVs isolated from the AD and MCI groups.
GFAP is an activation marker of astroglia, and in AD, this activation is associated with synaptic dysfunction [ 58 ]. In PsEVs, the diagnostic efficacy of GFAP by ROC analysis was observed as for AMC vs MCI (AUC = 0.8393, p < 0.0001, Sn = 88%, Sp = 76.67%) (Fig. 3 R), AMC vs. AD (AUC = 0.8814, p < 0.0001, Sn = 91.43%, Sp = 76.67%) compared to AMC (Fig. 3 S); MCI vs AD (AUC = 0.7657, p < 0.0001, Sn = 74.29%, Sp = 72%) (Fig. 3 T). In addition to this, we also checked the level of presynaptic protein, i.e., synaptophysin, within the PsEVs, as the level of synaptophysin correlates with cognitive decline in AD [ 59 ]. The diagnostic efficacy of synaptophysin by ROC analysis was observed as follows for AMC vs MCI (AUC = 0.8507, p < 0.0001, Sn = 80%, Sp = 86.67%) (Fig. 3 V), AMC vs AD (AUC = 0.9738, p < 0.0001, Sn = 88.57%, Sp = 96.67%) compared to AMC (Fig. 3 W); MCI vs AD (AUC = 0.8291, p < 0.0001, Sn = 85.71%, and Sp = 68%) (Fig. 3 X). Table 2 summarizes all the AUC, sensitivity, specificity, and p -value values for all the PsEVs-derived proteins.
Correlations of PsEVs concentration values with protein levels of amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin in PsEVs
As we found an elevated number of PsEVs in the diseased condition, we performed a correlation analysis between PsEVs concentration and the amyloid-β (1–42) level, p-Tau, IL-1β, and TNF-α within PsEV. We found that PsEV concentration was positively correlated with all the protein levels except synaptophysin, which showed a negative correlation (Fig. 4 ). In these correlations, amyloid-β (1–42) was positively correlated ( r = 0.7196, p < 0.0001) (Fig. 4 A); p-Tau positively correlates ( r = 0.7960, p < 0.0001) (Fig. 4 B); IL-1β also showed positive correlation ( r = 0.7220, p < 0.0001) (Fig. 4 C); and TNF-α also showed positive correlation ( r = 0.6473, p < 0.0001) (Fig. 4 D). GFAP showed a weak correlation with PsEVs concentration ( r = 0.5155, p < 0.0001) (Fig. 4 E), and synaptophysin showed a weak correlation ( r = 0.5752, p < 0.0001) (Fig. 4 F).

Correlation analysis between PsEVs concentration and PsEVs derived AD pathology markers. The correlation between PsEVs concentration with the amyloid-β (1–42) ( A ), p-Tau ( B ), IL-1β ( C ), TNF-α ( D ), GFAP ( E ), and synaptophysin ( F ). Abbreviations: p-Tau, Phospho-Tau, TNF-α, tumor necrosis factor-alpha; GFAP, glial fibrillary acidic protein. Spearman correlation was used for correlation analysis
Correlations of ACE-III and MMSE scores with protein levels of amyloid-β (1–42), p-Tau, IL-1β, and TNF-α in PsEVs
We performed a correlation analysis between ACE-III and MMSE values with the level of amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin (Fig. 5 ). We found that ACE-III and MMSE values were negatively correlated with all the protein levels except synaptophysin, which showed a positive value for the correlation coefficient. ACE-III values showed a negative correlation with amyloid-β (1–42) ( r = − 0.5107, p < 0.0001) (Fig. 5 A), p-Tau ( r = − 0.5055, p < 0.0001) (Fig. 5 B), IL-1β ( r = − 0.5684, p < 0.0001) (Fig. 5 C), and TNF-α ( r = − 0.6110, p < 0.0001) (Fig. 5 D). ACE-III values showed a negative correlation with GFAP ( r = − 0.5024, p < 0.0001) (Fig. 5 E), while synaptophysin showed a positive correlation ( r = 0.5036, p < 0.0001) (Fig. 5 F). In the case of MMSE, the values were as follows: for amyloid-β (1–42) ( r = − 0.5276, p < 0.0001) (Fig. 5 G), p-Tau ( r = − 0.6081, p < 0.0001) (Fig. 5 H), IL-1β ( r = − 0.5743, p < 0.0001) (Fig. 5 I), TNF-α ( r = − 0.5522, p < 0.0001) (Fig. 5 J), GFAP ( r = − 0.4596 p = 0.0002) (Fig. 5 K), and synaptophysin ( r = 0.5428, p < 0.0001) (Fig. 5 L). Table 3 summarizes all the values of Correlation coefficients for all the PsEVs-derived proteins.

Correlation between neuropsychological test (ACE-III and MMSE) and PsEV-derived AD pathology markers. Amyloid-β (1–42) β, p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin protein concentration. A – F Correlation between ACE-III scores and amyloid-β (1–42) ( A ), pTau ( B ), IL-1β ( C ), TNF-α ( D ), GFAP ( E ), and synaptophysin ( F ) protein concentration. G – L A correlation between MMSE Score and amyloid-β (1–42) ( G ), p-Tau (H), IL-1β ( I ), TNF-α ( J ), GFAP ( K ), and synaptophysin ( L ) protein concentration. Abbreviations: ACE-III, Addenbrooke Cognitive Examination; MMSE, Mini-Mental State Examination; p-Tau, Phospho-Tau; TNF-α, tumor necrosis factor-alpha; GFAP, glial fibrillary acidic protein. Spearman correlation was used for correlation analysis
In this study, we aimed to investigate the capacity of PsEVs to mirror pathological processes linked to AD and MCI. sEVs are extensively documented in the propagation of pathological processes associated with neurodegenerative and metabolic disorders [ 60 ]. The increased secretion of sEVs, coupled with the transmission of disease-related pathologies through sEVs-associated cargo, makes sEVs a viable candidate for understanding the physiological state of their originating cells, which is reflected in sEVs cargo [ 61 ]. To isolate the PsEVs, we employed a combined approach involving chemical precipitation followed by ultrafiltration, which effectively eliminates co-precipitants and minute protein contaminants such as albumin and LDL. We employed the neuronal protein L1CAM as a marker to ascertain the neuronal origin, although there is a debate surrounding its specificity for neuronal origin [ 62 ]. Nevertheless, in our study, the L1CAM marker is used to check for protein markers and not to confirm L1CAM affinity-based isolation. A two-step filtration procedure was used to accompany the sEV isolation method in our study to ensure high purity. Spherical lipid bi-layered vesicles within the typical size range of small extracellular vesicles (30–150 nm) were observed across AD, MCI, and AMC subjects (Fig. 1 A–C). NTA was employed to study the size distribution of sEVs in AD, MCI, and AMC. We observed that the isolated PsEVs come within the size range of < 200 nm, and there was a notable increase in the number of particles in diseased conditions compared to the control group. (Fig. 1 D–G).
Validation using sEVs-specific markers (CD63, CD81, and TSG101) demonstrated a noteworthy upregulation in MCI and AD, indicating PsEVs numbers are increased in disease conditions (Fig. 2 A–D). Levels of sEV-specific markers in AD and MCI are elevated because PsEV numbers are increased in the disease condition. As documented by various studies in MCI and AD, there is an increase in cross-talk between different pathophysiological processes, which leads to an increase in sEVs number and sEVs specific marker as a cellular response to heightened cellular stress aggravating neuronal damage and synaptic dysfunction [ 33 , 63 , 64 ]. Neuroinflammation, a characteristic feature of AD and MCI, may lead to the release of sEVs with inflammatory markers. Synaptic dysfunction, evidenced by synaptic degeneration, could contribute to the increased sEV-specific markers, reflecting vesicle release in response to altered synaptic activity [ 9 , 65 ]. Additionally, cells undergoing stress might activate compensatory mechanisms, and the elevated sEV-specific markers could signify communication for potential repair or damage mitigation. Therefore, the increase in sEV-specific markers may be linked to the progression of neurodegenerative processes, indicating ongoing pathological changes in the brain as the disease progresses. Additionally, the elevated expression of L1CAM, a neuron-associated marker, in MCI and AD further strengthens the association between PsEVs and neurodegenerative processes (Fig. 2 E). Furthermore, our observations extend beyond AD and MCI, showing increased concentrations of sEVs in other health conditions where higher levels of these vesicles correlate with elevated levels of disease markers [ 53 , 54 , 55 ]. The results of our research provide valuable insight into the characterization, validation, and functional implications of plasma-derived small extracellular vesicles (PsEVs) in the context of AD and MCI. Our comprehensive analysis encompassed morphological, biochemical, and functional aspects, shedding light on the potential role of PsEVs as biomarkers and contributors to neurodegenerative processes.
For this purpose, we performed the ELISA of amyloid-β (1–42) in PsEVs, where we observed higher protein concentrations of amyloid-β (1–42) in MCI. At the same time, in AD, the concentration also significantly increased (Fig. 3 A). In a similar study by A. Manolopoulos et al. [ 66 ], they studied levels of Aβ42, total Tau, and pro-brain-derived neurotrophic factor (BDNF) in both plasma neuron-derived extracellular vesicles (NDEVs) and plasma. The study reported a lack of correlation between the plasma and NDEVs, substantiating concerns about levels of the Aβ42 and total Tau measured in plasma originating from non-CNS sources. Multiple studies support the involvement of extracellular vesicles (EVs) in AD pathogenesis, where Aβ and Tau are released in association with EVs, influencing neuronal cell death and trans-synaptic spreading of the disease [ 7 , 15 , 54 , 67 ]. A progressive elevation in PsEV levels of p-Tau was observed in MCI, reaching a significantly higher AD concentration (Fig. 3 E). Previous research has revealed that p-tau alone effectively differentiates Frontotemporal Dementia (FTD) from AD with high specificity [ 68 , 69 ]. In our study, the alone analysis of p-Tau and amyloid-β (1–42) proved effective in distinguishing patients with MCI from AMC (Table 2 ). Consequently, studies have reported that the elevation of p-Tau suggests the future likelihood of AD development [ 70 ]. This dual elevation in amyloid-β (1–42) and p-Tau levels highlights their potential utility as concurrent biomarkers associated with MCI and AD diagnosis, as indicated by our ROC analysis. Therefore, the investigation into PsEV content revealed significant alterations in key markers associated with AD pathology, viz., amyloid-β (1–42) and p-Tau, which are a well-established marker of AD and exhibit an elevated level in PsEVs from AD and MCI patients compared to AMC in our study.
Synaptic dysfunction is considered a core feature of AD. It is suggested to precede other pathophysiological events of AD rather than neurodegeneration, which manifests during the later stages of the disease [ 71 ]. Synaptic dysfunction interacts with other core pathophysiology events of AD, such as the amyloid-β cascade, tau pathology, and neuroinflammation, eventually progressing to irreversible neurodegeneration and atrophy [ 72 , 73 ]. In this context, the synchronized exchange of proteins involved in these pathological processes between the CNS and neuronal-derived sEVs highlights the potential of sEVs as reliable carriers of pathophysiological cascade occurring at the pathological site [ 74 ]. In Fig. 3 U, we observed downregulated synaptophysin levels, a synaptic vesicle marker, in AD PsEVs compared to MCI and AMC. This suggests synaptic degeneration, which has also been discussed in several studies [ 59 , 63 , 64 ]. Synaptic damage induced by amyloid-β deposition triggers a response from the glia to eliminate impaired synapses. As amyloid-β accumulates, the severity of synaptic dysfunction intensifies, leading to tau hyperphosphorylation and the formation of tau tangles. Our study’s findings contradict J. Utz et al. (2021), which showed increased synaptophysin levels in microvesicles isolated from cerebrospinal fluid (CSF) in AD [ 28 ]. This discrepancy could be due to different biofluid sources, cellular origins, or clearance mechanisms for synaptophysin in these compartments. Our study also differs from Utz J et al. (2021) as we have studied PsEVs compared to microvesicles; both differ in biogenesis, structure, and functions. Moreover, our study aligns with existing studies that reported lower synaptophysin levels in plasma neuronal-derived EVs. Goetzl et al. [ 75 ] investigated the synaptic protein levels in neuronal-derived exosomes in plasma (NDEs) of patients with FTD and AD, where the authors found significantly lower levels of synaptopodin, neurogranin, synaptophysin, and synaptotagmin-2 in both conditions compared to controls. Furthermore, our results also align with the overall synaptic loss seen in AD patient’s brains, where lower levels of synaptophysin in the hippocampus have been reported to correlate with cognitive decline in AD [ 59 ]. Our study found that no significant difference in synaptophysin levels between MCI and AMC was observed, indicating that synapse dysfunction is more pronounced due to neuronal loss in the advanced disease stage, and its indication is reflected in PsEVs. Since the PsEVs pool also contains neuronal-derived EVs, we interpolate that the reduction in synaptic proteins in brain tissue is reflected in our results.
IL-1β, a potent immunomodulating cytokine, has previously been identified as a trigger for various inflammatory mediators in astrocytes and neurons [ 76 ]. Consistent evidence from post-mortem AD brain studies indicates the prevalent overexpression of IL-1β, with immunohistochemical analyses revealing its localization to microglia around plaques [ 77 ]. Moreover, pro-inflammatory markers (IL-1β and TNF-α) were significantly higher in PsEVs from AD and MCI subjects, as evidenced by ELISA and Western blot findings in our study (Fig. 3 I and M). Table 3 summarizes the correlation between PsEVs and neuroinflammatory markers. IL-1β plays a direct role in the pathophysiological changes associated with AD owing to its specific expression in the vicinity of plaques, and this localization suggests IL-1β as a mediator in the formation of plaques and tangles, thereby contributing to AD pathology [ 65 ]. TNF-α, another pro-inflammatory cytokine primarily secreted by activated macrophages and microglia, is recognized for its dual role in promoting cell survival and death in the central nervous system [ 78 , 79 ].
The cytoskeletal GFAP is found in astrocytic cells [ 80 ]. Increased plasma GFAP levels could result from “reactive astrogliosis,” another term for aberrant astrocytic function brought on by damage to neurons [ 81 ]. According to research on animal and cell models, reactive astrocytes encircle and penetrate amyloid-β plaques, contributing to the amyloid-β pathological process [ 82 , 83 ]. Research has demonstrated a correlation between amyloid-β burden, cognitive decline, and plasma GFAP [ 83 ]. PsEVs of GFAP were elevated in AD [ 27 ] and MCI (Fig. 3 Q). It is well known that sEVs play a pivotal role in the progression of disease pathologies in neurodegenerative and metabolic diseases [ 33 , 84 ]. The high levels of neuro-inflammatory markers (GFAP, TNF-α, and IL-1β) in PsEVs from MCI and AD subjects suggest a potential role of PsEVs in neuroinflammation. This activation of astrocytes and microglia precedes increased secretion of pro-inflammatory PsEVs and may contribute to neuronal damage and progressive cognitive impairment. Diseased conditions involve an increased secretion of sEVs and the cargo they carry, including pathological hallmark proteins or immunomodulatory cytokines [ 33 ].
Correlation analyses unveiled positive associations between PsEVs concentration and the protein levels of amyloid-β (1–42), p-Tau, IL-1β, TNF-α, GFAP, and synaptophysin (Fig. 4 ). Furthermore, our study also analyzed the correlation between cognitive examination scores (ACE-III and MMSE) and PsEV-associated protein levels (Fig. 5 ). The negative correlations observed imply that lower cognitive scores align with elevated levels of amyloid-β (1–42), p-Tau, IL-1β, and TNF-α in PsEVs Table 3 . This implies a strong connection between PsEV biomarkers and cognitive decline, reinforcing that PsEVs could serve as valuable diagnostic and prognostic tools. These findings underscore the potential of PsEVs as reliable disease progression and pathology indicators. The robust correlations further support the hypothesis that PsEVs may actively participate in disseminating neurodegenerative signals.
Our study extensively studied the multiple pathophysiological processes associated with AD by checking the protein levels involved in these processes within PsEVs, including amyloid-β (1–42), p-Tau, neuroinflammatory markers (IL-1β, TNF-α, GFAP), and synaptic protein levels. This comprehensive approach enhances diagnostic accuracy by considering the synergistic effects of these processes, providing valuable insights into disease progression from MCI to AD. We have also performed a systematic comparison with MCI, which was lacking in previous studies. We observed a significant correlation between these investigated protein levels within PsEVs and neuropsychological tests, thus filling a research gap addressing the clinical relevance of these dysregulated pathophysiological processes. The observed downregulated synaptophysin levels in AD PsEVs compared to MCI and control subjects shed light on the combined role of neuroinflammation and proteinopathy in the cognitive decline observed as the disease progresses. This finding suggests that PsEVs may reflect synaptic degeneration, opening avenues for further exploration into the role of PsEVs in synaptic damage and dysfunction in neurodegenerative diseases.
Our study provides a multifaceted examination of PsEVs, offering compelling evidence of their potential as biomarkers and functional contributors in AD. We have comprehensively discussed the synergistic role of synaptic dysfunction and neuroinflammation and their association with amyloid-β and tau pathologies within the PsEVs in AD progression. The pathophysiological conditions in the MCI and AD brain are reflected in PsEVs, as observed by the increased concentration of PsEVs containing disease-associated markers and markers for synaptic dysfunction and neuroinflammation. Therefore, the PsEVs can be exploited to understand the pathophysiological process involved in the progression and severity of MCI and AD.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
Addenbrooke Cognitive Examination
- Alzheimer’s disease
Age-matched controls
Glial fibrillary acidic protein
Interleukin-1β
- Mild cognitive impairment
Mini-Mental State Examination
Phospho-Tau
Tumor necrosis factor-alpha
Suescun J, Chandra S, Schiess MC. Chapter 13 - The role of neuroinflammation in neurodegenerative disorders. In: Actor JK, Smith KC, editors. Translational Inflammation. Academic Press; 2019. p. 241–67.
Chapter Google Scholar
DiSabato DJ, Quan N, Godbout JP. Neuroinflammation: the devil is in the details. J Neurochem. 2016;139(S2):136–53.
Article CAS PubMed PubMed Central Google Scholar
Lyman M, Lloyd DG, Ji X, Vizcaychipi MP, Ma D. Neuroinflammation: the role and consequences. Neurosci Res. 2014;79:1–12.
Article CAS PubMed Google Scholar
Mishra A, Kim HJ, Shin AH, Thayer SA. Synapse loss induced by interleukin-1β requires pre- and post-synaptic mechanisms. J Neuroimmune Pharmacol. 2012;7(3):571–8.
Article PubMed PubMed Central Google Scholar
Subramanian J, Savage JC, Tremblay MÈ. Synaptic loss in Alzheimer’s disease: mechanistic insights provided by two-photon in vivo imaging of transgenic mouse models. Front Cell Neurosci. 2020;14: 592607.
Chen GF, Xu TH, Yan Y, Zhou YR, Jiang Y, Melcher K, et al. Amyloid-β (1–42) beta: structure, biology and structure-based therapeutic development. Acta Pharmacol Sin. 2017;38(9):1205–35.
Sun X, Chen WD, Wang YD. β-Amyloid-β (1–42): the key peptide in the pathogenesis of Alzheimer’s DISEASE. Front Pharmacol. 2015;6:221.
Hampel H, Hardy J, Blennow K, Chen C, Perry G, Kim SH, et al. The amyloid-β (1–42)-β pathway in Alzheimer’s disease. Mol Psychiatry. 2021;26(10):5481–503.
Knopman DS, Amieva H, Petersen RC, Chételat G, Holtzman DM, Hyman BT, et al. Alzheimer disease. Nat Rev Dis Primers. 2021;7(1):1–21.
Article Google Scholar
Gu L, Guo Z. Alzheimer’s Aβ42 and Aβ40 peptides form interlaced Amyloid-β (1–42) fibrils. J Neurochem. 2013;126(3):305–11.
Bettens K, Sleegers K, Van Broeckhoven C. Current status on Alzheimer disease molecular genetics: from past, to present, to future. Hum Mol Genet. 2010;19(R1):R4–11.
George-Hyslop PHS. Molecular genetics of Alzheimer’s disease. Biol Psychiat. 2000;47(3):183–99.
Li NM, Liu KF, Qiu YJ, Zhang HH, Nakanishi H, Qing H. Mutations of beta-Amyloid-β (1–42) precursor protein alter the consequence of Alzheimer’s disease pathogenesis. Neural Regen Res. 2019;14(4):658–65.
Shen J, Kelleher RJ. The presenilin hypothesis of Alzheimer’s disease: evidence for a loss-of-function pathogenic mechanism. Proc Natl Acad Sci U S A. 2007;104(2):403–9.
Liu M, Sui D, Dexheimer T, Hovde S, Deng X, Wang KW, et al. Hyperphosphorylation renders Tau prone to aggregate and to cause cell death. Mol Neurobiol. 2020;57(11):4704–19.
Ferrer I, Andrés-Benito P, Ausín K, Pamplona R, del Rio JA, Fernández-Irigoyen J, et al. Dysregulated protein phosphorylation: a determining condition in the continuum of brain aging and Alzheimer’s disease. Brain Pathol. 2021;31(6): e12996.
Goel P, Chakrabarti S, Goel K, Bhutani K, Chopra T, Bali S. Neuronal cell death mechanisms in Alzheimer’s disease: an insight. Front Mol Neurosci. 2022;15: 937133.
Zhang W, Xiao D, Mao Q, Xia H. Role of neuroinflammation in neurodegeneration development. Sig Transduct Target Ther. 2023;8(1):1–32.
Choi SB, Kwon S, Kim JH, Ahn NH, Lee JH, Yang SH. The molecular mechanisms of neuroinflammation in Alzheimer’s disease, the consequence of neural cell death. Int J Mol Sci. 2023;24(14):11757.
Rajesh Y, Kanneganti TD. Innate immune cell death in neuroinflammation and Alzheimer’s disease. Cells. 2022;11(12):1885.
Skaper SD, Facci L, Zusso M, Giusti P. An inflammation-centric view of neurological disease: beyond the neuron. Front Cell Neurosci. 2018;10:00072.
Brucato DR, Benjamin DE. Synaptic pruning in Alzheimer’s disease: role of the complement system. Global J Med Res. 2020;20(F6):1–20.
Piccioni G, Mango D, Saidi A, Corbo M, Nisticò R. Targeting microglia-synapse interactions in Alzheimer’s disease. Int J Mol Sci. 2021;22(5):2342.
Mori Y, Tsuji M, Oguchi T, Kasuga K, Kimura A, Futamura A, et al. Serum BDNF as a potential biomarker of Alzheimer’s disease: verification through assessment of serum, cerebrospinal fluid, and medial temporal lobe atrophy. Front Neurol. 2021;12: 653267.
Giacomucci G, Mazzeo S, Bagnoli S, Ingannato A, Leccese D, Berti V, et al. Plasma neurofilament light chain as a biomarker of Alzheimer’s disease in subjective cognitive decline and mild cognitive impairment. J Neurol. 2022;269(8):4270–80.
Kim KY, Shin KY, Chang KA. GFAP as a potential biomarker for Alzheimer’s disease: a systematic review and meta-analysis. Cells. 2023;12(9):1309.
Ally M, Sugarman MA, Zetterberg H, Blennow K, Ashton NJ, Karikari TK, et al. Cross-sectional and longitudinal evaluation of plasma glial fibrillary acidic protein to detect and predict clinical syndromes of Alzheimer’s disease. Alzheimers Dement (Amst). 2023;15(4):e12492.
Article PubMed Google Scholar
Utz J, Berner J, Muñoz LE, Oberstein TJ, Kornhuber J, Herrmann M, et al. Cerebrospinal fluid of patients with Alzheimer’s disease contains increased percentages of synaptophysin-bearing microvesicles. Front Aging Neurosci. 2021;13: 682115.
Bruno D, Schurmann VS. Addenbrooke’s cognitive examination III in the diagnosis of dementia: a critical review. Neuropsychiatr Dis Treat. 2019;15:441–7.
Matías-Guiu JA, Valles-Salgado M, Rognoni T, Hamre-Gil F, Moreno-Ramos T, Matías-Guiu J. Comparative diagnostic accuracy of the ACE-III, MIS, MMSE, MoCA, and RUDAS for screening of Alzheimer disease. Dement Geriatr Cogn Disord. 2017;43(5–6):237–46.
Bajpai S, Upadhyay A, Sati H, Pandey RM, Chaterjee P, Dey AB. Hindi version of Addenbrook’s Cognitive Examination III: distinguishing cognitive impairment among older Indians at the lower cut-offs. Clin Interv Aging. 2020;15:329–39.
Howitt J, Hill AF. Exosomes in the pathology of neurodegenerative diseases. J Biol Chem. 2016;291(52):26589–97.
Rastogi S, Sharma V, Bharti PS, Rani K, Modi GP, Nikolajeff F, et al. The evolving landscape of exosomes in neurodegenerative diseases: exosomes characteristics and a promising role in early diagnosis. Int J Mol Sci. 2021;22(1):440.
Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):eaau6977.
Gomes P, Tzouanou F, Skolariki K, Vamvaka-Iakovou A, Noguera-Ortiz C, Tsirtsaki K, et al. Extracellular vesicles and Alzheimer’s disease in the novel era of Precision Medicine: implications for disease progression, diagnosis and treatment. Exp Neurol. 2022;358: 114183.
Cocucci E, Meldolesi J. Ectosomes and exosomes: shedding the confusion between extracellular vesicles. Trends Cell Biol. 2015;25(6):364–72.
Pegtel DM, Gould SJ. Exosomes. Annu Rev Biochem. 2019Jun;20(88):487–514.
Gámez-Valero A, Campdelacreu J, Vilas D, Ispierto L, Reñé R, Álvarez R, et al. Exploratory study on microRNA profiles from plasma-derived extracellular vesicles in Alzheimer’s disease and dementia with Lewy bodies. Transl Neurodegener. 2019;8(1):31.
Lim WQ, Michelle Luk KH, Lee KY, Nurul N, Loh SJ, Yeow ZX, et al. Small extracellular vesicles’ miRNAs: biomarkers and therapeutics for neurodegenerative diseases. Pharmaceutics. 2023;15(4):1216.
Banks WA, Sharma P, Bullock KM, Hansen KM, Ludwig N, Whiteside TL. Transport of extracellular vesicles across the blood-brain barrier: brain pharmacokinetics and effects of inflammation. Int J Mol Sci. 2020;21(12):4407.
Zhou F, Ebea P, Mutai E, Wang H, Sukreet S, Navazesh S, et al. Small extracellular vesicles in milk cross the blood-brain barrier in murine cerebral cortex endothelial cells and promote dendritic complexity in the hippocampus and brain function in C57BL/6J mice. Front Nutr. 2022;10:9838543.
Google Scholar
Eren E, Leoutsakos JM, Troncoso J, Lyketsos CG, Oh ES, Kapogiannis D. Neuronal-derived EV biomarkers track cognitive decline in Alzheimer’s disease. Cells. 2022;11(3):436.
Asai H, Ikezu S, Tsunoda S, Medalla M, Luebke J, Haydar T, et al. Depletion of microglia and inhibition of exosome synthesis halt tau propagation. Nat Neurosci. 2015;18(11):1584–93.
Söllvander S, Nikitidou E, Brolin R, Söderberg L, Sehlin D, Lannfelt L, et al. Accumulation of amyloid-β (1–42)-β by astrocytes result in enlarged endosomes and microvesicle-induced apoptosis of neurons. Mol Neurodegener. 2016;11(1):38.
Sardar Sinha M, Ansell-Schultz A, Civitelli L, Hildesjö C, Larsson M, Lannfelt L, et al. Alzheimer’s disease pathology propagation by exosomes containing toxic amyloid-β (1–42)-beta oligomers. Acta Neuropathol. 2018;136(1):41–56.
Zyśk M, Beretta C, Naia L, Dakhel A, Påvénius L, Brismar H, et al. Amyloid-β (1–42)-β accumulation in human astrocytes induces mitochondrial disruption and changed energy metabolism. J Neuroinflammation. 2023;20(1):43.
Gabrielli M, Prada I, Joshi P, Falcicchia C, D’Arrigo G, Rutigliano G, et al. Microglial large extracellular vesicles propagate early synaptic dysfunction in Alzheimer’s disease. Brain. 2022;145(8):2849–68.
Beretta C, Nikitidou E, Streubel-Gallasch L, Ingelsson M, Sehlin D, Erlandsson A. Extracellular vesicles from amyloid-β (1–42)-β exposed cell cultures induce severe dysfunction in cortical neurons. Sci Rep. 2020;10(1):19656.
Chen Y, He Y, Han J, Wei W, Chen F. Blood-brain barrier dysfunction and Alzheimer’s disease: associations, pathogenic mechanisms, and therapeutic potential. Front Aging Neurosci. 2023;15:1258640.
Garcia-Contreras M, Thakor AS. Extracellular vesicles in Alzheimer’s disease: from pathology to therapeutic approaches. Neural Regen Res. 2022;18(1):18–22.
PubMed Central Google Scholar
Vella LJ, Hill AF, Cheng L. Focus on extracellular vesicles: exosomes and their role in protein trafficking and biomarker potential in Alzheimer’s and Parkinson’s disease. Int J Mol Sci. 2016;17(2):173.
Huo L, Du X, Li X, Liu S, Xu Y. The emerging role of neural cell-derived exosomes in intercellular communication in health and neurodegenerative diseases. Front Neurosci. 2021;15: 738442.
Rastogi S, Rani K, Rai S, Singh R, Bharti PS, Sharma V, et al. Fluorescence-tagged salivary small extracellular vesicles as a nanotool in early diagnosis of Parkinson’s disease. BMC Med. 2023;21(1):335.
Rani K, Rastogi S, Vishwakarma P, Bharti PS, Sharma V, Renu K, et al. A novel approach to correlate the salivary exosomes and their protein cargo in the progression of cognitive impairment into Alzheimer’s disease. J Neurosci Methods. 2021;347: 108980.
Rai S, Bharti PS, Singh R, Rastogi S, Rani K, Sharma V, et al. Circulating plasma miR-23b-3p as a biomarker target for idiopathic Parkinson’s disease: comparison with small extracellular vesicle miRNA. Front Neurosci. 2023;17:1174951.
Théry C, Witwer KW, Aikawa E, Alcaraz MJ, Anderson JD, Andriantsitohaina R, et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J Extracell Vesicles. 2018;7(1):1535750.
Ng A, Tam WW, Zhang MW, Ho CS, Husain SF, McIntyre RS, et al. IL-1β, IL-6, TNF- α and CRP in elderly patients with depression or Alzheimer’s disease: systematic review and meta-analysis. Sci Rep. 2018;8(1):12050.
Hulshof LA, van Nuijs D, Hol EM, Middeldorp J. The role of astrocytes in synapse loss in Alzheimer’s disease: a systematic review. Front Cell Neurosci. 2022;16: 899251.
Sze CI, Troncoso JC, Kawas C, Mouton P, Price DL, Martin LJ. Loss of the presynaptic vesicle protein synaptophysin in hippocampus correlates with cognitive decline in Alzheimer disease. J Neuropathol Exp Neurol. 1997;56(8):933–44.
Yuyama K, Igarashi Y. Exosomes as carriers of Alzheimer’s amyloid-β (1–42)-ß. Front Neurosci. 2017;11:00229.
Watson LS, Hamlett ED, Stone TD, Sims-Robinson C. Neuronally derived extracellular vesicles: an emerging tool for understanding Alzheimer’s disease. Mol Neurodegener. 2019;14(1):22.
Gomes DE, Witwer KW. L1CAM-associated extracellular vesicles: a systematic review of nomenclature, sources, separation, and characterization. J Extracell Biol. 2022;1(3): e35.
Goetzl EJ, Kapogiannis D, Schwartz JB, Lobach IV, Goetzl L, Abner EL, et al. Decreased synaptic proteins in neuronal exosomes of frontotemporal dementia and Alzheimer’s disease. FASEB J. 2016;30(12):4141–8.
Goetzl EJ, Abner EL, Jicha GA, Kapogiannis D, Schwartz JB. Declining levels of functionally specialized synaptic proteins in plasma neuronal exosomes with progression of Alzheimer’s disease. FASEB J. 2018;32(2):888–93.
Jung YJ, Tweedie D, Scerba MT, Greig NH. Neuroinflammation as a factor of neurodegenerative disease: thalidomide analogs as treatments. Front Cell Develop Biol. 2019;7:00313.
Manolopoulos A, Delgado-Peraza F, Mustapic M, Pucha KA, Nogueras-Ortiz C, Daskalopoulos A, et al. Comparative assessment of Alzheimer’s disease-related biomarkers in plasma and neuron-derived extracellular vesicles: a nested case-control study. Front Mol Biosci. 2023;10:1254834.
He Z, Guo JL, McBride JD, Narasimhan S, Kim H, Changolkar L, et al. Amyloid-β (1–42)-β plaques enhance Alzheimer’s brain tau-seeded pathologies by facilitating neuritic plaque tau aggregation. Nat Med. 2018;24(1):29–38.
Pekeles H, Qureshi HY, Paudel HK, Schipper HM, Gornistky M, Chertkow H. Development and validation of a salivary tau biomarker in Alzheimer’s disease. Alzheimers Dement (Amst). 2018;11:53–60.
Silva MC, Ferguson FM, Cai Q, Donovan KA, Nandi G, Patnaik D, et al. Targeted degradation of aberrant tau in frontotemporal dementia patient-derived neuronal cell models. Elife. 2019;8:45457.
Article CAS Google Scholar
Holper S, Watson R, Yassi N. Tau as a biomarker of neurodegeneration. Int J Mol Sci. 2022;23(13):7307.
Lleó A, Núñez-Llaves R, Alcolea D, Chiva C, Balateu-Paños D, Colom-Cadena M, et al. Changes in synaptic proteins precede neurodegeneration markers in preclinical Alzheimer’s disease cerebrospinal fluid. Mol Cell Proteomics. 2019;18(3):546–60.
Guo T, Zhang D, Zeng Y, Huang TY, Xu H, Zhao Y. Molecular and cellular mechanisms underlying the pathogenesis of Alzheimer’s disease. Mol Neurodegener. 2020;15(1):40.
Breijyeh Z, Karaman R. Comprehensive review on Alzheimer’s disease: causes and treatment. Molecules. 2020;25(24):5789.
Snellman A, Ekblad LL, Koivumäki M, Lindgrén N, Tuisku J, Perälä M, et al. ASIC-E4: interplay of beta-amyloid-β (1–42), synaptic density and neuroinflammation in cognitively normal volunteers with three levels of genetic risk for late-onset Alzheimer’s disease – study protocol and baseline characteristics. Front Neurol. 2022;13: 826423.
Kinney JW, Bemiller SM, Murtishaw AS, Leisgang AM, Salazar AM, Lamb BT. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimers Dement (N Y). 2018;4:575–90.
Mrak RE, Griffin WST. Interleukin-1 and the immunogenetics of Alzheimer disease. J Neuropathol Exp Neurol. 2000;59(6):471–6.
Frankola KA, Greig NH, Luo W, Tweedie D. Targeting TNF-alpha to elucidate and ameliorate neuroinflammation in neurodegenerative diseases. CNS Neurol Disord Drug Targets. 2011;10(3):391–403.
Jayaraman A, Htike TT, James R, Picon C, Reynolds R. TNF-mediated neuroinflammation is linked to neuronal necroptosis in Alzheimer’s disease hippocampus. Acta Neuropathol Commun. 2021;9(1):159.
Jain P, Wadhwa PK, Jadhav HR. Reactive astrogliosis: role in Alzheimer’s disease. CNS Neurol Disord Drug Targets. 2015;14(7):872–9.
Kamphuis W, Mamber C, Moeton M, Kooijman L, Sluijs JA, Jansen AHP, et al. GFAP isoforms in adult mouse brain with a focus on neurogenic astrocytes and reactive astrogliosis in mouse models of Alzheimer disease. PLoS ONE. 2012;7(8): e42823.
Chatterjee P, Pedrini S, Stoops E, Goozee K, Villemagne VL, Asih PR, et al. Plasma glial fibrillary acidic protein is elevated in cognitively normal older adults at risk of Alzheimer’s disease. Transl Psychiatry. 2021;11(1):1–10.
Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):6977.
Download references
Acknowledgements
We express our gratitude to the Electron Microscopy Facility, Sophisticated Analytical Instrumentation Facility (SAIF) at AIIMS, New Delhi.
Authors’ X handles
X (Formally Twitter) handle: Saroj Kumar (corresponding author)—@skumarlabaiims.
Open access funding provided by Lulea University of Technology. The Indian Council of Medical Research (ICMR, funding number 2020–1194), Council of Scientific and Industrial Research (CSIR, funding number 09/006(0533)/2021-EMR-I), and Department of Health Research (DHR, funding numbers GIA/2020/000595, YSS/2020/000158) provided funding for this research manuscript.
Author information
Authors and affiliations.
Department of Biophysics, All India Institute of Medical Sciences, New Delhi, 110029, India
Rishabh Singh, Sanskriti Rai, Prahalad Singh Bharti, Sadaqa Zehra, Krishna Kishore Inampudi & Saroj Kumar
Department of Anatomy, All India Institute of Medical Sciences, New Delhi, India
Priya Kumari Gorai & Neerja Rani
Department of Pharmaceutical Engineering and Technology, Indian Institute of Technology BHU, Varanasi, India
Gyan Prakash Modi
Department of Biotechnology, Jamia Millia Islamia, New Delhi, India
Department of Neurology, All India Institute of Medical Sciences, New Delhi, India
Vishnu V. Y.
Department of Geriatric Medicine, All India Institute of Medical Sciences, New Delhi, India
Prasun Chatterjee
Department of Health, Education, and Technology, Lulea University of Technology, Lulea, 97187, Sweden
Fredrik Nikolajeff & Saroj Kumar
You can also search for this author in PubMed Google Scholar
Contributions
S.K. conceptualized and designed the study. R.S., S.R., P.S.B., and S.Z. performed the acquisition and analysis of data. R.S., S.R., P.S.B., S.Z., and P.K.G. performed the drafting the text or preparing the figures. R.S., S.R., P.S.B., N.R., K.D., K.K.I., P.C., V.V.Y, G.P.M., F.N., and S.K. performed the initial revision and proofreading of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Saroj Kumar .
Ethics declarations
Ethics approval and consent to participate.
The ethical clearance for this study was obtained from the institutional ethics committee of All Institute of Medical Sciences, New Delhi, India. The ethical clearance number is IECPG-670/25.08.2022. All subjects were recruited for the study after obtainment of the written informed consent form. A detailed written participant information sheet and participant informed consent form were provided to the subjects to take part in this study and their signatures were obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
12916_2024_3475_moesm1_esm.docx.
Additional file 1: Fig S1. [CD63 expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S2. [CD81 expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S3. [TSG101 expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S4. [L1CAM expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S5. [Synaptophysin (SYP) expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S6. [Glial Fibrillary Acidic Protein (GFAP) expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S7. [β-Actin expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S8. [Amyloidβ-42 Oligomer expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S9. [IL1β (A) and TNFα (B) expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis]. Fig S10. [p-Tau expression in age-matched controls (AMC), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) and their densitometric analysis].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Singh, R., Rai, S., Bharti, P.S. et al. Circulating small extracellular vesicles in Alzheimer’s disease: a case–control study of neuro-inflammation and synaptic dysfunction. BMC Med 22 , 254 (2024). https://doi.org/10.1186/s12916-024-03475-z
Download citation
Received : 27 February 2024
Accepted : 11 June 2024
Published : 20 June 2024
DOI : https://doi.org/10.1186/s12916-024-03475-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Small extracellular vesicles
- Synaptic dysfunction
- Neuroinflammation
BMC Medicine
ISSN: 1741-7015
- Submission enquiries: [email protected]
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
CBSE Class 12 Business Studies Case Studies - Controlling. Controlling is the process of monitoring organisational performance, finding out deviations (or gaps in between the actual performance and the set standards), and taking corrective action in order to achieve organisational goals (as per set standards). Nature of Controlling.
Examples. A case-control study is an observational study where researchers analyzed two groups of people (cases and controls) to look at factors associated with particular diseases or outcomes. Below are some examples of case-control studies: Investigating the impact of exposure to daylight on the health of office workers (Boubekri et al., 2014).
Revised on June 22, 2023. A case-control study is an experimental design that compares a group of participants possessing a condition of interest to a very similar group lacking that condition. Here, the participants possessing the attribute of study, such as a disease, are called the "case," and those without it are the "control.".
Internal Controls - Cash Operations. The office manager controlled the company's financial operations. She did payroll, accounts payable, invoicing and cash receipts. She rarely took time off ...
Introduction. Case-control and cohort studies are observational studies that lie near the middle of the hierarchy of evidence. These types of studies, along with randomised controlled trials, constitute analytical studies, whereas case reports and case series define descriptive studies (1). Although these studies are not ranked as highly as ...
1 Introduction to case-control studies 8 1.1 Defining a case-control study 8 1.2 Measuring association: the odds ratio 12 1.3 Methods for controlling confounding 13 1.4 Temporal aspects 16 1.5 Further details on the sampling of cases and controls 20 1.6 Bias in case-control studies 23 1.7 Use of case-control studies 26 Notes 29 2 The simplest ...
A case control study is a retrospective, observational study that compares two existing groups. Researchers form these groups based on the existence of a condition in the case group and the lack of that condition in the control group. They evaluate the differences in the histories between these two groups looking for factors that might cause a ...
A case-control study is a type of observational study commonly used to look at factors associated with diseases or outcomes. The case-control study starts with a group of cases, which are the individuals who have the outcome of interest. The researcher then tries to construct a second group of individuals called the controls, who are similar to ...
A case-control study is a type of observational study commonly used to look at factors associated with diseases or outcomes.[1] The case-control study starts with a group of cases, which are the individuals who have the outcome of interest. The researcher then tries to construct a second group of individuals called the controls, who are similar to the case individuals but do not have the ...
A case-control study was conducted to investigate if exposure to zinc oxide is a more effective skin cancer prevention measure. The study involved comparing a group of former lifeguards that had developed cancer on their cheeks and noses (cases) to a group of lifeguards without this type of cancer (controls) and assess their prior exposure to ...
Case-control studies are typically rapid, inexpensive, and simple to conduct. Samples of cases and controls are frequently taken from sources like an existing database of patient health records. Additionally, case-control studies are particularly well suited for researching the risk factors linked to uncommon diseases or conditions.
By contrast, in a case-control study the ratio of cases and controls is higher than in the underlying population in order to make more efficient use of resources. • There are two main types of case-control design; matched and unmatched. • The odds ratio is the most commonly used measure of association between exposure and outcome in a case ...
A case-control study is a retrospective study that looks back in time to find the relative risk between a specific exposure (e.g. second hand tobacco smoke) and an outcome (e.g. cancer). A control group of people who do not have the disease or who did not experience the event is used for comparison. The goal is figure out the relationship ...
At IESE, we spent a good 3 months on a module that explained this very phenomenon. Management Control is an issue that goes beyond just finding the pain area in the organization and taking ...
General Overview of Case-Control Studies. In observational studies, also called epidemiologic studies, the primary objective is to discover and quantify an association between exposures and the outcome of interest, in hopes of drawing causal inference. Observational studies can have a retrospective study design, a prospective design, a cross ...
The purpose of this article is to present in elementary mathematical and statistical terms a simple way to quickly and effectively teach and understand case-control studies, as they are commonly done in dynamic populations—without using the rare disease assumption. Our focus is on case-control studies of disease incidence ('incident ...
Case-Control Studies. Chris Nickson. Nov 3, 2020. Home CCC. OVERVIEW. a type of retrospective observational study. control patients are 'matched' using some criteria (age, gender), typically should have no history of the disease of interest and should be representative of the general population. begins with a definition of outcome or interest.
The purpose of this article is to present in elementary mathematical and statistical terms a simple way to quickly and effectively teach and understand case-control studies, as they are commonly done in dynamic populations-without using the rare disease assumption. Our focus is on case-control studies of disease incidence ('incident case ...
Significant Findings and Recommendations. Inventory Control. The company had over $5 million in inventory and had never done an annual physical count. When their bank finally required a physical ...
Question 2. State the steps in the process of controlling. (CBSE, Delhi 2017) Answer: The various steps involved in the controlling process are described below: Setting performance standards: The first step in the controlling process involves setting standards in clear, specific and measurable terms. Standards can be set in both quantitative as ...
Explain the importance of controlling highlighted in above key elements. Ans: (I) Ensuring order and discipline. (ii) Improving employee's motivation. (iii) facilitating coordination in action. Business Studies CBSE Class 12 Case Study - Controlling with answers. Managers at New York city import-export company suspected Corporate Defence ...
A case report is the description of the clinical story of a single patient, whereas a case-control study compares 2 groups of participants differing in outcome in order to determine if a suspected exposure in their past caused that difference. 1. Cases: a group of participants who have the outcome (eg. diseased individuals) 2.
current experience of controlling bracken using hand pulling and whipping in different parts of the UK. It provides some real-world experience to supplement the preliminary guidance about each control method. The detail is limited by the amount of information available. More case study . information is welcomed to allow us to add . to the guidance.
for a matched case-control study, and adjusted OR and 95% CI were reported. Three models are presented: (1) unadjusted conditional logistic regression analysis, (2) adjusted for age, sex and level of education and (3) fully adjusted for age, sex, level of education and predefined vascular risk factors. Based
To the best of our knowledge, this is the first case-control study to investigate the potential association between the pathophysiology of GAD and the pro-inflammatory cytokine, IL-2, and the anti-inflammatory cytokine, IL-10, among the Bangladeshi population. We observed that IL-10 serum levels were significantly lower in GAD patients than in ...
Warning: This episode contains mentions of bullying and suicide. A rising tide of mental health problems among teenagers has sent parents, teachers and doctors searching for answers.
However, no studies have compared the surgical efficacy of the tissue adhesive 2-octyl cyanoacrylate (SurgiSeal®) to that of traditional suture closure in Asian children undergoing surgery for lower lid epiblepharon. Methods: This is a single-center retrospective case-control study. Surgical correction for epiblepharon was performed on 22 ...
We conducted a retrospective matched case-control study in Helsinki University area hospitals during 2013-2017. Newborn singletons with moderate or severe HIE and the need for therapeutic hypothermia were included. They were identified from the hospital database using ICD-codes P91.00, P91.01 and P91.02. For every newborn with the need for ...
Data sources. The study uses monthly mumps case data in the mainland of China during the 2004-2018 period. It is from the Public Health Science Data Center [].The monthly average temperature and humidity data is from the Chinese Bureau of Statistics [].Although each school semester's opening and closing dates varied province by province, city by city, in general, the first semester of each ...
Background Alzheimer's disease (AD) is a neurodegenerative disease characterized by Aβ plaques and neurofibrillary tangles. Chronic inflammation and synaptic dysfunction lead to disease progression and cognitive decline. Small extracellular vesicles (sEVs) are implicated in AD progression by facilitating the spread of pathological proteins and inflammatory cytokines. This study investigates ...