- Open access
- Published: 20 September 2022

Factors that influence mental health of university and college students in the UK: a systematic review
- Fiona Campbell 1 ,
- Lindsay Blank 1 ,
- Anna Cantrell 1 ,
- Susan Baxter 1 ,
- Christopher Blackmore 1 ,
- Jan Dixon 1 &
- Elizabeth Goyder 1
BMC Public Health volume 22 , Article number: 1778 ( 2022 ) Cite this article
120k Accesses
71 Citations
98 Altmetric
Metrics details
Worsening mental health of students in higher education is a public policy concern and the impact of measures to reduce transmission of COVID-19 has heightened awareness of this issue. Preventing poor mental health and supporting positive mental wellbeing needs to be based on an evidence informed understanding what factors influence the mental health of students.
To identify factors associated with mental health of students in higher education.
We undertook a systematic review of observational studies that measured factors associated with student mental wellbeing and poor mental health. Extensive searches were undertaken across five databases. We included studies undertaken in the UK and published within the last decade (2010–2020). Due to heterogeneity of factors, and diversity of outcomes used to measure wellbeing and poor mental health the findings were analysed and described narratively.
We included 31 studies, most of which were cross sectional in design. Those factors most strongly and consistently associated with increased risk of developing poor mental health included students with experiences of trauma in childhood, those that identify as LGBTQ and students with autism. Factors that promote wellbeing include developing strong and supportive social networks. Students who are prepared and able to adjust to the changes that moving into higher education presents also experience better mental health. Some behaviours that are associated with poor mental health include lack of engagement both with learning and leisure activities and poor mental health literacy.
Improved knowledge of factors associated with poor mental health and also those that increase mental wellbeing can provide a foundation for designing strategies and specific interventions that can prevent poor mental health and ensuring targeted support is available for students at increased risk.
Peer Review reports
Poor mental health of students in further and higher education is an increasing concern for public health and policy [ 1 , 2 , 3 , 4 ]. A 2020 Insight Network survey of students from 10 universities suggests that “1 in 5 students has a current mental health diagnosis” and that “almost half have experienced a serious psychological issue for which they felt they needed professional help”—an increase from 1 in 3 in the same survey conducted in 2018 [ 5 ]. A review of 105 Further Education (FE) colleges in England found that over a three-year period, 85% of colleges reported an increase in mental health difficulties [ 1 ]. Depression and anxiety were both prevalent and widespread in students; all colleges reported students experiencing depression and 99% reported students experiencing severe anxiety [ 5 , 6 ]. A UK cohort study found that levels of psychological distress increase on entering university [ 7 ], and recent evidence suggests that the prevalence of mental health problems among university students, including self-harm and suicide, is rising, [ 3 , 4 ] with increases in demand for services to support student mental health and reports of some universities finding a doubling of the number of students accessing support [ 8 ]. These common mental health difficulties clearly present considerable threat to the mental health and wellbeing of students but their impact also has educational, social and economic consequences such as academic underperformance and increased risk of dropping out of university [ 9 , 10 ].
Policy changes may have had an influence on the student experience, and on the levels of mental health problems seen in the student population; the biggest change has arguably been the move to widen higher education participation and to enable a more diverse demographic to access University education. The trend for widening participation has been continually rising since the late 1960s [ 11 ] but gained impetus in the 2000s through the work of the Higher Education Funding Council for England (HEFCE). Macaskill (2013) [ 12 ] suggests that the increased access to higher education will have resulted in more students attending university from minority groups and less affluent backgrounds, meaning that more students may be vulnerable to mental health problems, and these students may also experience greater challenges in making the transition to higher education.
Another significant change has been the introduction of tuition fees in 1998, which required students to self fund up to £1,000 per academic year. Since then, tuition fees have increased significantly for many students. With the abolition of maintenance grants, around 96% of government support for students now comes in the form of student loans [ 13 ]. It is estimated that in 2017, UK students were graduating with average debts of £50,000, and this figure was even higher for the poorest students [ 13 ]. There is a clear association between a student’s mental health and financial well-being [ 14 ], with “increased financial concern being consistently associated with worse health” [ 15 ].
The extent to which the increase in poor mental health is also being seen amongst non-students of a similar age is not well understood and warrants further study. However, the increase in poor mental health specifically within students in higher education highlights a need to understand what the risk factors are and what might be done within these settings to ensure young people are learning and developing and transitioning into adulthood in environments that promote mental wellbeing.
Commencing higher education represents a key transition point in a young person’s life. It is a stage often accompanied by significant change combined with high expectations of high expectations from students of what university life will be like, and also high expectations from themselves and others around their own academic performance. Relevant factors include moving away from home, learning to live independently, developing new social networks, adjusting to new ways of learning, and now also dealing with the additional greater financial burdens that students now face.
The recent global COVID-19 pandemic has had considerable impact on mental health across society, and there is concern that younger people (ages 18–25) have been particularly affected. Data from Canada [ 16 ] indicate that among survey respondents, “almost two-thirds (64%) of those aged 15 to 24 reported a negative impact on their mental health, while just over one-third (35%) of those aged 65 and older reported a negative impact on their mental health since physical distancing began” (ibid, p.4). This suggests that older adults are more prepared for the kind of social isolation which has been brought about through the response to COVID-19, whereas young adults have found this more difficult to cope with. UK data from the National Union of Students reports that for over half of UK students, their mental health is worse than before the pandemic [ 17 ]. Before COVID-19, students were already reporting increasing levels of mental health problems [ 2 ], but the COVID-19 pandemic has added a layer of “chronic and unpredictable” stress, creating the perfect conditions for a mental health crisis [ 18 ]. An example of this is the referrals (both urgent and routine) of young people with eating disorders for treatment in the NHS which almost doubled in number from 2019 to 2020 [ 19 ]. The travel restrictions enforced during the pandemic have also impacted on student mental health, particularly for international students who may have been unable to commence studies or go home to see friends and family during holidays [ 20 ].
With the increasing awareness and concern in the higher education sector and national bodies regarding student mental health has come increasing focus on how to respond. Various guidelines and best practice have been developed, e.g. ‘Degrees of Disturbance’ [ 21 ], ‘Good Practice Guide on Responding to Student Mental Health Issues: Duty of Care Responsibilities for Student Services in Higher Education’ [ 22 ] and the recent ‘The University Mental Health Charter’ [ 2 ]. Universities UK produced a Good Practice Guide in 2015 called “Student mental wellbeing in higher education” [ 23 ]. An increasing number of initiatives have emerged that are either student-led or jointly developed with students, and which reflect the increasing emphasis students and student bodies place on mental health and well-being and the increased demand for mental health support: Examples include: Nightline— www.nightline.ac.uk , Students Against Depression— www.studentsagainstdepression.org , Student Minds— www.studentminds.org.uk/student-minds-and-mental-wealth.html and The Alliance for Student-Led Wellbeing— www.alliancestudentwellbeing.weebly.com/ .
Although requests for professional support have increased substantially [ 24 ] only a third of students with mental health problems seek support from counselling services in the UK [ 12 ]. Many students encounter barriers to seeking help such as stigma or lack of awareness of services [ 25 ], and without formal support or intervention, there is a risk of deterioration. FE colleges and universities have identified the need to move beyond traditional forms of support and provide alternative, more accessible interventions aimed at improving mental health and well-being. Higher education institutions have a unique opportunity to identify, prevent, and treat mental health problems because they provide support in multiple aspects of students’ lives including academic studies, recreational activities, pastoral and counselling services, and residential accommodation.
In order to develop services that better meet the needs of students and design environments that are supportive of developing mental wellbeing it is necessary to explore and better understand the factors that lead to poor mental health in students.
Research objectives
The overall aim of this review was to identify, appraise and synthesise existing research evidence that explores the aetiology of poor mental health and mental wellbeing amongst students in tertiary level education. We aimed to gain a better understanding of the mechanisms that lead to poor mental health amongst tertiary level students and, in so doing, make evidence-based recommendations for policy, practice and future research priorities. Specific objectives in line with the project brief were to:
To co-produce with stakeholders a conceptual framework for exploring the factors associated with poorer mental health in students in tertiary settings. The factors may be both predictive, identifying students at risk, or causal, explaining why they are at risk. They may also be protective, promoting mental wellbeing.
To conduct a review drawing on qualitative studies, observational studies and surveys to explore the aetiology of poor mental health in students in university and college settings and identify factors which promote mental wellbeing amongst students.
To identify evidence-based recommendations for policy, service provision and future research that focus on prevention and early identification of poor mental health
Methodology
Identification of relevant evidence.
The following inclusion criteria were used to guide the development of the search strategy and the selection of studies.
We included students from a variety of further education settings (16 yrs + or 18 yrs + , including mature students, international students, distance learning students, students at specific transition points).
Universities and colleges in the UK. We were also interested in the context prior to the beginning of tertiary education, including factors during transition from home and secondary education or existing employment to tertiary education.
Any factor shown to be associated with mental health of students in tertiary level education. This included clinical indicators such as diagnosis and treatment and/or referral for depression and anxiety. Self-reported measures of wellbeing, happiness, stress, anxiety and depression were included. We did not include measures of academic achievement or engagement with learning as indicators of mental wellbeing.
Study design
We included cross-sectional and longitudinal studies that looked at factors associated with mental health outcomes in Table 5 .
Data extraction and quality appraisal
We extracted and tabulated key data from the included papers. Data extraction was undertaken by one reviewer, with a 10% sample checked for accuracy and consistency The quality of the included studies were evaluated using the Newcastle-Ottawa Scale [ 26 ] and the findings of the quality appraisal used in weighting the strength of associations and also identifying gaps for future high quality research.
Involvement of stakeholders
We recruited students, ex-students and parents of students to a public involvement group which met on-line three times during the process of the review and following the completion of the review. During a workshop meeting we asked for members of the group to draw on their personal experiences to suggest factors which were not mentioned in the literature.
Methods of synthesis
We undertook a narrative synthesis [ 27 ] due to the heterogeneity in the exposures and outcomes that were measured across the studies. Data showing the direction of effects and the strength of the association (correlation coefficients) were recorded and tabulated to aid comparison between studies.
Search strategy
Searches were conducted in the following electronic databases: Medline, Applied Social Sciences Index and Abstracts (ASSIA), International Bibliography of Social Sciences (IBSS), Science,PsycINFO and Science and Social Sciences Ciatation Indexes. Additional searches of grey literature, and reference lists of included studies were also undertaken.
The search strategy combined a number of terms relating to students and mental health and risk factors. The search terms included both subject (MeSH) and free-text searches. The searches were limited to papers about humans in English, published from 2010 to June 2020. The flow of studies through the review process is summarised in Fig. 1 .

Flow diagram
The full search strategy for Medline is provided in Appendix 1 .
Thirty-one quantitative, observational studies (39 papers) met the inclusion criteria. The total number of students that participated in the quantitative studies was 17,476, with studies ranging in size from 57 to 3706. Eighteen studies recruited student participants from only one university; five studies (10 publications) [ 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 ] included seven or more universities. Six studies (7 publications) [ 35 , 36 , 37 , 38 , 39 , 40 , 41 ] only recruited first year students, while the majority of studies recruited students from a range of year groups. Five studies [ 39 , 42 , 43 , 44 , 45 ] recruited only, or mainly, psychology students which may impact on the generalisability of findings. A number of studies focused on students studying particular subjects including: nursing [ 46 ] medicine [ 47 ], business [ 48 ], sports science [ 49 ]. One study [ 50 ] recruited LGBTQ (lesbian, gay, bisexual, transgender, intersex, queer/questioning) students, and one [ 51 ] recruited students who had attended hospital having self-harmed. In 27 of the studies, there were more female than male participants. The mean age of the participants ranged from 19 to 28 years. Ethnicity was not reported in 19 of the studies. Where ethnicity was reported, the proportion that were ‘white British’ ranged from 71 – 90%. See Table 1 for a summary of the characteristics of the included studies and the participants.
Design and quality appraisal of the included studies
The majority of included studies ( n = 22) were cross-sectional surveys. Nine studies (10 publications) [ 35 , 36 , 39 , 41 , 43 , 50 , 51 , 52 , 53 , 62 ] were longitudinal in design, recording survey data at different time points to explore changes in the variables being measured. The duration of time that these studies covered ranged from 19 weeks to 12 years. Most of the studies ( n = 22) only recruited participants from a single university. The use of one university setting and the large number of studies that recruited only psychology students weakens the wider applicability of the included studies.
Quantitative variables
Included studies ( n = 31) measured a wide range of variables and explored their association with poor mental health and wellbeing. These included individual level factors: age, gender, sexual orientation, ethnicity and a range of psychological variables. They also included factors that related to mental health variables (family history, personal history and mental health literacy), pre-university factors (childhood trauma and parenting behaviour. University level factors including social isolation, adjustment and engagement with learning. Their association was measured against different measures of positive mental health and poor mental health.
Measurement of association and the strength of that association has some limitations in addressing our research question. It cannot prove causality, and nor can it capture fully the complexity of the inter-relationship and compounding aspect of the variables. For example, the stress of adjustment may be manageable, until it is combined with feeling isolated and out of place. Measurement itself may also be misleading, only capturing what is measureable, and may miss variables that are important but not known. We included both qualitative and PPI input to identify missed but important variables.
The wide range of variables and different outcomes, with few studies measuring the same variable and outcomes, prevented meta-analyses of findings which are therefore described narratively.
The variables described were categorised during the analyses into the following categories:
Vulnerabilities – factors that are associated with poor mental health
Individual level factors including; age, ethnicity, gender and a range of psychological variables were all measured against different mental health outcomes including depression, anxiety, paranoia, and suicidal behaviour, self-harm, coping and emotional intelligence.
Six studies [ 40 , 42 , 47 , 50 , 60 , 63 ] examined a student’s ages and association with mental health. There was inconsistency in the study findings, with studies finding that age (21 or older) was associated with fewer depressive symptoms, lower likelihood of suicide ideation and attempt, self-harm, and positively associated with better coping skills and mental wellbeing. This finding was not however consistent across studies and the association was weak. Theoretical models that seek to explain this mechanism have suggested that older age groups may cope better due to emotion-regulation strategies improving with age [ 67 ]. However, those over 30 experienced greater financial stress than those aged 17-19 in another study [ 63 ].
Sexual orientation
Four studies [ 33 , 40 , 64 , 68 ] examined the association between poor mental health and sexual orientation status. In all of the studies LGBTQ students were at significantly greater risk of mental health problems including depression [ 40 ], anxiety [ 40 ], suicidal behaviour [ 33 , 40 , 64 ], self harm [ 33 , 40 , 64 ], use of mental health services [ 33 ] and low levels of wellbeing [ 68 ]. The risk of mental health problems in these students compared with heterosexual students, ranged from OR 1.4 to 4.5. This elevated risk may reflect the greater levels of isolation and discrimination commonly experienced by minority groups.
Nine studies [ 33 , 38 , 39 , 40 , 42 , 47 , 50 , 60 , 63 ] examined whether gender was associated mental health variables. Two studies [ 33 , 47 ] found that being female was statistically significantly associated with use of mental health services, having a current mental health problem, suicide risk, self harm [ 33 ] and depression [ 47 ]. The results were not consistent, with another study [ 60 ] finding the association was not significant. Three studies [ 39 , 40 , 42 ] that considered mediating variables such as adaptability and coping found no difference or very weak associations.
Two studies [ 47 , 60 ] examined the extent to which ethnicity was associated with mental health One study [ 47 ] reported that the risks of depression were significantly greater for those who categorised themselves as non-white (OR 8.36 p = 0.004). Non-white ethnicity was also associated with poorer mental health in another cross-sectional study [ 63 ]. There was no significant difference in the McIntyre et al. (2018) study [ 60 ]. The small number of participants from ethnic minority groups represented across the studies means that this data is very limited.
Family factors
Six studies [ 33 , 40 , 42 , 50 , 60 ] explored the association of a concept that related to a student’s experiences in childhood and before going to university. Three studies [ 40 , 50 , 60 ] explored the impact of ACEs (Adverse Childhood Experiences) assessed using the same scale by Feletti (2009) [ 69 ] and another explored the impact of abuse in childhood [ 46 ]. Two studies examined the impact of attachment anxiety and avoidance [ 42 ], and parental acceptance [ 46 , 59 ]. The studies measured different mental health outcomes including; positive and negative affect, coping, suicide risk, suicide attempt, current mental health problem, use of mental health services, psychological adjustment, depression and anxiety.
The three studies that explored the impact of ACE’s all found a significant and positive relationship with poor mental health amongst university students. O’Neill et al. (2018) [ 50 ] in a longitudinal study ( n = 739) showed that there was in increased likelihood in self-harm and suicidal behaviours in those with either moderate or high levels of childhood adversities (OR:5.5 to 8.6) [ 50 ]. McIntyre et al. (2018) [ 60 ] ( n = 1135) also explored other dimensions of adversity including childhood trauma through multiple regression analysis with other predictive variables. They found that childhood trauma was significantly positively correlated with anxiety, depression and paranoia (ß = 0.18, 0.09, 0.18) though the association was not as strong as the correlation seen for loneliness (ß = 0.40) [ 60 ]. McLafferty et al. (2019) [ 40 ] explored the compounding impact of childhood adversity and negative parenting practices (over-control, overprotection and overindulgence) on poor mental health (depression OR 1.8, anxiety OR 2.1 suicidal behaviour OR 2.3, self-harm OR 2.0).
Gaan et al.’s (2019) survey of LGBTQ students ( n = 1567) found in a multivariate analyses that sexual abuse, other abuse from violence from someone close, and being female had the highest odds ratios for poor mental health and were significantly associated with all poor mental health outcomes [ 33 ].
While childhood trauma and past abuse poses a risk to mental health for all young people it may place additional stresses for students at university. Entry to university represents life stage where there is potential exposure to new and additional stressors, and the possibility that these students may become more isolated and find it more difficult to develop a sense of belonging. Students may be separated for the first time from protective friendships. However, the mechanisms that link childhood adversities and negative psychopathology, self-harm and suicidal behaviour are not clear [ 40 ]. McLafferty et al. (2019) also measured the ability to cope and these are not always impacted by childhood adversities [ 40 ]. They suggest that some children learn to cope and build resilience that may be beneficial.
McLafferty et al. (2019) [ 40 ] also studied parenting practices. Parental over-control and over-indulgence was also related to significantly poorer coping (OR -0.075 p < 0.05) and this was related to developing poorer coping scores (OR -0.21 p < 0.001) [ 40 ]. These parenting factors only became risk factors when stress levels were high for students at university. It should be noted that these studies used self-report, and responses regarding views of parenting may be subjective and open to interpretation. Lloyd et al.’s (2014) survey found significant positive correlations between perceived parental acceptance and students’ psychological adjustment, with paternal acceptance being the stronger predictor of adjustment.
Autistic students may display social communication and interaction deficits that can have negative emotional impacts. This may be particularly true during young adulthood, a period of increased social demands and expectations. Two studies [ 56 ] found that those with autism had a low but statistically significant association with poor social problem-solving skills and depression.
Mental health history
Three studies [ 47 , 51 , 68 ] investigated mental health variables and their impact on mental health of students in higher education. These included; a family history of mental illness and a personal history of mental illness.
Students with a family history or a personal history of mental illness appear to have a significantly greater risk of developing problems with mental health at university [ 47 ]. Mahadevan et al. (2010) [ 51 ] found that university students who self-harm have a significantly greater risk (OR 5.33) of having an eating disorder than a comparison group of young adults who self-harm but are not students.
Buffers – factors that are protective of mental wellbeing
Psychological factors.
Twelve studies [ 29 , 39 , 40 , 41 , 42 , 43 , 46 , 49 , 54 , 58 , 64 ] assessed the association of a range of psychological variables and different aspects of mental wellbeing and poor mental health. We categorised these into the following two categories: firstly, psychological variables measuring an individual’s response to change and stressors including adaptability, resilience, grit and emotional regulation [ 39 , 40 , 41 , 42 , 43 , 46 , 49 , 54 , 58 ] and secondly, those that measure self-esteem and body image [ 29 , 64 ].
The evidence from the eight included quantitative studies suggests that students with psychological strengths including; optimism, self-efficacy [ 70 ], resilience, grit [ 58 ], use of positive reappraisal [ 49 ], helpful coping strategies [ 42 ] and emotional intelligence [ 41 , 46 ] are more likely to experience greater mental wellbeing (see Table 2 for a description of the psychological variables measured). The positive association between these psychological strengths and mental well-being had a positive affect with associations ranging from r = 0.2–0.5 and OR1.27 [ 41 , 43 , 46 , 49 , 54 ] (low to moderate strength of association). The negative associations with depressive symptoms are also statistically significant but with a weaker association ( r = -0.2—0.3) [ 43 , 49 , 54 ].
Denovan (2017a) [ 43 ] in a longitudinal study found that the association between psychological strengths and positive mental wellbeing was not static and that not all the strengths remained statistically significant over time. The only factors that remained significant during the transition period were self-efficacy and optimism, remaining statistically significant as they started university and 6 months later.
Parental factors
Only one study [ 59 ] explored family factors associated with the development of psychological strengths that would equip young people as they managed the challenges and stressors encountered during the transition to higher education. Lloyd et al. (2014) [ 59 ] found that perceived maternal and paternal acceptance made significant and unique contributions to students’ psychological adjustment. Their research methods are limited by their reliance on retrospective measures and self-report measures of variables, and these results could be influenced by recall bias.
Two studies [ 29 , 64 ] considered the impact of how individuals view themselves on poor mental health. One study considered the impact of self-esteem and the association with non-accidental self-injury (NSSI) and suicide attempt amongst 734 university students. As rates of suicide and NSSI are higher amongst LGBT (lesbian, gay, bisexual, transgender) students, the prevalence of low self-esteem was compared. There was a low but statistically significant association between low self-esteem and NSSI, though not for suicide attempt. A large survey, including participants from seven universities [ 42 ] compared depressive symptoms in students with marked body image concerns, reporting that the risk of depressive symptoms was greater (OR 2.93) than for those with lower levels of body image concerns.
Mental health literacy and help seeking behaviour
Two studies [ 48 , 68 ] investigated attitudes to mental illness, mental health literacy and help seeking for mental health problems.
University students who lack sufficient mental health literacy skills to be able to recognise problems or where there are attitudes that foster shame at admitting to having mental health problems can result in students not recognising problems and/or failing to seek professional help [ 48 , 68 ]. Gorcyznski et al. (2017) [ 68 ] found that women and those who had a history of previous mental health problems exhibited significantly higher levels of mental health literacy. Greater mental health literacy was associated with an increased likelihood that individuals would seek help for mental health problems. They found that many students find it hard to identify symptoms of mental health problems and that 42% of students are unaware of where to access available resources. Of those who expressed an intention to seek help for mental health problems, most expressed a preference for online resources, and seeking help from family and friends, rather than medical professionals such as GPs.
Kotera et al. (2019) [ 48 ] identified self-compassion as an explanatory variable, reducing social comparison, promoting self-acceptance and recognition that discomfort is an inevitable human experience. The study found a strong, significant correlation between self-compassion and mental health symptoms ( r = -0.6. p < 0.01).
There again appears to be a cycle of reinforcement, where poor mental health symptoms are felt to be a source of shame and become hidden, help is not sought, and further isolation ensues, leading to further deterioration in mental health. Factors that can interrupt the cycle are self-compassion, leading to more readiness to seek help (see Fig. 2 ).

Poor mental health – cycles of reinforcement
Social networks
Nine studies [ 33 , 38 , 41 , 46 , 51 , 54 , 60 , 64 , 65 ] examined the concepts of loneliness and social support and its association with mental health in university students. One study also included students at other Higher Education Institutions [ 46 ]. Eight of the studies were surveys, and one was a retrospective case control study to examine the differences between university students and age-matched young people (non-university students) who attended hospital following deliberate self-harm [ 51 ].
Included studies demonstrated considerable variation in how they measured the concepts of social isolation, loneliness, social support and a sense of belonging. There were also differences in the types of outcomes measured to assess mental wellbeing and poor mental health. Grouping the studies within a broad category of ‘social factors’ therefore represents a limitation of this review given that different aspects of the phenomena may have been being measured. The tools used to measure these variables also differed. Only one scale (The UCLA loneliness scale) was used across multiple studies [ 41 , 60 , 65 ]. Diverse mental health outcomes were measured across the studies including positive affect, flourishing, self-harm, suicide risk, depression, anxiety and paranoia.
Three studies [ 41 , 60 , 62 ] measuring loneliness, two longitudinally [ 41 , 62 ], found a consistently positive association between loneliness and poor mental health in university students. Greater loneliness was linked to greater anxiety, stress, depression, poor general mental health, paranoia, alcohol abuse and eating disorder problems. The strength of the correlations ranged from 0–3-0.4 and were all statistically significant (see Tables 3 and 4 ). Loneliness was the strongest overall predictor of mental distress, of those measured. A strong identification with university friendship groups was most protective against distress relative to other social identities [ 60 ]. Whether poor mental health is the cause, or the result of loneliness was explored further in the studies. The results suggest that for general mental health, stress, depression and anxiety, loneliness induces or exacerbates symptoms of poor mental health over time [ 60 , 62 ]. The feedback cycle is evident, with loneliness leading to poor mental health which leads to withdrawal from social contacts and further exacerbation of loneliness.
Factors associated with protecting against loneliness by fostering supportive friendships and promoting mental wellbeing were also identified. Beliefs about the value of ‘leisure coping’, and attributes of resilience and emotional intelligence had a moderate, positive and significant association with developing mental wellbeing and were explored in three studies [ 46 , 54 , 66 ].
The transition to and first year at university represent critical times when friendships are developed. Thomas et al. (2020) [ 65 ] explored the factors that predict loneliness in the first year of university. A sense of community and higher levels of ‘social capital’ were significantly associated with lower levels of loneliness. ‘Social capital’ scales measure the development of emotionally supportive friendships and the ability to adjust to the disruption of old friendships as students transition to university. Students able to form close relationships within their first year at university are less likely to experience loneliness (r-0.09, r- 0.36, r- 0.34). One study [ 38 ] investigating the relationship between student experience and being the first in the family to attend university found that these students had lower ratings for peer group interactions.
Young adults at university and in higher education are facing multiple adjustments. Their ability to cope with these is influenced by many factors. Supportive friendships and a sense of belonging are factors that strengthen coping. Nightingale et al. (2012) undertook a longitudinal study to explore what factors were associated with university adjustment in a sample of first year students ( n = 331) [ 41 ]. They found that higher skills of emotion management and emotional self-efficacy were predictive of stable adjustment. These students also reported the lowest levels of loneliness and depression. This group had the skills to recognise their emotions and cope with stressors and were confident to access support. Students with poor emotion management and low levels of emotional self-efficacy may benefit from intervention to support the development of adaptive coping strategies and seeking support.
The positive and negative feedback loops
The relationship between the variables described appeared to work in positive and negative feedback loops with high levels of social capital easing the formation of a social network which acts as a critical buffer to stressors (see Fig. 3 ). Social networks and support give further strengthening and reinforcement, stimulating positive affect, engagement and flourishing. These, in turn, widen and deepen social networks for support and enhance a sense of wellbeing. Conversely young people who enter the transition to university/higher education with less social capital are less likely to identify with and locate a social network; isolation may follow, along with loneliness, anxiety, further withdrawal from contact with social networks and learning, and depression.

Triggers – factors that may act in combination with other factors to lead to poor mental health
Stress is seen as playing a key role in the development of poor mental health for students in higher education. Theoretical models and empirical studies have suggested that increases in stress are associated with decreases in student mental health [ 12 , 43 ]. Students at university experience the well-recognised stressors associated with academic study such as exams and course work. However, perhaps less well recognised are the processes of transition, requiring adapting to a new social and academic environment (Fisher 1994 cited by Denovan 2017a) [ 43 ]. Por et al. (2011) [ 46 ] in a small ( n = 130 prospective survey found a statistically significant correlation between higher levels of emotional intelligence and lower levels of perceived stress ( r = 0.40). Higher perceived stress was also associated with negative affect in two studies [ 43 , 46 ], and strongly negatively associated with positive affect (correlation -0.62) [ 54 ].
University variables
Eleven studies [ 35 , 39 , 47 , 51 , 52 , 54 , 60 , 63 , 65 , 83 , 84 ] explored university variables, and their association with mental health outcomes. The range of factors and their impact on mental health variables is limited, and there is little overlap. Knowledge gaps are shown by factors highlighted by our PPI group as potentially important but not identified in the literature (see Table 5 ). It should be noted that these may reflect the focus of our review, and our exclusion of intervention studies which may evaluate university factors.
High levels of perceived stress caused by exam and course work pressure was positively associated with poor mental health and lack of wellbeing [ 51 , 52 , 54 ]. Other potential stressors including financial anxieties and accommodation factors appeared to be less consistently associated with mental health outcomes [ 35 , 38 , 47 , 51 , 60 , 62 ]. Important mediators and buffers to these stressors are coping strategies and supportive networks (see conceptual model Appendix 2 ). One impact of financial pressures was that students who worked longer hours had less interaction with their peers, limiting the opportunities for these students to benefit from the protective effects of social support.
Red flags – behaviours associated with poor mental health and/or wellbeing
Engagement with learning and leisure activities.
Engagement with learning activities was strongly and positively associated with characteristics of adaptability [ 39 ] and also happiness and wellbeing [ 52 ] (see Fig. 4 ). Boulton et al. (2019) [ 52 ] undertook a longitudinal survey of undergraduate students at a campus-based university. They found that engagement and wellbeing varied during the term but were strongly correlated.

Engagement and wellbeing
Engagement occurred in a wide range of activities and behaviours. The authors suggest that the strong correlation between all forms of engagement with learning has possible instrumental value for the design of systems to monitor student engagement. Monitoring engagement might be used to identify changes in the behaviour of individuals to assist tutors in providing support and pastoral care. Students also were found to benefit from good induction activities provided by the university. Greater induction satisfaction was positively and strongly associated with a sense of community at university and with lower levels of loneliness [ 65 ].
The inte r- related nature of these variables is depicted in Fig. 4 . Greater adaptability is strongly associated with more positive engagement in learning and university life. More engagement is associated with higher mental wellbeing.
Denovan et al. (2017b) [ 54 ] explored leisure coping, its psychosocial functions and its relationship with mental wellbeing. An individual’s beliefs about the benefits of leisure activities to manage stress, facilitate the development of companionship and enhance mood were positively associated with flourishing and were negatively associated with perceived stress. Resilience was also measured. Resilience was strongly and positively associated with leisure coping beliefs and with indicators of mental wellbeing. The authors conclude that resilient individuals are more likely to use constructive means of coping (such as leisure coping) to proactively cultivate positive emotions which counteract the experience of stress and promote wellbeing. Leisure coping is predictive of positive affect which provides a strategy to reduce stress and sustain coping. The belief that friendships acquired through leisure provide social support is an example of leisure coping belief. Strong emotionally attached friendships that develop through participation in shared leisure pursuits are predictive of higher levels of well-being. Friendship bonds formed with fellow students at university are particularly important for maintaining mental health, and opportunities need to be developed and supported to ensure that meaningful social connections are made.
The ‘broaden-and-build theory’ (Fredickson 2004 [ 85 ] cited by [ 54 ]) may offer an explanation for the association seen between resilience, leisure coping and psychological wellbeing. The theory is based upon the role that positive and negative emotions have in shaping human adaptation. Positive emotions broaden thinking, enabling the individual to consider a range of ways of dealing with and adapting to their environment. Conversely, negative emotions narrow thinking and limit options for adapting. The former facilitates flourishing, facilitating future wellbeing. Resilient individuals are more likely to use constructive means of coping which generate positive emotion (Tugade & Fredrickson 2004 [ 86 ], cited by [ 54 ]). Positive emotions therefore lead to growth in coping resources, leading to greater well-being.
Health behaviours at university
Seven studies [ 29 , 31 , 38 , 45 , 51 , 54 , 66 ] examined how lifestyle behaviours might be linked with mental health outcomes. The studies looked at leisure activities [ 63 , 80 ], diet [ 29 ], alcohol use [ 29 , 31 , 38 , 51 ] and sleep [ 45 ].
Depressive symptoms were independently associated with problem drinking and possible alcohol dependence for both genders but were not associated with frequency of drinking and heavy episodic drinking. Students with higher levels of depressive symptoms reported significantly more problem drinking and possible alcohol dependence [ 31 ]. Mahadevan et al. (2010) [ 51 ] compared students and non-students seen in hospital for self-harm and found no difference in harmful use of alcohol and illicit drugs.
Poor sleep quality and increased consumption of unhealthy foods were also positively associated with depressive symptoms and perceived stress [ 29 ]. The correlation with dietary behaviours and poor mental health outcomes was low, but also confirmed by the negative correlation between less perceived stress and depressive symptoms and consumption of a healthier diet.
Physical activity and participation in leisure pursuits were both strongly correlated with mental wellbeing ( r = 0.4) [ 54 ], and negatively correlated with depressive symptoms and anxiety ( r = -0.6, -0.7) [ 66 ].
Thirty studies measuring the association between a wide range of factors and poor mental health and mental wellbeing in university and college students were identified and included in this review. Our purpose was to identify the factors that contribute to the growing prevalence of poor mental health amongst students in tertiary level education within the UK. We also aimed to identify factors that promote mental wellbeing and protect against deteriorating poor mental health.
Loneliness and social isolation were strongly associated with poor mental health and a sense of belonging and a strong support network were strongly associated with mental wellbeing and happiness. These associations were strongly positive in the eight studies that explored them and are consistent with other meta-analyses exploring the link between social support and mental health [ 87 ].
Another factor that appeared to be protective was older age when starting university. A wide range of personal traits and characteristics were also explored. Those associated with resilience, ability to adjust and better coping led to improved mental wellbeing. Better engagement appeared as an important mediator to potentially explain the relationship between these two variables. Engagement led to students being able to then tap into those features that are protective and promoting of mental wellbeing.
Other important risk factors for poor mental wellbeing that emerged were those students with existing or previous mental illness. Students on the autism spectrum and those with poor social problem-solving also were more likely to suffer from poor mental health. Negative self-image was also associated with poor mental health at university. Eating disorders were strongly associated with poor mental wellbeing and were found to be far more of a risk in students at university than in a comparative group of young people not in higher education. Other studies of university students also found that pre-existing poor mental health was a strong predictor of poor mental health in university students [ 88 ].
At a family level, the experience of childhood trauma and adverse experiences including, for example, neglect, household dysfunction or abuse, were strongly associated with poor mental health in young people at university. Students with a greater number of ‘adverse childhood experiences’ were at significantly greater risk of poor mental health than those students without experience of childhood trauma. This was also identified in a review of factors associated with depression and suicide related outcomes amongst university undergraduate students [ 88 ].
Our findings, in contrast to findings from other studies of university students, did not find that female gender associated with poor mental health and wellbeing, and it also found that being a mature student was protective of mental wellbeing.
Exam and course work pressure was associated with perceived stress and poor mental health. A lack of engagement with learning activities was also associated with poor mental health. A number of variables were not consistently shown to be associated with poor mental health including financial concerns and accommodation factors. Very little evidence related to university organisation or support structures was assessed in the evidence. One study found that a good induction programme had benefits for student mental wellbeing and may be a factor that enables students to become a part of a social network positive reinforcement cycle. Involvement in leisure activities was also found to be associated with improved coping strategies and better mental wellbeing. Students with poorer mental health tended to also eat in a less healthy manner, consume more harmful levels of alcohol, and experience poorer sleep.
This evidence review of the factors that influence mental health and wellbeing indicate areas where universities and higher education settings could develop and evaluate innovations in practice. These include:
Interventions before university to improve preparation of young people and their families for the transition to university.
Exploratory work to identify the acceptability and feasibility of identifying students at risk or who many be exhibiting indications of deteriorating mental health
Interventions that set out to foster a sense of belonging and identify
Creating environments that are helpful for building social networks
Improving mental health literacy and access to high quality support services
This review has a number of limitations. Most of the included studies were cross-sectional in design, with a small number being longitudinal ( n = 7), following students over a period of time to observe changes in the outcomes being measured. Two limitations of these sources of data is that they help to understand associations but do not reveal causality; secondly, we can only report the findings for those variables that were measured, and we therefore have to support causation in assuming these are the only factors that are related to mental health.
Furthermore, our approach has segregated and categorised variables in order to better understand the extent to which they impact mental health. This approach does not sufficiently explore or reveal the extent to which variables may compound one another, for example, feeling the stress of new ways of learning may not be a factor that influences mental health until it is combined with a sense of loneliness, anxiety about financial debt and a lack of parental support. We have used our PPI group and the development of vignettes of their experiences to seek to illustrate the compounding nature of the variables identified.
We limited our inclusion criteria to studies undertaken in the UK and published within the last decade (2009–2020), again meaning we may have limited our inclusion of relevant data. We also undertook single data extraction of data which may increase the risk of error in our data.
Understanding factors that influence students’ mental health and wellbeing offers the potential to find ways to identify strategies that enhance the students’ abilities to cope with the challenges of higher education. This review revealed a wide range of variables and the mechanisms that may explain how they impact upon mental wellbeing and increase the risk of poor mental health amongst students. It also identified a need for interventions that are implemented before young people make the transition to higher education. We both identified young people who are particularly vulnerable and the factors that arise that exacerbate poor mental health. We highlight that a sense of belonging and supportive networks are important buffers and that there are indicators including lack of engagement that may enable early intervention to provide targeted and appropriate support.
Availability of data and materials
Further details of the study and the findings can be provided on request to the lead author ([email protected]).
Association of Colleges. Association of Colleges’ survey on students with mental health conditions in further education. London: 2017.
Google Scholar
Hughes G, Spanner L. The University Mental Health Charter. Leeds: Student Minds; 2019.
Sivertsen B, Hysing M, Knapstad M, Harvey AG, Reneflot A, Lønning KJ, et al. Suicide attempts and non-suicidal self-harm among university students: prevalence study. BJPsych Open. 2019;5(2):e26.
Article PubMed PubMed Central Google Scholar
Storrie K, Ahern K, Tuckett A. A systematic review: students with mental health problems—a growing problem. Int J Nurs Pract. 2010;16(1):1–6.
Article PubMed Google Scholar
Pereira S, Reay K, Bottell J, Walker L, Dzikiti C, Platt C, Goodrham C. Student Mental Health Survey 2018: A large scale study into the prevalence of student mental illness within UK universities. 2019.
Bayram N, Bilgel N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc Psychiatry Psychiatr Epidemiol. 2008;43(8):667–72.
Bewick B, Koutsopoulou G, Miles J, Slaa E, Barkham M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud High Educ. 2010;35(6):633–45.
Article Google Scholar
Thorley C. Not By Degrees: Not by degrees: Improving student mental health in the UK’s universities. London: IPPR; 2017.
Eisenberg D, Golberstein E, Hunt JB. Mental health and academic success in college. BE J Econ Anal Pol. 2009;9(1):1–37.
Hysenbegasi A, Hass SL, Rowland CR. The impact of depression on the academic productivity of university students. J Ment Health Policy Econ. 2005;8(3):145.
PubMed Google Scholar
Chowdry H, Crawford C, Dearden L, Goodman A, Vignoles A. Widening participation in higher education: analysis using linked administrative data. J R Stat Soc A Stat Soc. 2013;176(2):431–57.
Macaskill A. The mental health of university students in the United Kingdom. Br J Guid Couns. 2013;41(4):426–41.
Belfield C, Britton J, van der Erve L. Higher Education finance reform: Raising the repayment threshold to£ 25,000 and freezing the fee cap at £ 9,250: Institute for Fiscal Studies Briefing note. London: Institute for Fiscal Studies; 2017. Available from https://ifs.org.uk/publications/9964 .
Benson-Egglenton J. The financial circumstances associated with high and low wellbeing in undergraduate students: a case study of an English Russell Group institution. J Furth High Educ. 2019;43(7):901–13.
Jessop DC, Herberts C, Solomon L. The impact of financial circumstances on student health. Br J Health Psychol. 2005;10(3):421–39.
(2020) SCSC. Canadians’ mental health during the COVID-19 pandemic. 2020.
(NUS) NUoS. Coronavirus Student Survey phase III November 2020. 2020.
Hellemans K, Abizaid A, Gabrys R, McQuaid R, Patterson Z. For university students, COVID-19 stress creates perfect conditions for mental health crises. The Conversation. 2020. Available from: https://theconversation.com/for-university-students-covid-19-stress-creates-perfect-conditions-for-mental-health-crises-149127 .
England N. Children and Young People with an Eating Disorder Waiting Times: NHS England; 2021 [Available from: https://www.england.nhs.uk/statistics/statistical-work-areas/cyped-waiting-times/
King JA, Cabarkapa S, Leow FH, Ng CH. Addressing international student mental health during COVID-19: an imperative overdue. Australas Psychiatry. 2020;28(4):469.
Rana R, Smith E, Walking J. Degrees of disturbance: the new agenda; the Impact of Increasing Levels of Psychological Disturbance Amongst Students in Higher Education. England: Association for University and College Counselling Rugby; 1999.
AMOSSHE. Responding to student mental health issues: 'Duty of Care' responsibilities for student services in higher education. https://www.amosshe.org.uk/resources/Documents/AMOSSHE_Duty_of_Care_2001.pdf [accessed 24.12.2020]. (2001).
Universities UK. Student mental wellbeing in higher education. Good practice guide. London: Universities UK; 2015.
Williams M, Coare P, Marvell R, Pollard E, Houghton A-M, Anderson J. 2015. Understanding provision for students with mental health problems and intensive support needs: Report to HEFCE by the Institute for Employment Studies (IES) and Researching Equity, Access and Partnership (REAP). Institute for Employment Studies.
Hunt J, Eisenberg D. Mental health problems and help-seeking behavior among college students. J Adolesc Health. 2010;46(1):3–10.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. In.: Oxford; 2000.
Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890.
El Ansari W, Adetunji H, Oskrochi R. Food and mental health: relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent Eur J Public Health. 2014a;22(2):90–7.
El Ansari W, Dibba E, Stock C. Body image concerns: levels, correlates and gender differences among students in the United Kingdom. Cent Eur J Public Health. 2014b;22(2):106–17.
Ansari EL, W, Oskrochi R, Stock C. Symptoms and health complaints and their association with perceived stress: Students from seven universities in England, Wales and Northern Ireland. J Public Health. 2013;21(5):413–25.
El Ansari W, Sebena R, Stock C. Do importance of religious faith and healthy lifestyle modify the relationships between depressive symptoms and four indicators of alcohol consumption? A survey of students across seven universities in England, Wales, and Northern Ireland. Subst Use Misuse. 2014c;49(3):211–20.
El Ansari W, Stock C. Is the health and wellbeing of university students associated with their academic performance? Cross sectional findings from the United Kingdom. International Journal of Environmental Research & Public Health [Electronic Resource]. 2010;7(2):509–27.
Gnan GH, Rahman Q, Ussher G, Baker D, West E, Rimes KA. General and LGBTQ-specific factors associated with mental health and suicide risk among LGBTQ students. J Youth Stud. 2019;22(10):1393–408.
Jackson SL, Dritschel B. Modeling the impact of social problem-solving deficits on depressive vulnerability in the broader autism phenotype. Res Aut Spectr Disord. 2016;21:128–38.
Richardson T, Elliott P, Roberts R. The impact of tuition fees amount on mental health over time in British students. J Public Health. 2015;37(3):412–8.
Article CAS Google Scholar
Richardson T, Mma Y, Jansen M, Elliott P, Roberts R. Financial difficulties and psychosis risk in British undergraduate students: a longitudinal analysis. J Public Ment Health. 2018;17(2):61–8.
Thomas L, Briggs P, Hart A, Kerrigan F. Understanding social media and identity work in young people transitioning to university. Comput Hum Behav. 2017;76:541–53.
Hixenbaugh P, Dewart H, Towell T. What enables students to succeed? An investigation of socio-demographic, health and student experience variables. Psychodyn Pract. 2012;18(3):285–301.
Holliman A, Martin A, Collie R. Adaptability, engagement, and degree completion: a longitudinal investigation of university students. Educ Psychol. 2018;38(6):785–99.
McLafferty M, Armour C, Bunting B, Ennis E, Lapsley C, Murray E, et al. Coping, stress, and negative childhood experiences: the link to psychopathology, self-harm, and suicidal behavior. Psychic J. 2019;8(3):293–306.
Nightingale S, Roberts S, Tariq V, Appleby Y, Barnes L, Harris R, et al. Trajectories of university adjustment in the United Kingdom: EMOTION management and emotional self-efficacy protect against initial poor adjustment. Learn Individ Differ. 2013;27:174–81.
Berry K, Kingswell S. An investigation of adult attachment and coping with exam-related stress. Br J Guid Couns. 2012;40(4):315.
Denovan A, Macaskill A. Stress and subjective well-being among first year UK undergraduate students. J Happiness Stud. 2017a;18(2):505–25.
Hassel S, Ridout N. An investigation of first-year students’ and lecturers’ expectations of university education. Front Psychol. 2018;8:2218.
Norbury R, Evans S. Time to think: subjective sleep quality, trait anxiety and university start time. Psychiatry Res. 2019;271:214–9.
Por J, Barriball L, Fitzpatrick J, Roberts J. Emotional intelligence: its relationship to stress, coping, well-being and professional performance in nursing students. Nurse Educ Today. 2011;31(8):855.
Honney K, Buszewicz M, Coppola W, Griffin M. Comparison of levels of depression in medical and non-medical students. Clin Teach. 2010;7(3):180–4.
Kotera Y, Conway E, Van Gordon W. Mental health of UK university business students: Relationship with shame, motivation and self-compassion. Journal of Education for Business. 2019;94(1):11–20.
Oliver EJ, Markland D, Hardy J. Interpretation of self-talk and post-lecture affective states of higher education students: a self-determination theory perspective. Br J Educ Psychol. 2010;80(Pt 2):307–23.
O’Neill S, McLafferty M, Ennis E, Lapsley C, Bjourson T, Armour C, et al. Socio-demographic, mental health and childhood adversity risk factors for self-harm and suicidal behaviour in College students in Northern Ireland. J Affect Disord. 2018;239:58–65.
Mahadevan S, Hawton K, Casey D. Deliberate self-harm in Oxford University students, 1993–2005: a descriptive and case-control study. Soc Psychiatry Psychiatr Epidemiol. 2010;45(2):211–9.
Boulton CA, Hughes E, Kent C, Smith JR, Williams HTP. Student engagement and wellbeing over time at a higher education institution. PLoS One [Electronic Resource]. 2019;14(11): e0225770.
Davies EL, Paltoglou AE. Public self-consciousness, pre-loading and drinking harms among university students. Subst Use Misuse. 2019;54(5):747–57.
Denovan A, Macaskill A. Stress, resilience and leisure coping among university students: Applying the broaden-and-build theory. Leisure Studies. 2017b;36(6):852–65.
El Ansari W, Vallentin-Holbech L, Stock C. Predictors of illicit drug/s use among university students in Northern Ireland, Wales and England. Glob J Health Sci. 2015;7(4):18–29.
Freeth M, Bullock T, Milne E. The distribution of and relationship between autistic traits and social anxiety in a UK student population. Autism. 2013;17(5):571–81.
Jessop DC, Reid M, Solomon L. Financial concern predicts deteriorations in mental and physical health among university students. Psychology Health. 2020;35(2):196–209.
Kannangara CS, Allen RE, Waugh G, Nahar N, Khan SZN, Rogerson S, Carson J. All that glitters is not grit: Three studies of grit in university students. Front Psychol. 2018;9:1539.
Lloyd J, Ward T, Young J. Do parental interpersonal power and prestige moderate the relationship between parental acceptance and psychological adjustment in U.K. Students? Cross-Cultural Research. The Journal of Comparative Social Science. 2014;48(3):326–35.
McIntyre JC, Worsley J, Corcoran R, Harrison Woods P, Bentall RP. Academic and non-academic predictors of student psychological distress: the role of social identity and loneliness. J Ment Health. 2018;27(3):230–9.
Ribchester C, Ross K, Rees EL. Examining the impact of pre-induction social networking on the student transition into higher education. Innov Educ Teach Int. 2014;51(4):355–65.
Richardson T, Elliott P, Roberts R. Relationship between loneliness and mental health in students. J Public Ment Health. 2017a;16(2):48–54.
Richardson T, Elliott P, Roberts R, Jansen M. A Longitudinal Study of Financial Difficulties and Mental Health in a National Sample of British Undergraduate Students. Community Ment Health J. 2017;53(3):344–52.
Taylor PJ, Dhingra K, Dickson JM, McDermott E. Psychological Correlates of Self-Harm within Gay, Lesbian and Bisexual UK University Students. Arch Suicide Res. 2020;24(sup1):41–56.
Thomas L, Orme E, Kerrigan F. Student loneliness: The role of social media through life transitions. Comput Educ. 2020;146:103754.
Tyson P, Wilson K, Crone D, Brailsford R, Laws K. Physical activity and mental health in a student population. J Ment Health. 2010;19(6):492–9.
Folkman S. The Oxford handbook of stress, health, and coping. Oxford: Oxford University Press; 2011.
Gorczynski P, Sims-schouten W, Hill D, Wilson JC. Examining mental health literacy, help seeking behaviours, and mental health outcomes in UK university students. J Ment Health Train Educ Pract. 2017;12(2):111–20.
Felitti VJ. Adverse childhood experiences and adult health. Acad Pediatr. 2009;9(3):131–2.
Denovan A, Macaskill A. An interpretative phenomenological analysis of stress and coping in first year undergraduates. Br Educ Res J. 2013;39(6):1002–24.
Bandura A. Self-efficacy: The foundation of agency. Control of human behavior, mental processes, and consciousness: Essays in honor of the 60th birthday of August Flammer. 2000;16.
Martin AJ, Nejad H, Colmar S, Liem GAD. Adaptability: Conceptual and empirical perspectives on responses to change, novelty and uncertainty. J Psychol Couns Sch. 2012;22(1):58–81.
Lazarus RS, Folkman S. Stress, appraisal, and coping: Springer publishing company; 1984.
Gross JJ. Emotion regulation: Past, present, future. Cogn Emot. 1999;13(5):551–73.
Mayer JD, Salovey P, Caruso DR. TARGET ARTICLES:" Emotional Intelligence: Theory, Findings, and Implications". Psychol Inq. 2004;15(3):197–215.
Duckworth AL, Peterson C, Matthews MD, Kelly DR. Grit: perseverance and passion for long-term goals. J Pers Soc Psychol. 2007;92(6):1087.
Snyder CR, Ilardi SS, Cheavens J, Michael ST, Yamhure L, Sympson S. The role of hope in cognitive-behavior therapies. Cognit Ther Res. 2000;24(6):747–62.
Scheier MF, Carver CS, Bridges MW. Optimism, pessimism, and psychological well-being. 2001.
Seligman ME. Positive psychology in practice: Wiley; 2012.
Masten AS. Ordinary magic: Lessons from research on resilience in human development. Education Canada. 2009;49(3):28–32.
Rosenberg M, Schooler C, Schoenbach C, Rosenberg F. Global self-esteem and specific self-esteem: Different concepts, different outcomes. Am Sociol Rev. 1995:141–56.
Oliver EJ, Markland D, Hardy J. Interpretation of self-talk and post-lecture affective states of higher education students: A self-determination theory perspective. Br J Educ Psychol. 2010;80(2):307–23.
Hofmann W, Friese M, Strack F. Impulse and self-control from a dual-systems perspective. Perspect Psychol Sci. 2009;4(2):162–76.
Aceijas C, Waldhausl S, Lambert N, Cassar S, Bello-Corassa R. Determinants of health-related lifestyles among university students. Perspect Public Health. 2017;137(4):227–36.
Fredrickson BL. The broaden–and–build theory of positive emotions. Philos Trans R Soc Lond B Biol Sci. 2004;359(1449):1367–77.
Tugade MM, Fredrickson BL, Feldman Barrett L. Psychological resilience and positive emotional granularity: Examining the benefits of positive emotions on coping and health. J Pers. 2004;72(6):1161–90.
Harandi TF, Taghinasab MM, Nayeri TD. The correlation of social support with mental health: A meta-analysis. Electron physician. 2017;9(9):5212.
Sheldon E, Simmonds-Buckley M, Bone C, Mascarenhas T, Chan N, Wincott M, Gleeson H, Sow K, Hind D, Barkham M. Prevalence and risk factors for mental health problems in university undergraduate students: A systematic review with meta-analysis. J Affect Disord. 2021;287:282–92.
Download references
Acknowledgements
We acknowledge the input from our public advisory group which included current and former students, and family members of students who have struggled with their mental health. The group gave us their extremely valuable insights to assist our understanding of the evidence.
This project was supported by funding from the National Institute for Health Research as part of the NIHR Public Health Research Programme (fuding reference 127659 Public Health Review Team). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Author information
Authors and affiliations.
University of Sheffield, Sheffield, UK
Fiona Campbell, Lindsay Blank, Anna Cantrell, Susan Baxter, Christopher Blackmore, Jan Dixon & Elizabeth Goyder
You can also search for this author in PubMed Google Scholar
Contributions
All of the included authors designed the project methods and prepared a protocol. A.C. designed the search strategy. F.C, L.B and C.B screened the identified citations and undertook data extraction. S.B. led the PPI involvement. JD participated as a member of the PPI group. F.C and L.B undertook the analysis. F.C. and L.B wrote the main manuscript text. All authors reviewed the manuscript. F.C designed Figs. 2 , 3 and 4 . The author(s) read and approved the final manuscript.
Corresponding author
Correspondence to Fiona Campbell .
Ethics declarations
Ethics approval and consent to participate.
Not applicable as this was secondary research.
Consent for publication
Not applicable.
Competing interests
None of the authors have competing interests or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1., additional file 2., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Campbell, F., Blank, L., Cantrell, A. et al. Factors that influence mental health of university and college students in the UK: a systematic review. BMC Public Health 22 , 1778 (2022). https://doi.org/10.1186/s12889-022-13943-x
Download citation
Received : 03 February 2022
Accepted : 25 July 2022
Published : 20 September 2022
DOI : https://doi.org/10.1186/s12889-022-13943-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Student mental health
- Mental wellbeing
- Risk factors
- Rapid review
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]
Balancing Work, School, and Personal Life among Graduate Students: a Positive Psychology Approach
- Published: 24 July 2018
- Volume 14 , pages 1265–1286, ( 2019 )
Cite this article

- Jessica M. Nicklin 1 ,
- Emily J. Meachon 1 &
- Laurel A. McNall 2
7028 Accesses
22 Citations
1 Altmetric
Explore all metrics
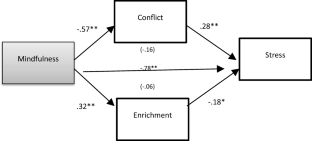
Graduate students are faced with an array of responsibilities in their personal and professional lives, yet little research has explored how working students maintain a sense of well-being while managing work, school, and personal-life. Drawing on conservation of resources theory and work-family enrichment theory, we explored personal, psychological resources that increase enrichment and decrease conflict, and in turn decrease perceptions of stress. In a study of 231 employed graduate students, we found that mindfulness was negatively related to stress via perceptions of conflict and enrichment, whereas self-compassion, resilience, and recovery experience were negatively related to stress, but only through conflict, not enrichment. These findings suggest that graduate students who are able to be “in the moment” may experience higher levels of well-being, in part due to greater enrichment and lower conflict.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

Exploring How Mindfulness Links to Work Outcomes: Positive Affectivity and Work-Life Enrichment

Study Demands–Resources Theory: Understanding Student Well-Being in Higher Education
Examining ways that a mindfulness-based intervention reduces stress in public school teachers: a mixed-methods study.
Allen, T. D., & Kiburtz, K. M. (2012). Trait mindfulness and work-family balance among working parents: The mediating effects of vitality and sleep quality. Journal of Vocational Behavior, 80 , 372–379. https://doi.org/10.1016/j.jvb.2011.09.002 .
Article Google Scholar
Allen, T. D., & Paddock, E. L. (2015). How being mindful impacts individuals' work-family balance, conflict, and enrichment: A review of existing evidence, mechanisms and future directions. In J. Reb, P. B. Atkins, J. Reb, & P. B. Atkins (Eds.), Mindfulness in organizations: Foundations, research, and applications (pp. 213–238). New York: Cambridge University Press.
Chapter Google Scholar
Amstad, F. T., Meier, L. L., Fasel, U., Elfering, A., & Semmer, N. K. (2011). A meta-analysis of work–family conflict and various outcomes with a special emphasis on cross-domain versus matching-domain relations. Journal of Occupational Health Psychology, 16 (2), 151–169 http://psycnet.apa.org/doi/10.1037/a0022170 .
Baghurst, T., & Kelley, B. C. (2014). An examination of stress in college students over the course of a semester. Health Promotion Practice, 15 (3), 438–447. https://doi.org/10.1177/1524839913510316 .
Baron, R. M. & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology, 51 (6), 1173–1182.
Blau, P. M. (1964). Exchange and power in social life . New York: Wiley.
Google Scholar
Bonifas, R. P., & Napoli, M. (2013). Mindfully increasing quality of life: A promising curriculum for MSW students. Social Work Education, 33 , 469–484. https://doi.org/10.1080/02615479.2013.838215 .
Braunstein-Bercovitz, H., Frish-Burstein, S., & Benjamin, B. A. (2012). The role of personal resources in work–family conflict: Implications for young mothers' well-being. Journal of Vocational Behavior, 80 (2), 317–325. https://doi.org/10.1016/j.jvb.2011.10.003 .
Britt, T. W., Shen, W., Sinclair, R. R., Grossman, M. R., & Klieger, D. M. (2016). How much do we really know about employee resilience? Industrial and Organizational Psychology, 9 (2), 378–404. https://doi.org/10.1017/iop.2016.36 .
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84 , 822–848. https://doi.org/10.1037/0022-3514.84.4.822 .
Carley-Baxter, L. R., Hill, C. A., Roe, D. J., Twiddy, S. E., Baxter, R. K., & Ruppenkamp, J. (2009). Does response rate matter? Journal editors use of survey quality measures in manuscript publication decisions. Survey Practice, 2 (7), 1–7.
Carlson, L. E., & Brown, K. W. (2005). Validation of the mindful attention awareness scale in a cancer population. Journal of Psychosomatic Research, 58 , 29–33. https://doi.org/10.1016/j.jpsychores.2004.04.366 .
Carlson, D. S., Kacmar, K. M., Wayne, J. H., Grzywacz, J. G. (2006). Measuring the positive side of the work–family interface: Development and validation of a work–family enrichment scale. Journal of Vocational Behavior, 68 (1), 131–164. https://doi.org/10.1016/j.jvb.2005.02.002 .
Cheng, B. H., & McCarthy, J. M. (2013). Managing work, family, and school roles: Disengagement strategies can help and hinder. Journal of Occupational Health Psychology, 18 , 241–251. https://doi.org/10.1037/a0032507 .
Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18 (2), 76–82.
Council of Graduate Schools. Graduate Schools Report Strong Growth In First-Time Enrollment Of Underrepresented Minorities . 2016. Print.
Creed, P. A., French, J., & Hood, M. (2015). Working while studying at university: The relationship between work benefits and demands and engagement and well-being. Journal of Vocational Behavior, 86 , 48–57. https://doi.org/10.1016/j.jvb.2014.11.002 .
Davis, J. (2012). School enrollment and work status: 2011. United States Census Bureau. Retrieved from: https://www.census.gov/prod/2013pubs/acsbr11-14.pdf .
Ditto, B., Eclache, M., & Goldman, N. (2006). Short-term autonomic and cardiovascular effects of mindfulness body scan meditation. Annals of Behavioral Medicine, 32 (3), 227–234. https://doi.org/10.1207/s15324796abm3203_9 .
Dyrbye, L. N., Power, D. V., Massie, F. S., et al. (2010). Factors associated with resilience to and recovery from burnout: A prospective, multi-institutional study of US medical students. Medical Education, 44 , 1016–1026. https://doi.org/10.1111/j.1365-2923.2010.03754.x .
Etzion, D., Eden, D., & Lapidot, Y. (1998). Relief from job stressors and burnout: Reserve service as a respite. Journal of Applied Psychology, 83 , 377–585.
Evans, T. M., Bira, L., Gastelum, J. B., Weiss, T. L., & Vanderford, N. L. (2018). Evidence for a mental health crisis in graduate education. Nature Biotechnology, 36 , 282–284. https://doi.org/10.1038/nbt.4089 .
Flavin, C. & Swody, C. (2016). LeaderMoms use self-compassion as antidote to unproductive guilt. Tech report. Thrive Leadership.
Fredrickson, B. L. (2004). The broaden-and-build theory of positive emotions. Philosophical Transactions of the Royal Society B: Biological Sciences, 359 (1449), 1367–1378. https://doi.org/10.1098/rstb.2004.1512 .
Gable, S. L., & Haidt, J. (2005). What (and why) is positive psychology? Review of General Psychology, 9 (2), 103–110. https://doi.org/10.1037/1089-2680.9.2.103 .
Gilbert, P. (2005). Compassion and cruelty: A biopsychosocial approach. In P. Gilbert (Ed.), Compassion: Conceptualisations, research and use in psychotherapy (pp. 9–74). London: Routledge.
Goewey, (2015). Generation stress. The Huffington Post. Retrieved From: http://www.huffingtonpost.com/don-joseph-goewey-/generation-stress_b_8062346.html .
Greenhaus, J. H., & Parasuraman, S. (1999). Research on work, family, and gender: Current status and future directions. In G. N. Powell (Ed.), Handbook of Gender & Work (pp. 391–412). Thousand Oaks: Sage Publications.
Greenhaus, J. H., & Powell, G. N. (2006). When work and family are allies: A theory of work-family enrichment. Academy of Management Review, 31 , 72–92. https://doi.org/10.1016/j.jvb.2005.02.002 .
Greeson, J. M., Juberg, M. K., Maytan, M., James, K., & Rogers, H. (2014). A randomized controlled trial of KORU: A mindfulness program for college students and other emerging adults. Journal of American College Health, 64 (4), 222–233. https://doi.org/10.1080/07448481.2014.887571 .
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57 , 35–43. https://doi.org/10.1016/S0022-3999(03)00573-7 .
Hahn, V. C., Binnewies, C., Sonnentag, S., & Mojza, E. J. (2011). Learning how to recover from job stress: Effects of a recovery training program on recovery, recovery-related self-efficacy, and well-being. Journal of Occupational Health Psychology, 16 (2), 202–216. https://doi.org/10.1037/a0022169 .
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach . New York: Guilford Press.
Hayes, A. F. (2016). Partial, conditional, and moderated mediation: Quantification, inference and interpretation . Retrieved from http://afhayes.com/public/pmm2016.pdf .
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44 (3), 513–524. https://doi.org/10.1037/0003-066X.44.3.513 .
Hobfoll, S. E. (2002). Social and psychological resources and adaptation. Review of General Psychology, 6 , 307–324. https://doi.org/10.1037/1089-2680.6.4.307 .
Hoffman, J. (2015). Anxiety on campuses: Reporter’s notebook. The New York Times . Retrieved from: https://www.nytimes.com/times-insider/2015/05/28/anxiety-on-campus-reporters-notebook/ .
Holland, K. (2014). Back to school: Older students on the rise in college classrooms. Nbcnews.com . Retrieved from: http://www.nbcnews.com/business/business-news/back-school-older-students-rise-college-classrooms-n191246 .
Kabat-Zinn. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness . New York: Bantam Dell.
Kadziolka, M. J., Di Pierdomenico, E., & Miller, C. J. (2016). Trait-like mindfulness promotes healthy self-regulation of stress. Mindfulness, 7 (1), 236–245. https://doi.org/10.1007/s12671-015-0437-0 .
Karatepe, O. M., & Karadas, G. (2014). The effect of psychological capital on conflicts in the work-family interface, turnover and absence intentions. International Journal of Hospitality Management, 43 , 132–143.
Kiburz, K.M., & Allen, T.D. (2012). Dispositional mindfulness as a unique predictor of work-family conflict . Paper presented at the 27th annual Conference of the Society for Industrial and Organizational Psychology, April 2012, San Diego, CA.
Kiburz, K.M., & Allen, T.D. (2014). Examining the effects of mindfulness based work-family interventions. In J.G. Randall and M. Beier (Co-chairs), in MindWandering and Mindfulness: Self-regulation at Work. Symposium presented at the 29 th Annual conference of the Society for Industrial and Organizational Psychology, May 2014, Honolulu, HI.
King, J. (2006). Working their way through college: Student employment and its impact on the college experience. ACE Issue Brief. Retrieved from: http://www.acenet.edu/news-room/Documents/IssueBrief-2006-Working-their-way-through-College.pdf .
Krisor, S. M., Diebig, M., & Rowold, J. (2015). Is cortisol as a biomarker of stress influenced by the interplay of work-family conflict, work-family balance and resilience? Personnel Review, 44 (4), 648–661.
Kruger, S., & Sonoro, E. (2016). Physical activity and psychosomatic-related health problems as correlates of quality of life among university students. Journal of Psychology in Africa, 26 , 357–326. https://doi.org/10.1080/14330237.2016.1185907 1-6.
Kunz-Ebrecht, S. R., Kirschbaum, C., Marmot, M., & Steptoe, A. (2004). Differences in cortisol awakening response on work days and weekends in women and men from the Whitehall II cohort. Physchoneuroendocrinology, 29 , 516–528.
Lemyre, L., & Tessier, R. (2003). Measuring psychological stress. Concept, model, and measurement instrument in primary care research. Canadian Family Physician Medecin De Famille Canadien, 49 , 1159–1160.
Li, M. (2008). Relationships among stress coping, secure attachment, and the trait of resilience among Taiwanese college students. College Student Journal, 42 (2), 312–325.
Lundberg, U., & Frankenhaeuser, M. (1999). Stress and workload of men and women in high-ranking positions. Journal of Occupational Health Psychology, 4 , 142–151. https://doi.org/10.1037/1076-8998.4.2.142 .
Luthans, F., Avolio, B. J., Avey, J. B., & Norman, S. M. (2007). Psychological capital: Measurement and relationship with performance and job satisfaction. Personnel Psychology, 60 , 541–572. https://doi.org/10.1111/j.1744-6570.2007.00083.x .
Mallya, S., & Fiocco, A. J. (2016). Effects of mindfulness training on cognition and well-being in healthy older adults. Mindfulness, 7 (2), 453–465. https://doi.org/10.1007/s12671-015-0468-6 .
Markel, K. S., & Frone, M. R. (1998). Job characteristics, work-school conflict, and school outcomes among adolescents: Testing a structural model. Journal of Applied Psychology, 83 , 277–287.
Marks, S. R. (1977). Multiple roles and role strain: Some notes on human energy, time and commitment. American Sociological Review, 41 , 921–993.
McNall, L. A., & Michel, J. S. (2011). A dispositional approach to work–school conflict and enrichment. Journal of Business and Psychology, 26 (3), 397–411. https://doi.org/10.1007/s10869-010-9187-0 .
McNall, L. A., & Michel, J. S. (2017). The relationship between student core self-evaluations, support for school, and the work–school interface. Community, Work & Family, 20 , 253–272. https://doi.org/10.1080/13668803.2016.1249827 .
McNall, L. A., Nicklin, J. M., & Masuda, A. (2010). A meta- analytic review of the consequences associated with work- family enrichment. Journal of Business and Psychology, 25 , 381–396. https://doi.org/10.1007/s10869-009-9141-1 .
Michel, A., Bosch, C., & Rexroth, M. (2014). Mindfulness as a cognitive–emotional segmentation strategy: An intervention promoting work–life balance. Journal of Occupational and Organizational Psychology, 87 (4), 733–754. https://doi.org/10.1111/joop.12072 .
Moreno-Jiménez, B., Mayo, M., Sanz-Vergel, A. I., Geurts, S., Rodríguez-Muñoz, A., & Garrosa, E. (2009). Effects of work–family conflict on employees’ well-being: The moderating role of recovery strategies. Journal of Occupational Health Psychology, 14 (4), 427–440. https://doi.org/10.1037/a0016739 .
Mosewich, A. D., Kowalski, K. C., Sabiston, C. M., Sedgwick, W. A., & Tracy, J. L. (2011). Self-compassion: A potential resource for young women athletes. Journal of Sport & Exercise Psychology, 33 (1), 103–123.
National Center for Education Statistics (2017). Postbaccalaureate Enrollment. Retrieved from https://nces.ed.gov/programs/coe/indicator_chb.asp .
Neely, M. E., Schallert, D. L., Mohammed, S. S., Roberts, R. M., & Chen, Y. (2009). Self-kindness when facing stress: The role of self-compassion, goal regulation, and support in college students’ well-being. Motivation and Emotion, 33 , 88–97. https://doi.org/10.1007/s11031-008-9119-8 .
Neff, K. D. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2 , 85–102. https://doi.org/10.1080/15298860390129863 .
Neff, K., & Germer, C. (2013). Being kind to yourself: The science of self-compassion. In T. Singer & M. Bolz (Eds.), Compassion: Bridging theory and practice: A multimedia book (pp. 291–312). Leipzig: Max-Planck Institute.
Neff, K. D., & McGehee, P. (2009). Self-compassion and psychological resilience among adolescents and young adults. Self and Identity, 9 (3), 226–240 http://www.tandfonline.com/doi/abs/10.1080/15298860902979307 .
Neff, K. D., Kirkpatrick, K. L., & Rude, S. S. (2007). Self-compassion and adaptive psychological functioning. Journal of Research in Personality, 41 , 139–154. https://doi.org/10.1016/j.jrp.2006.03.004 .
Netemeyer, R. G., Boles, J. S., & Mcmurrian, R. (1996). Development and validation of work-family conflict and family-work conflict scales. Journal of Applied Psychology, 81 (4), 400–410. https://doi.org/10.1037/0021-9010.81.4.400 .
Nicklin, J. M., & McNall, L. A. (2013). Work–family enrichment, support, and satisfaction: A test of mediation. European Journal of Work and Organizational Psychology, 22 (1), 67–77. https://doi.org/10.1080/1359432X.2011.616652 .
Nicklin, J. M., McNall, L. A., & Janssen, A. (2018). An examination of positive psychological resources for promoting work-life balance. In J. M. Nicklin (Ed.), Work-family balance in the 21 st century . New York: Nova.
Park, Y., & Fritz, C. (2015). Spousal recovery support, recovery experiences, and life satisfaction crossover among dual-earner couples. Journal of Applied Psychology, 100(2), 557–566. https://doi.org/10.1037/a0037894 .
Park, Y. A., & Sprung, J. M. (2013). Work-school conflict and health outcomes: Beneficial resources for working college students. Journal of Occupational Health Psychology, 18 , 384–394. https://doi.org/10.1037/a0033614 .
Park, Y., & Sprung, J. M. (2015). Weekly work-school conflict, sleep quality, and fatigue: Recovering self-efficacy as a cross-level moderator. Journal of Organizational Behavior, 36 , 112–127. https://doi.org/10.1002/job.1953 .
Parker, K., & Wang, W. (2013). Modern parenthood: Roles of moms and dads converge as they balance work and family. Pew Research Center. Retrieved from: http://www.pewsocialtrends.org/2013/03/14/modern-parenthood-roles-of-moms-and-dads-converge-as-they-balance-work-and-family/ .
Parkinson, B., & Totterdell, P. (1999). Classifying affect regulation strategies. Cognition and Emotion, 13 , 277–303.
Phillips, W. J., & Ferguson, S. J. (2012). Self-compassion: A resource for positive aging. Journal of Gerontology, 68 (4), 529–539. https://doi.org/10.1093/geronb/gbs091 .
Podsako, P. M., MacKenzie, S. B., Lee, J.-Y., & Podsako, N. P. (2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology, 88 (5), 879–903. https://doi.org/10.1037/0021-9010.88.5.879 .
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers, 36 (4), 717–731.
Pryor, J. H., Hurtado, S., DeAngelo, L., Palucki Blake, L., & Tran, S. (2010). The American freshman: National norms fall 2010 . Los Angeles: Higher Education Research Institute, UCLA.
Qu, Y., Dasborough, M. T., & Todorova, G. (2015). Which mindfulness measures to choose to use? Industrial and Organizational Psychology: Perspectives on Science and Practice, 8 (04), 710–723. https://doi.org/10.1017/iop.2015.105 .
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the self-compassion scale. Clinical Psychology & Psychotherapy, 18 , 250–255. https://doi.org/10.1002/cpp.702 .
Roche, M., Haar, J. M., & Luthans, F. (2014). The role of mindfulness and psychological capital on the well-being of leaders. Journal of Occupational Health Psychology, 19 (4), 476–489. https://doi.org/10.1037/a0037183 .
Roeser, R. W., Schonert-Reichl, K. A., Jha, A., Cullen, M., Wallace, L., Wilensky, R., Oberle, E., Thomson, K., Taylor, C., & Harrison, J. (2013). Mindfulness training and reductions in teacher stress and burnout: Results from two randomized, waitlist-control field trials. Journal of Educational Psychology, 105 , 787–804. https://doi.org/10.1037/a0032093 .
Sanz-Vergel, A., Demerouti, E., Moreno-Jimenez, B., & Mayo, M. (2010). Work-family balance and energy: A day-level study on recovery conditions. Journal of Vocational Behavior, 76 (1), 118–130. https://doi.org/10.1016/j.jvb.2009.07.001 .
Seligman, M. E. P. (1998). Positive social science. APA monitor, 29 (4), 2–5.
Sherrington, C. B. (2014). Graduate psychology students' experience of stress: Is a symptom expression modified by dispositional mindfulness, experiential avoidance, and self-attention style? Dissertation Abstracts International, 75 , 117.
Sieber, S. D. (1974). Toward a theory of role accumulation. American Sociological Review, l39 (4), 567–578. https://doi.org/10.2307/2094422 .
Singh, N. N., Singh, A. N., Lancioni, G. E., Singh, J., Winton, A. S. W., & Adkins, A. D. (2010). Mindfulness training for parents and their children with ADHD increases the children’s compliance. Journal of Child and Family Studies, 19 , 157–166. https://doi.org/10.1007/s10826-009-9272-z .
Sirois, F. M. (2014). Procrastination and stress: Exploring the role of self- compassion. Self and Identity, 13 (2), 128–145. https://doi.org/10.1080/15298868.2013.763404 .
Siu, O. L., Cooper, C. L., & Phillips, D. R. (2014). Intervention studies on enhancing work well-being, reducing burnout, and improving recovery experiences among Hong Kong health care workers and teachers. International Journal of Stress Management, 21 (1), 69–84. https://doi.org/10.1037/a0033291 .
Sonnentag, S., & Fritz, C. (2007). The recovery experience questionnaire: Development and validation of a measure for assessing recuperation and unwinding from work. Journal of Occupational Health Psychology, 12 , 204–221. https://doi.org/10.1037/1076-8998.12.3.204 .
Soysa, C. K., & Wilcomb, C. J. (2013). Mindfulness, self-compassion, self-efficacy, and gender as predictors of depression, anxiety, stress, and well-being. Mindfulness, 6 , 217–226. https://doi.org/10.1007/s12671-013-0247-1 .
Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American College Health, 56 , 445–453. https://doi.org/10.3200/JACH.56.44.445-454 .
Stuart, E. A. (2010). Academy health: Advancing research, policy and practice. Academy Health . Retrieved from: www.academyhealth.org/files/2010/sunday/stuartE.pdf .
Tarrasch, R. (2015). Mindfulness meditation training for graduate students in educational counseling and special education: A qualitative analysis. Journal of Child and Family Studies, 24 (5), 1322–1333. https://doi.org/10.1007/s10826-014-9939-y .
Thompson, C. (2001). Conservation of resources theory. Sloan Network Encyclopedia. Retrieved from: https://workfamily.sas.upenn.edu/wfrn-repo/object/pt3yu38m2ae8vj2t .
Van der Klink, J. J. L., Blonk, R. W. B., Schene, A. H., & Van Dijk, F. J. H. (2001). The benefits of interventions for work-related stress. American Journal of Public Health, 91 , 270–276.
Wilks, S. E. (2008). Resilience amid academic stress: The moderating impact of social support among social work students. Advances in Social Work, 9 , 106–125 Retrieved.
Wilks, E. S., & Spivey, C. A. (2010). Resilience in undergraduate social work students: Social support and adjustment to academic stress. Social Work Education, 28 (3), 276–288.
Wyland, R. L., Lester, S. W., Mone, M. A., & Winkel, D. E. (2013). Work and school at the same time: A conflict perspective of the work–school interface. Journal of Leadership and Organizational Studies, 20 , 346–357. https://doi.org/10.1177/1548051813484360 .
Wyland, R., Lester, S. W., Ehrhardt, K., & Standifer, R. (2015). An examination of the relationship between the work–school interface, job satisfaction, and job performance. Journal of Business and Psychology, 31 (2), 187-203. https://doi.org/10.1007/s10869-015-9415-8 .
Download references
Acknowledgements
We would like to thank the editor and two anonymous reviewers for their helpful feedback.
Author information
Authors and affiliations.
University of Hartford, 200 Bloomfield Avenue, West Hartford, CT, 06119, USA
Jessica M. Nicklin & Emily J. Meachon
The College at Brockport, State University of New York, New York, NY, USA
Laurel A. McNall
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Jessica M. Nicklin .
Ethics declarations
Conflicts of interest.
There are no conflicts of interested associated with this paper and we did not include any identifying information in the manuscript.
Rights and permissions
Reprints and permissions
About this article
Nicklin, J.M., Meachon, E.J. & McNall, L.A. Balancing Work, School, and Personal Life among Graduate Students: a Positive Psychology Approach. Applied Research Quality Life 14 , 1265–1286 (2019). https://doi.org/10.1007/s11482-018-9650-z
Download citation
Received : 02 August 2017
Accepted : 09 July 2018
Published : 24 July 2018
Issue Date : November 2019
DOI : https://doi.org/10.1007/s11482-018-9650-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Self-compassion
- Mindfulness
- Graduate students
- Conservation of resources
- Find a journal
- Publish with us
- Track your research
Student mental health is in crisis. Campuses are rethinking their approach
Amid massive increases in demand for care, psychologists are helping colleges and universities embrace a broader culture of well-being and better equipping faculty to support students in need
Vol. 53 No. 7 Print version: page 60
- Mental Health

By nearly every metric, student mental health is worsening. During the 2020–2021 school year, more than 60% of college students met the criteria for at least one mental health problem, according to the Healthy Minds Study, which collects data from 373 campuses nationwide ( Lipson, S. K., et al., Journal of Affective Disorders , Vol. 306, 2022 ). In another national survey, almost three quarters of students reported moderate or severe psychological distress ( National College Health Assessment , American College Health Association, 2021).
Even before the pandemic, schools were facing a surge in demand for care that far outpaced capacity, and it has become increasingly clear that the traditional counseling center model is ill-equipped to solve the problem.
“Counseling centers have seen extraordinary increases in demand over the past decade,” said Michael Gerard Mason, PhD, associate dean of African American Affairs at the University of Virginia (UVA) and a longtime college counselor. “[At UVA], our counseling staff has almost tripled in size, but even if we continue hiring, I don’t think we could ever staff our way out of this challenge.”
Some of the reasons for that increase are positive. Compared with past generations, more students on campus today have accessed mental health treatment before college, suggesting that higher education is now an option for a larger segment of society, said Micky Sharma, PsyD, who directs student life’s counseling and consultation service at The Ohio State University (OSU). Stigma around mental health issues also continues to drop, leading more people to seek help instead of suffering in silence.
But college students today are also juggling a dizzying array of challenges, from coursework, relationships, and adjustment to campus life to economic strain, social injustice, mass violence, and various forms of loss related to Covid -19.
As a result, school leaders are starting to think outside the box about how to help. Institutions across the country are embracing approaches such as group therapy, peer counseling, and telehealth. They’re also better equipping faculty and staff to spot—and support—students in distress, and rethinking how to respond when a crisis occurs. And many schools are finding ways to incorporate a broader culture of wellness into their policies, systems, and day-to-day campus life.
“This increase in demand has challenged institutions to think holistically and take a multifaceted approach to supporting students,” said Kevin Shollenberger, the vice provost for student health and well-being at Johns Hopkins University. “It really has to be everyone’s responsibility at the university to create a culture of well-being.”
Higher caseloads, creative solutions
The number of students seeking help at campus counseling centers increased almost 40% between 2009 and 2015 and continued to rise until the pandemic began, according to data from Penn State University’s Center for Collegiate Mental Health (CCMH), a research-practice network of more than 700 college and university counseling centers ( CCMH Annual Report , 2015 ).
That rising demand hasn’t been matched by a corresponding rise in funding, which has led to higher caseloads. Nationwide, the average annual caseload for a typical full-time college counselor is about 120 students, with some centers averaging more than 300 students per counselor ( CCMH Annual Report , 2021 ).
“We find that high-caseload centers tend to provide less care to students experiencing a wide range of problems, including those with safety concerns and critical issues—such as suicidality and trauma—that are often prioritized by institutions,” said psychologist Brett Scofield, PhD, executive director of CCMH.
To minimize students slipping through the cracks, schools are dedicating more resources to rapid access and assessment, where students can walk in for a same-day intake or single counseling session, rather than languishing on a waitlist for weeks or months. Following an evaluation, many schools employ a stepped-care model, where the students who are most in need receive the most intensive care.
Given the wide range of concerns students are facing, experts say this approach makes more sense than offering traditional therapy to everyone.
“Early on, it was just about more, more, more clinicians,” said counseling psychologist Carla McCowan, PhD, director of the counseling center at the University of Illinois at Urbana-Champaign. “In the past few years, more centers are thinking creatively about how to meet the demand. Not every student needs individual therapy, but many need opportunities to increase their resilience, build new skills, and connect with one another.”
Students who are struggling with academic demands, for instance, may benefit from workshops on stress, sleep, time management, and goal-setting. Those who are mourning the loss of a typical college experience because of the pandemic—or facing adjustment issues such as loneliness, low self-esteem, or interpersonal conflict—are good candidates for peer counseling. Meanwhile, students with more acute concerns, including disordered eating, trauma following a sexual assault, or depression, can still access one-on-one sessions with professional counselors.
As they move away from a sole reliance on individual therapy, schools are also working to shift the narrative about what mental health care on campus looks like. Scofield said it’s crucial to manage expectations among students and their families, ideally shortly after (or even before) enrollment. For example, most counseling centers won’t be able to offer unlimited weekly sessions throughout a student’s college career—and those who require that level of support will likely be better served with a referral to a community provider.
“We really want to encourage institutions to be transparent about the services they can realistically provide based on the current staffing levels at a counseling center,” Scofield said.
The first line of defense
Faculty may be hired to teach, but schools are also starting to rely on them as “first responders” who can help identify students in distress, said psychologist Hideko Sera, PsyD, director of the Office of Equity, Inclusion, and Belonging at Morehouse College, a historically Black men’s college in Atlanta. During the pandemic, that trend accelerated.
“Throughout the remote learning phase of the pandemic, faculty really became students’ main points of contact with the university,” said Bridgette Hard, PhD, an associate professor and director of undergraduate studies in psychology and neuroscience at Duke University. “It became more important than ever for faculty to be able to detect when a student might be struggling.”
Many felt ill-equipped to do so, though, with some wondering if it was even in their scope of practice to approach students about their mental health without specialized training, Mason said.
Schools are using several approaches to clarify expectations of faculty and give them tools to help. About 900 faculty and staff at the University of North Carolina have received training in Mental Health First Aid , which provides basic skills for supporting people with mental health and substance use issues. Other institutions are offering workshops and materials that teach faculty to “recognize, respond, and refer,” including Penn State’s Red Folder campaign .
Faculty are taught that a sudden change in behavior—including a drop in attendance, failure to submit assignments, or a disheveled appearance—may indicate that a student is struggling. Staff across campus, including athletic coaches and academic advisers, can also monitor students for signs of distress. (At Penn State, eating disorder referrals can even come from staff working in food service, said counseling psychologist Natalie Hernandez DePalma, PhD, senior director of the school’s counseling and psychological services.) Responding can be as simple as reaching out and asking if everything is going OK.
Referral options vary but may include directing a student to a wellness seminar or calling the counseling center to make an appointment, which can help students access services that they may be less likely to seek on their own, Hernandez DePalma said. Many schools also offer reporting systems, such as DukeReach at Duke University , that allow anyone on campus to express concern about a student if they are unsure how to respond. Trained care providers can then follow up with a welfare check or offer other forms of support.
“Faculty aren’t expected to be counselors, just to show a sense of care that they notice something might be going on, and to know where to refer students,” Shollenberger said.
At Johns Hopkins, he and his team have also worked with faculty on ways to discuss difficult world events during class after hearing from students that it felt jarring when major incidents such as George Floyd’s murder or the war in Ukraine went unacknowledged during class.
Many schools also support faculty by embedding counselors within academic units, where they are more visible to students and can develop cultural expertise (the needs of students studying engineering may differ somewhat from those in fine arts, for instance).
When it comes to course policy, even small changes can make a big difference for students, said Diana Brecher, PhD, a clinical psychologist and scholar-in-residence for positive psychology at Toronto Metropolitan University (TMU), formerly Ryerson University. For example, instructors might allow students a 7-day window to submit assignments, giving them agency to coordinate with other coursework and obligations. Setting deadlines in the late afternoon or early evening, as opposed to at midnight, can also help promote student wellness.
At Moraine Valley Community College (MVCC) near Chicago, Shelita Shaw, an assistant professor of communications, devised new class policies and assignments when she noticed students struggling with mental health and motivation. Those included mental health days, mindful journaling, and a trip with family and friends to a Chicago landmark, such as Millennium Park or Navy Pier—where many MVCC students had never been.
Faculty in the psychology department may have a unique opportunity to leverage insights from their own discipline to improve student well-being. Hard, who teaches introductory psychology at Duke, weaves in messages about how students can apply research insights on emotion regulation, learning and memory, and a positive “stress mindset” to their lives ( Crum, A. J., et al., Anxiety, Stress, & Coping , Vol. 30, No. 4, 2017 ).
Along with her colleague Deena Kara Shaffer, PhD, Brecher cocreated TMU’s Thriving in Action curriculum, which is delivered through a 10-week in-person workshop series and via a for-credit elective course. The material is also freely available for students to explore online . The for-credit course includes lectures on gratitude, attention, healthy habits, and other topics informed by psychological research that are intended to set students up for success in studying, relationships, and campus life.
“We try to embed a healthy approach to studying in the way we teach the class,” Brecher said. “For example, we shift activities every 20 minutes or so to help students sustain attention and stamina throughout the lesson.”
Creative approaches to support
Given the crucial role of social connection in maintaining and restoring mental health, many schools have invested in group therapy. Groups can help students work through challenges such as social anxiety, eating disorders, sexual assault, racial trauma, grief and loss, chronic illness, and more—with the support of professional counselors and peers. Some cater to specific populations, including those who tend to engage less with traditional counseling services. At Florida Gulf Coast University (FGCU), for example, the “Bold Eagles” support group welcomes men who are exploring their emotions and gender roles.
The widespread popularity of group therapy highlights the decrease in stigma around mental health services on college campuses, said Jon Brunner, PhD, the senior director of counseling and wellness services at FGCU. At smaller schools, creating peer support groups that feel anonymous may be more challenging, but providing clear guidelines about group participation, including confidentiality, can help put students at ease, Brunner said.
Less formal groups, sometimes called “counselor chats,” meet in public spaces around campus and can be especially helpful for reaching underserved groups—such as international students, first-generation college students, and students of color—who may be less likely to seek services at a counseling center. At Johns Hopkins, a thriving international student support group holds weekly meetings in a café next to the library. Counselors typically facilitate such meetings, often through partnerships with campus centers or groups that support specific populations, such as LGBTQ students or student athletes.
“It’s important for students to see counselors out and about, engaging with the campus community,” McCowan said. “Otherwise, you’re only seeing the students who are comfortable coming in the door.”
Peer counseling is another means of leveraging social connectedness to help students stay well. At UVA, Mason and his colleagues found that about 75% of students reached out to a peer first when they were in distress, while only about 11% contacted faculty, staff, or administrators.
“What we started to understand was that in many ways, the people who had the least capacity to provide a professional level of help were the ones most likely to provide it,” he said.
Project Rise , a peer counseling service created by and for Black students at UVA, was one antidote to this. Mason also helped launch a two-part course, “Hoos Helping Hoos,” (a nod to UVA’s unofficial nickname, the Wahoos) to train students across the university on empathy, mentoring, and active listening skills.
At Washington University in St. Louis, Uncle Joe’s Peer Counseling and Resource Center offers confidential one-on-one sessions, in person and over the phone, to help fellow students manage anxiety, depression, academic stress, and other campus-life issues. Their peer counselors each receive more than 100 hours of training, including everything from basic counseling skills to handling suicidality.
Uncle Joe’s codirectors, Colleen Avila and Ruchika Kamojjala, say the service is popular because it’s run by students and doesn’t require a long-term investment the way traditional psychotherapy does.
“We can form a connection, but it doesn’t have to feel like a commitment,” said Avila, a senior studying studio art and philosophy-neuroscience-psychology. “It’s completely anonymous, one time per issue, and it’s there whenever you feel like you need it.”
As part of the shift toward rapid access, many schools also offer “Let’s Talk” programs , which allow students to drop in for an informal one-on-one session with a counselor. Some also contract with telehealth platforms, such as WellTrack and SilverCloud, to ensure that services are available whenever students need them. A range of additional resources—including sleep seminars, stress management workshops, wellness coaching, and free subscriptions to Calm, Headspace, and other apps—are also becoming increasingly available to students.
Those approaches can address many student concerns, but institutions also need to be prepared to aid students during a mental health crisis, and some are rethinking how best to do so. Penn State offers a crisis line, available anytime, staffed with counselors ready to talk or deploy on an active rescue. Johns Hopkins is piloting a behavioral health crisis support program, similar to one used by the New York City Police Department, that dispatches trained crisis clinicians alongside public safety officers to conduct wellness checks.
A culture of wellness
With mental health resources no longer confined to the counseling center, schools need a way to connect students to a range of available services. At OSU, Sharma was part of a group of students, staff, and administrators who visited Apple Park in Cupertino, California, to develop the Ohio State: Wellness App .
Students can use the app to create their own “wellness plan” and access timely content, such as advice for managing stress during final exams. They can also connect with friends to share articles and set goals—for instance, challenging a friend to attend two yoga classes every week for a month. OSU’s apps had more than 240,000 users last year.
At Johns Hopkins, administrators are exploring how to adapt school policies and procedures to better support student wellness, Shollenberger said. For example, they adapted their leave policy—including how refunds, grades, and health insurance are handled—so that students can take time off with fewer barriers. The university also launched an educational campaign this fall to help international students navigate student health insurance plans after noticing below average use by that group.
Students are a key part of the effort to improve mental health care, including at the systemic level. At Morehouse College, Sera serves as the adviser for Chill , a student-led advocacy and allyship organization that includes members from Spelman College and Clark Atlanta University, two other HBCUs in the area. The group, which received training on federal advocacy from APA’s Advocacy Office earlier this year, aims to lobby public officials—including U.S. Senator Raphael Warnock, a Morehouse College alumnus—to increase mental health resources for students of color.
“This work is very aligned with the spirit of HBCUs, which are often the ones raising voices at the national level to advocate for the betterment of Black and Brown communities,” Sera said.
Despite the creative approaches that students, faculty, staff, and administrators are employing, students continue to struggle, and most of those doing this work agree that more support is still urgently needed.
“The work we do is important, but it can also be exhausting,” said Kamojjala, of Uncle Joe’s peer counseling, which operates on a volunteer basis. “Students just need more support, and this work won’t be sustainable in the long run if that doesn’t arrive.”
Further reading
Overwhelmed: The real campus mental-health crisis and new models for well-being The Chronicle of Higher Education, 2022
Mental health in college populations: A multidisciplinary review of what works, evidence gaps, and paths forward Abelson, S., et al., Higher Education: Handbook of Theory and Research, 2022
Student mental health status report: Struggles, stressors, supports Ezarik, M., Inside Higher Ed, 2022
Before heading to college, make a mental health checklist Caron, C., The New York Times, 2022
Related topics
- Mental health
- Stress effects on the body
Contact APA
You may also like.
Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Article Menu

- Subscribe SciFeed
- Recommended Articles
- Google Scholar
- on Google Scholar
- Table of Contents
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
JSmol Viewer
Can social identities improve working students’ academic and social outcomes lessons from three studies.

Share and Cite
Grozev, V.H.; Easterbrook, M.J. Can Social Identities Improve Working Students’ Academic and Social Outcomes? Lessons from Three Studies. Educ. Sci. 2024 , 14 , 939. https://doi.org/10.3390/educsci14090939
Grozev VH, Easterbrook MJ. Can Social Identities Improve Working Students’ Academic and Social Outcomes? Lessons from Three Studies. Education Sciences . 2024; 14(9):939. https://doi.org/10.3390/educsci14090939
Grozev, Vladislav H., and Matthew J. Easterbrook. 2024. "Can Social Identities Improve Working Students’ Academic and Social Outcomes? Lessons from Three Studies" Education Sciences 14, no. 9: 939. https://doi.org/10.3390/educsci14090939
Article Metrics
Article access statistics, further information, mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
ORIGINAL RESEARCH article
Work-related mental health issues in graduate student population.

- 1 Instituto de Organizaciones Saludables, Universidad Siglo 21, Córdoba, Argentina
- 2 Vicerrectoria de Investigación, Pontifica Universidad Católica Madre y Maestra, Santiago de los Caballeros, Dominican Republic
The scientific and educational community is becoming increasingly aware of the impact of current academic working conditions on graduate students’ mental health and how this is affecting scientific progress and ultimately society as a whole. Our study aimed to shed light on the work-related mental health issues affecting graduate students, providing a comprehensive research work including psychological and biological assessment. Our findings showed that a sizeable number of graduate student present anxiety, depression, or high burnout and that the time spent in academia plays an important role. The graduate student population displayed a specific work-related mental health issues profile with an altered hypothalamic–pituitary–adrenal (HPA) axis and low levels of work engagement. Finally, graduate students were equally stressed, with less work engagement, and more anxious and depressed than general workers.
Introduction
Graduate students in most countries are not considered to be part of the labor force, even though in addition to their degree work they are frequently engaged as research and teaching assistants. These combined responsibilities, along with the psychosocial environment of graduate education, are entailed in the mental health issues associated with work. Burnout, the work-related stress syndrome, is one of these issues ( Cornér et al., 2017 ); it emerges in response to chronic interpersonal stressors on the job and can have a negative influence on an individual’s psychological and physical health ( Maslach et al., 2001 ). Furthermore, the Burnout syndrome may contribute to the development of pathological conditions such as anxiety and depression ( Harvey et al., 2013 ). These two other mental health problems in the workplace are recognized as the leading causes of sickness absence and long-term work disability ( Harvey et al., 2013 ).
Mental health issues in graduate students have been the focus of a few recent investigations, helping to make the problem visible ( Levecque et al., 2017 ; Evans et al., 2018 ). They show the graduate student population to be at risk of having or developing a common psychiatric disorder ( Levecque et al., 2017 ), with a high prevalence of anxiety and depression ( Garcia-Williams et al., 2014 ; Evans et al., 2018 ). However, research on the subject remains scarce and, in most cases, does not compare graduate students with the general working population, nor does it include biological assessment. Research on work engagement, a positive work-related state of well-being, has likewise been largely neglected in the graduate student population. This is a critical point since reducing stress or discomfort is not equivalent to increasing well-being ( Salanova et al., 2016 ). Therefore, the assessment of burnout syndrome along with work engagement in the graduate student population emerges as a crucial topic that could be fundamental to the development of early intervention and eventually help to prevent generalized anxiety and depression.
Whereas individual well-being is probably the more important concern, mental health issues could affect the quality and quantity of a researcher’s output, impact the functioning of research teams, and influence entry into and persistence in the research field ( Levecque et al., 2017 ). The combined effect on scientific advancement has high societal costs.
In light of the above, there is an urgent need for more integral studies to better analyze these risk factors with the aim of addressing more effective interventions targeting graduate students’ well-being and health.
In this work, we deployed a range of psychobiological tools to inquire into the work-related mental health issues in a graduate student population. We found that graduate students are deeply affected by these issues and that the accumulation of time spent in academia plays an important role. The graduate student population displayed a specific profile with an altered hypothalamic–pituitary–adrenal (HPA) axis, high levels of burnout, and low levels of work engagement. Finally, graduate students were more affected by these issues than general workers. It is hoped that the data presented here will prompt the international scientific community to take the necessary measures to fully address the issues involved.
Materials and Methods
Participants.
We conducted a cross-sectional study on a population of science-related graduate students in the field of physics, chemistry, and biology. A convenience sample of 153 Ph.D. students (59% women and 41% men) participated in the study. The sample comprised individuals with an average age of 28 years, SD = 3. All students were enrolled in universities within the authors’ country and recruitment was according to their availability and accessibility. To reduce participation bias, since participants who have had a history of anxiety or depression may be more apt to respond the survey, intense in-person engagement work was done to involve as many students as possible from each research institution visited. For comparison, we surveyed a population of 1,044 Argentinian workers (52% women and 48% men with an age average of 42 years, SD = 13) from diverse fields/types of work (see Supplementary Material) sampled with a probability (cluster) sampling method.
We requested all selected individuals to complete a self-administered questionnaire after reading an accompanying letter explaining the objectives of the study. Informed consent was obtained from all graduate students/participants in the study. In the case of the graduate students, we also provided them with three plastic tubes (Corning LS tubes of 15 ml) and detailed instructions on collecting saliva, emphasizing the need to strictly follow the time schedule and refrain from drinking, eating, and brushing their teeth before collecting the three saliva samples. Inclusion criteria for the study were as follows: representatives of both sexes, appropriate language ability (able to read and complete questionnaires in Spanish), signing of the corresponding informed consent form, and being an active worker with at least 1 months in the job at the time of the sampling. All participants were asked to provide information regarding potential covariates that could affect cortisol levels, considered as exclusion criteria: use of systemic or topical steroids in the last 4 weeks, intense exercise prior to sampling, report of consumption of steroid-based anti-inflammatory drugs, oral injuries or diseases, alcoholism, chemotherapy, prolonged corticotherapy, autoimmune diseases, and infection ( Morera et al., 2020 ). The study had the approval of the Hospital Nacional de Clínicas ethical committee (CIEIS-HNC) of the Faculty of Medical Sciences, National University of Córdoba, which has provincial jurisdiction. Finally, the study was conducted according to the Declaration of Helsinki on studies with human subjects.
Questionnaires
We provided all participants with a paper-and-pencil questionnaire that included a socio-demographic questionnaire and all the psychological instruments.
The socio-demographic questionnaire included personal details such as gender, age, research field, and starting date of postgraduate education, among other data. We assessed Anxiety and Depression with the brief Patient Health Questionnaire-4 (PHQ-4) ( Cano-Vindel et al., 2018 ). This instrument combines the two short versions (the GAD-2 and the PHQ-2) of the “Generalized Anxiety Disorder–7 scale” (GAD–7) and “Patient Health Questionnaire-9” (PHQ-9) ( Kroenke et al., 2009 ). The Spanish version of the PHQ-4 was validated in our group ( Cano-Vindel et al., 2018 ). GAD-2 and PHQ-2 items were rated on a four-point frequency scale, ranging from one (never) to four (daily). Anxiety and Depression scores for each individual were obtained by adding up the item scores of each respective disorder. We used the reported cutoff of three ( Cano-Vindel et al., 2018 ) in both GAD-2 and PHQ-2 to dichotomize into an Anxiety (A) and non-Anxiety (non-A) symptoms group and a Depressed (D) and non-Depressed (non-D) symptoms group, respectively.
To assess Burnout, we used the Argentinean version ( Spontón et al., 2019 ) of the Maslach Burnout Inventory-General Survey (MB-GS) ( Schaufeli and Buunk, 1996 ; Maslach et al., 2001 ). This included the exhaustion scale comprising five items (e.g., “I feel emotionally drained by my work”) and the cynicism scale comprising four items (e.g., “I have become less enthusiastic about my work”). We measured work engagement using the Argentinean version ( Spontón et al., 2012 ) of the Utrecht Work Engagement instrument (UWES) ( Schaufeli et al., 2002 ) comprising the vigor scale with six items (e.g., “at my work, I feel bursting with energy”) and the dedication scale, also with six items (e.g., “I am enthusiastic about my work”). MB-GS and UWES items were rated on a seven-point frequency scale, ranging from one ( never ) to seven ( daily ). In order to avoid response bias, we randomly merged all burnout and work engagement items into one questionnaire. Burnout and Work Engagement scores for each individual were obtained by adding up the item scores of each respective instrument. We dichotomized Burnout and work engagement by dividing the MB-GS and UWES total score into Low (≤25th percentile) and high (≥75th percentile). In this way, we obtained the Low Burnout (Low-B) and High Burnout (High-B) group and Low-Engagement (Low-E) and High-Engagement (High-E) group. We used the Low-B and Low-E groups as the reference categories. Dichotomous classification of burnout and work engagement has been used and recommended by different research groups ( Ishii et al., 2018 ; Penz et al., 2018 ).
Salivary Cortisol
Salivary cortisol was collected at three time points to determine the cortisol awakening response (CAR): immediately after awakening and 30 and 45 min thereafter ( Powell and Schlotz, 2012 ). All samples were stored at 4°C until sent to the laboratory, where they were then centrifuged for 5 min at 2,000 rpm to extract saliva with low viscosity and subsequently transferred to 1.5-ml tubes and stored in a freezer at –80°C until analysis. After thawing, 20 μl of salivary samples was transferred to a sample cup and cortisol was estimated using a cortisol RP Elecsys kit (Roche Diagnostics, United States) in a cobas e 411 analyzer. Summary indexes of CAR included the area under the curve with respect to ground (AUC G ) and the area under the curve with respect to increase (AUC I ) calculated according to the work of Pruessner et al. (2003) .
Data Analysis
All statistical analyses were performed using SPSS 23.0 (IBM., Chicago, IL, United States). We describe continuous variables using mean with the standard deviation (SD)/standard error of the median (SE) and qualitative variables using frequency (percentage). Skewness and kurtosis were used to test the normality distribution for numeric variables. For univariate analysis, we applied independent t test to compare mean values between the two groups. We used the Pearson bivariate correlation to evaluate the linear relationship between month spent in graduate education and the mental health issue scores. In the analytical procedures, a two-sided value of <0.05 was considered as statistically significant. All analyses controlled age, sex, and type of work.
Graduate Education: Disadvantages and Drawbacks for Mental Health
With the aim of analyzing the relationship between work-related mental health issues and graduate education, we used a psychobiological approach to assess a cohort of 153 science-related graduate students. Individuals were from the biological, chemical, and physical sciences, 59% women and 41% men, with an average age of 28 years, SD = 3.
We relied on psychological tools to address a comprehensive study of the work-related mental health issues prevalence in this population and their relationship with graduate education. We included an anxiety and depression assessment and also Burnout and Work engagement, two of the lesser studied issues in this population. Based on the cutoff value of three for the GAD-2 anxiety scale and PHQ-2 for the depression scale ( Cano-Vindel et al., 2018 ), we found a prevalence of 68% for anxiety symptoms and 50% for depression symptoms ( Figure 1A ). In line with the results of Evans and co-workers, our findings show that these common mental issues have a high prevalence in graduate students. Differences in the percentages between the two studies may be related to the sample characteristics or the specificity/sensitivity relation of the psychological instrument. As shown in Figure 1B , the Pearson correlation statistic showed a significant positive correlation between the time elapsed in graduate education and both anxiety and depression scores. These data suggest that graduate education is positively related to these issues.

Figure 1. Psychobiological assessment of work-related mental health issues in graduate students. (A) Prevalence of the work-related mental health issues within the population of graduate students analyzed. (B) Linear correlation of months of graduate education with Anxiety (Pearson r = 0.337, p = < 0.001), Depression (Pearson r = 0.195, p = < 0.05), Burnout (Pearson r = 0.454, p = < 0.001), and Work Engagement (Pearson r = −0.424, p = < 0.001) scores among the students. (C) Comparison of the cortisol awaking response (CAR) and its respective indices (AUC G and AUC I ) between the different graduate student groups, i.e., graduate students with (A) and without anxiety symptoms (non-A), with (D) and without (non-D) depression symptoms, with High (High-B) and Low (Low-B) Burnout, and with High (High-E) and low (Low-E) work engagement. The graphs show mean values, with error bars representing the standard error of the mean. Statistical significance: * p < 0.05; ** p < 0.01.
Various studies have shown that graduate students commonly feel stress and exhaustion, among other negative symptoms ( Hyun et al., 2007 ; Cornér et al., 2017 ). It was reported that a population of graduate dental students presented high rates of burnout symptoms, particularly emotional exhaustion and reduced personal accomplishment ( Divaris et al., 2012 ). We therefore analyzed the prevalence of burnout in this graduate student population. We measured the manifestation of emotional exhaustion and cynicism toward their work, two of the main domains of burnout present in the Maslach Burnout Inventory (MBI) ( Spontón et al., 2019 ). The scores obtained were added up and expressed as the burnout score. As in studies by other groups, further dichotomization was used to categorize into low burnout vs. high burnout (see section “Materials and Methods”). We found that an appreciable amount of students (28%) ( Figure 1A ) presented high burnout and that burnout scores tended to be higher as the months of graduate education increased ( Figure 1B ). We analyzed work engagement in the same manner. Work engagement is understood as a positive work-related affective–cognitive state of mind characterized by the manifestation of vigor and dedication in one’s work ( Attridge, 2009 ). It is important to measure work engagement independently of burnout since it is not considered to be an exact counterpart to the latter ( Schaufeli and Salanova, 2011 ). We obtained the work engagement score as the sum of the measured vigor and dedication scores from the Utrecht Work Engagement Scale (UWES) ( Spontón et al., 2012 ), categorizing them into low and high work engagement. As shown in Figures 1A,B , only 9% of graduate students presented high work engagement and there is an inverse correlation between the months spent in graduate education and the work engagement score. Collectively, the data presented above demonstrate that work-related mental health issues favored by graduate student education have a considerable prevalence in the graduate student community, to the detriment of well-being.
Glucocorticoid Dysregulation in Graduate Students
Deregulation of the HPA axis by the work-related mental health issues analyzed in this work has been widely demonstrated. For instance, symptoms for anxiety and depressive disorders have been linked with hypersecretion of corticotropin-releasing hormone (CRH) and high levels of circulating glucocorticoids ( Gold et al., 2002 ; Schulkin, 2011 ). However, high levels of cortisol have been positively associated with burnout syndrome ( Penz et al., 2018 ), this finding being in dissonance with other studies reporting a negative relationship between these variables ( Oosterholt et al., 2015 ; Pilger et al., 2018 ). In addition, differences in cortisol suppression in response to the dexamethasone suppression test were found between burnout and engaged workers, indicating a higher HPA axis feedback sensitivity for the latter ( Langelaan et al., 2006 ; Bakker et al., 2011 ). Nevertheless, only few biological assessments have been conducted on the graduate student population. Ignacchiti and co-workers showed high plasma cortisol concentration in graduate students with pre-final examination anxiety ( Ignacchiti et al., 2011 ), while flattening of cortisol awaking response (CAR) was determined before the graduate education entrance exam ( Duan et al., 2013 ) and after the first year ( McGregor et al., 2016 ). To further analyze how work-related mental issues in graduate students are associated with dysregulation of their HPA axis, we measured the CAR in this population. A plethora of studies have suggested the CAR as a standard tool for testing HPA axis integrity ( Fries et al., 2009 ). To determine CAR, salivary cortisol was sampled at three time points, immediately upon awakening (CORT-1) and 30 (CORT-2) and 45 (CORT-3) min later ( Powell and Schlotz, 2012 ). Cortisol was compared between groups of graduate students with different disorders and their counterparts ( Figure 1C ). All three cortisol measures as well as the widely used and recommended summary indexes of CAR, i.e., the AUC G and the AUC I ( Pruessner et al., 2003 ), were contrasted. While AUC G is related to total hormonal output, AUC I emphasizes changes over time and is associated with the sensitivity of the system ( Fekedulegn et al., 2007 ). Compared to the non-Anxiety group (non-A), results show significantly higher mean values for COR-2, CORT-3, and AUC G in the Anxiety group (A) ( Figure 1C ), indicating an altered cortisol secretion immediately after awaking. A cortisol increase was also found in the depression (D) and the high burnout (High-B) group with a significant value in AUC G for the former and a more marked significant difference in COR-1, CORT-2, CORT-3, and AUC G for the latter ( Figure 1C ). In the High-B group, the higher level of CORT-1 indicates a dysregulation of cortisol that may reflect altered nocturnal secretion patterns in individuals with these issues. In this regard, it has been shown that CORT-1 levels reflect secretory activity during the late stages of sleep ( Wilhelm et al., 2007 ). High levels of cortisol in the inactive/night period were associated with stress-related sleep deprivation, acting as a risk factor for insulin resistance ( McEwen, 2006 ). It is worth mentioning that AUC I mean values were not significantly different between these groups, demonstrating that changes in the total amounts of the hormone were not accompanied by changes in cortisol profiles and in rates of change ( Fekedulegn et al., 2007 ).
Finally, we found an opposite trend in work engagement, but the differences with their counterparts were not significant. This is in agreement with the idea that engaged employees need to mobilize resources to face job demands, giving rise to a state of activation–tension where cortisol may participate in an orchestrated manner.
Graduate Students Are More Affected by These Issues Than the General Working Population
To determine whether the psychosocial conditions of graduate education are as detrimental as those of works in general, we carried out a first-time comparison between graduate students and a population of 1,044 employees. The employees analyzed were from diverse fields/types of work, ages, and genders. The results of the comparative analysis between the two groups in terms of the mental health issues cited above are shown in Figure 2 . The scores were significantly higher in the graduate student group for Anxiety and Depression symptoms, indicating that, in line with previous research ( Evans et al., 2018 ), this population is more likely to experience these two common mental health issues. The differences observed between the two population were independent of age, sex, and type of work. A comparison of burnout scores showed no significant differences between the two populations ( Figure 2 ), indicating that graduate students experience similar work-related stress to general workers.

Figure 2. Graduate student vs. general worker population. Comparison of the work-related mental health issues scores between the graduate student population (color bars) and the general working population (gray bars). The graphs show mean values, with error bars representing the standard error of the mean. Statistical significance: ** p < 0.01.
Work engagement encompasses dedication, enthusiasm, inspiration, and pride, in addition to a sense of meaning and being challenged by one’s work. Individuals with low engagement have a worrying psychological profile, with lower levels of energy and mental resistance and a lower desire to invest effort in their work. Despite the importance of work engagement, to the best of our knowledge, no previous study has measured it in the graduate student population. Surprisingly, our evaluation of work engagement in this population shows a significantly lower mean score than in the case of the working population in general ( Figure 2 ).
Overall, our findings show that the graduate education environment is more detrimental to mental health than general working conditions and is also unfavorable to well-being.
In recent years, there has been a growing awareness that not all occupational hazards have a physical occurrence. Substantial scientific evidence indicates that psychosocial factors can deeply affect the physical and mental health of workers. In this regard, the World Health Organization has underlined the need to strengthen efforts to extrapolate the impact of psychosocial risk on different health outcomes with the aim of improving the health of workers around the globe ( Leka et al., 2010 ). This is particularly important in the context of the scientific community and in particular graduate students, who are not immune to these problems; research is required with a specific focus on their particular characteristics and environment. Our study aimed to shed light on the work-related mental health issues affecting graduate students, providing a comprehensive study including psychological and biological assessment. We show that a sizeable number of graduate student present anxiety, depression, or high burnout and that these disorders are accompanied by the unbalanced secretion of cortisol. This is critical due to the implication of cortisol, as a biological intermediary, in different medical conditions including metabolic syndrome, cancer, obesity, cardiovascular disease, and increased susceptibility to infections ( Russell and Lightman, 2019 ). The association we found between months spent in graduate education and these work-related mental health issues indicates the decisive role that graduate education plays in these disorders and opens up a novel scenario for research focus. Furthermore, we found that graduate students are equally stressed and more anxious and depressed than general workers.
Bearing in mind that well-being is not equivalent to reduced discomfort, we evaluated work engagement in graduate students. Our findings show a negative impact of graduate education on work engagement, the latter being lower in the graduate student population than among general workers. Empirical research shows that workers with vigor and dedication, two key aspects of work engagement, are able to create their own resources, helping them to perform better ( Bakker et al., 2008 ). Promoting work engagement may not only benefit graduate students’ well-being but also enhance their scientific output.
Taken together, these findings highlight the importance of addressing work-related mental health issues in graduate students, a deeply affected segment of the population, and serve toward the implementation of decision-making processes and new policies. In line with this, it is also necessary to empirically determine the psychosocial factors that influence well-being in graduate education. Some of these factors are perhaps what we like to call “diseases of science,” such as the publish or perish culture ( Kiai, 2019 ; Poppelaars et al., 2019 ) or the replication crisis ( Pashler and Wagenmakers, 2012 ; Smith, 2017 ), that affect the scientific community in general and the progress of science. In this regard, a recent survey of more than 4,000 scientists indicates that 55% have a negative impression of research culture, and one-quarter said that the culture damaged the quality of research ( Abbott, 2020 ). It is most likely that additional factors specific to the graduate student population are also at play, such as mentorship relationships ( Evans et al., 2018 ), job demands ( Levecque et al., 2017 ), etc. Are all these psychosocial factors promoting work-related mental health issues? Is there a vicious cycle of factors and disorders? Can all this generate a distinct pattern of comorbidity leading to a more complex “Science disease”? These are all questions that need to be answered.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by Hospital Nacional de Clínicas ethical committee (CIEIS-HNC) of the Faculty of Medical Sciences, National University of Córdoba. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LM conceived the project. JG and LM conducted the experiments. JG analyzed the data and wrote the manuscript. All authors discussed the results and read and approved the final manuscript.
This work was supported by grants from Siglo 21 University and the Ministry of Science and Technology of Córdoba.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
JG and LM acknowledge their postdoctoral fellowships from the National Scientific and Technical Research Council of Argentina (CONICET). We would like to dedicate this work to all those Argentinean graduate students who fight for their well-being and to be recognized as employees.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2021.593562/full#supplementary-material
Abbott, A. (2020). Stress, anxiety, harassment: huge survey reveals pressures of scientists’ working lives. Nature 577, 460–461. doi: 10.1038/d41586-020-00101-9
PubMed Abstract | CrossRef Full Text | Google Scholar
Attridge, M. (2009). Measuring and managing employee work engagement: a review of the research and business literature. J. Workplace Behav. Health 24, 383–398. doi: 10.1080/15555240903188398
CrossRef Full Text | Google Scholar
Bakker, A. B., Albrecht, S. L., and Leiter, M. P. (2011). Key questions regarding work engagement. Eur. J. Work Organ. Psychol. 20, 4–28. doi: 10.1080/1359432X.2010.485352
Bakker, A. B., Schaufeli, W. B., Leiter, M. P., and Taris, T. W. (2008). Work engagement: an emerging concept in occupational health psychology. Work Stress 22, 187–200. doi: 10.1080/02678370802393649
Cano-Vindel, A., Muñoz-Navarro, R., Medrano, L. A., Ruiz-Rodríguez, P., González-Blanch, C., Gómez-Castillo, M. D., et al. (2018). A computerized version of the patient health questionnaire-4 as an ultra-brief screening tool to detect emotional disorders in primary care. J. Affect. Disord. 234, 247–255. doi: 10.1016/j.jad.2018.01.030
Cornér, S., Löfström, E., and Pyhältö, K. (2017). The relationships between doctoral students’ perceptions of supervision and burnout. Int. J. Dr. Stud. 12, 91–106.
Google Scholar
Divaris, K., Polychronopoulou, A., Taoufik, K., Katsaros, C., and Eliades, T. (2012). Stress and burnout in postgraduate dental education. Eur. J. Den. Educ. 16, 35–42. doi: 10.1111/j.1600-0579.2011.00715.x
Duan, H., Yuan, Y., Zhang, L., Qin, S., Zhang, K., Buchanan, T. W., et al. (2013). Chronic stress exposure decreases the cortisol awakening response in healthy young men. Stress 16, 630–637. doi: 10.3109/10253890.2013.840579
Evans, T. M., Bira, L., Gastelum, J. B., Weiss, L. T., and Vanderford, N. L. (2018). Evidence for a mental health crisis in graduate education. Nat. Biotechnol. 36, 282–284. doi: 10.1038/nbt.4089
Fekedulegn, D. B., Andrew, M. E., Burchfiel, C. M., Violanti, J. M., Hartley, T. A., Charles, L. E., et al. (2007). Area under the curve and other summary indicators of repeated waking cortisol measurements. Psychosom. Med. 69, 651–659. doi: 10.1097/psy.0b013e31814c405c
Fries, E., Dettenborn, L., and Kirschbaum, C. (2009). The cortisol awakening response (CAR): facts and future directions. Int. J. Psychophysiol. 72, 67–73. doi: 10.1016/j.ijpsycho.2008.03.014
Garcia-Williams, A. G., Moffitt, L., and Kaslow, N. J. (2014). Mental health and suicidal behavior among graduate students. Acad. Psychiatry 38, 554–560. doi: 10.1007/s40596-014-0041-y
Gold, P. W., Drevets, W. C., and Charney, D. S. (2002). New insights into the role of cortisol and the glucocorticoid receptor in severe depression. Biol. Psychiatry 52, 381–385. doi: 10.1016/s0006-3223(02)01480-4
Harvey, S., Joyce, S., Modini, M., Christensen, H., Bryant, R., Mykletun, A., et al. (2013). Work and Depression/Anxiety Disorders: A Systematic Review of Reviews. Melbourne VIC: Beyondblue.
Hyun, J., Quinn, B., Madon, T., and Lustig, S. (2007). Mental health need, awareness, and use of counseling services among international graduate students. J. Am. College Health 56, 109–118. doi: 10.3200/jach.56.2.109-118
Ignacchiti, M., Sesti-Costa, R., Marchi, L., Chedraoui-Silva, S., and Mantovani, B. (2011). Effect of academic psychological stress in post-graduate students: the modulatory role of cortisol on superoxide release by neutrophils. Stress 14, 290–300. doi: 10.3109/10253890.2010.545459
Ishii, K., Shibata, A., and Oka, K. (2018). Work engagement, productivity, and self-reported work-related sedentary behavior among japanese adults: a cross-sectional study. J. Occup. Environ. Med. 60:e173–e177. doi: 10.1097/JOM.0000000000001270
Kiai, A. (2019). To protect credibility in science, banish “publish or perish”. Nat. Hum. Behav. 3, 1017–1018. doi: 10.1038/s41562-019-0741-0
Kroenke, K., Spitzer, R. L., Williams, J. B., and Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: the PHQ–4. Psychosomatics 50, 613–621. doi: 10.1176/appi.psy.50.6.613
Langelaan, S., Bakker, A. B., Schaufeli, W. B., van Rhenen, W., and van Doornen, L. J. (2006). Do burned-out and work-engaged employees differ in the functioning of the hypothalamic-pituitary-adrenal axis? Scand. J. Work Environ. Health 32, 339–348. doi: 10.5271/sjweh.1029
Leka, S., Jain, A., and Organization, W. H. (2010). Health Impact of Psychosocial Hazards at Work: An Overview. Geneva: World Health Organization.
Levecque, K., Anseel, F., De Beuckelaer, A., Van der Heyden, J., and Gisle, L. (2017). Work organization and mental health problems in PhD students. Res. Policy 46, 868–879. doi: 10.1016/j.respol.2017.02.008
Maslach, C., Schaufeli, W. B., and Leiter, M. P. (2001). Job burnout. Annu. Rev. Psychol. 52, 397–422. doi: 10.1146/annurev.psych.52.1.397
McEwen, B. S. (2006). Sleep deprivation as a neurobiologic and physiologic stressor: allostasis and allostatic load. Metabolism 55, S20–S23.
McGregor, B. A., Murphy, K. M., Albano, D. L., and Ceballos, R. M. (2016). Stress, cortisol, and B lymphocytes: a novel approach to understanding academic stress and immune function. Stress 19, 185–191. doi: 10.3109/10253890.2015.1127913
Morera, L. P., Gallea, J. I., Trógolo, M. A., Guido, M. E., and Medrano, L. A. (2020). From work well-being to burnout: a hypothetical phase model. Front. Neurosci. 14:360. doi: 10.3389/fnins.2020.00360
Oosterholt, B. G., Maes, J. H. R., Van der Linden, D., Verbraak, M. J. P. M., and Kompier, M. A. J. (2015). Burnout and cortisol: evidence for a lower cortisol awakening response in both clinical and non-clinical burnout. J. Psychosom. Res. 78, 445–451. doi: 10.1016/j.jpsychores.2014.11.003
Pashler, H., and Wagenmakers, E. J. (2012). Editors’ introduction to the special section on replicability in psychological science: a crisis of confidence? Perspect. Psychol. Sci. 7, 528–530. doi: 10.1177/1745691612465253
Penz, M., Stalder, T., Miller, R., Ludwig, V. M., Kanthak, M. K., and Kirschbaum, C. (2018). Hair cortisol as a biological marker for burnout symptomatology. Psychoneuroendocrinology 87, 218–221. doi: 10.1016/j.psyneuen.2017.07.485
Pilger, A., Haslacher, H., Meyer, B. M., Lackner, A., Nassan-Agha, S., Nistler, S., et al. (2018). Midday and nadir salivary cortisol appear superior to cortisol awakening response in burnout assessment and monitoring. Sci. Rep. 8:9151. doi: 10.1038/s41598-018-27386-1
Poppelaars, E. S., Rattel, J., Wislowska, M., Hahn, M., Rodriguez-Cabello, S. F., and El Rassi, E. (2019). Publish-Or-Perish Culture: A PhD student Perspective. Basingstoke: Springer Nature.
Powell, D. J., and Schlotz, W. (2012). Daily life stress and the cortisol awakening response: testing the anticipation hypothesis. PLoS One 7:e52067. doi: 10.1371/journal.pone.0052067
Pruessner, J. C., Kirschbaum, C., Meinlschmid, G., and Hellhammer, D. H. (2003). Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 28, 916–931. doi: 10.1016/S0306-4530(02)00108-7
Russell, G., and Lightman, S. (2019). The human stress response. Nat. Rev. Endocrinol. 15, 525–534.
Salanova, M., Llorens, S., and Martínez, I. M. (2016). Aportaciones desde la psicología organizacional positiva para desarrollar organizaciones saludables y resilientes. [Contributions from positive organizational psychology to develop healthy & resilient organizations. Pap. Psicól. 37, 177–184.
Schaufeli, W., and Salanova, M. (2011). Work engagement: on how to better catch a slippery concept. Eur. J. Work Organ. Psychol. 20, 39–46. doi: 10.1080/1359432x.2010.515981
Schaufeli, W. B., and Buunk, B. P. (1996). Professional burnout. Handb. work Health Psychol. 1, 383–425.
Schaufeli, W. B., Salanova, M., González-Romá, V., and Bakker, A. B. (2002). The measurement of engagement and burnout: a two sample confirmatory factor analytic approach. J. Happiness Stud. 3, 71–92.
Schulkin, J. (2011). Evolutionary conservation of glucocorticoids and corticotropin releasing hormone: behavioral and physiological adaptations. Brain Res. 1392, 27–46. doi: 10.1016/j.brainres.2011.03.055
Smith, N. (2017). Why’Statistical Significance’Is Often Insignificant. New York, NY: Bloomberg.
Spontón, C., Medrano, L. A., Maffei, L., Spontón, M., and Castellano, E. (2012). Validación del cuestionario de engagement UWES a la población de trabajadores de Córdoba, Argentina. Liberabit 18, 147–154.
Spontón, C., Trógolo, M., Castellano, E., and Medrano, L. A. (2019). Medición del burnout: estructura factorial, validez y confiabilidad en trabajadores argentinos measurement of burnout: factor structure, validity and reliability in argentinean. Interdisciplinaria 36, 87–103.
Wilhelm, I., Born, J., Kudielka, B. M., Schlotz, W., and Wüst, S. (2007). Is the cortisol awakening rise a response to awakening? Psychoneuroendocrinology 32, 358–366. doi: 10.1016/j.psyneuen.2007.01.008
Keywords : graduate students, mental health, well-being, burnout, cortisol, HPA axis (hypothalamus–pituitary–adrenal), engagement
Citation: Gallea JI, Medrano LA and Morera LP (2021) Work-Related Mental Health Issues in Graduate Student Population. Front. Neurosci. 15:593562. doi: 10.3389/fnins.2021.593562
Received: 10 August 2020; Accepted: 08 March 2021; Published: 01 April 2021.
Reviewed by:
Copyright © 2021 Gallea, Medrano and Morera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Ignacio Gallea, [email protected]
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
- About The Journalist’s Resource
- Follow us on Facebook
- Follow us on Twitter
- Criminal Justice
- Environment
- Politics & Government
- Race & Gender
Expert Commentary
Improving college student mental health: Research on promising campus interventions
Hiring more counselors isn’t enough to improve college student mental health, scholars warn. We look at research on programs and policies schools have tried, with varying results.

Republish this article

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License .
by Denise-Marie Ordway, The Journalist's Resource September 13, 2023
This <a target="_blank" href="https://journalistsresource.org/education/college-student-mental-health-research-interventions/">article</a> first appeared on <a target="_blank" href="https://journalistsresource.org">The Journalist's Resource</a> and is republished here under a Creative Commons license.<img src="https://journalistsresource.org/wp-content/uploads/2020/11/cropped-jr-favicon-150x150.png" style="width:1em;height:1em;margin-left:10px;">
If you’re a journalist covering higher education in the U.S., you’ll likely be reporting this fall on what many healthcare professionals and researchers are calling a college student mental health crisis.
An estimated 49% of college students have symptoms of depression or anxiety disorder and 14% seriously considered committing suicide during the past year, according to a national survey of college students conducted during the 2022-23 school year. Nearly one-third of the 76,406 students who participated said they had intentionally injured themselves in recent months.
In December, U.S. Surgeon General Vivek Murthy issued a rare public health advisory calling attention to the rising number of youth attempting suicide , noting the COVID-19 pandemic has “exacerbated the unprecedented stresses young people already faced.”
Meanwhile, colleges and universities of all sizes are struggling to meet the need for mental health care among undergraduate and graduate students. Many schools have hired more counselors and expanded services but continue to fall short.
Hundreds of University of Houston students held a protest earlier this year , demanding the administration increase the number of counselors and make other changes after two students died by suicide during the spring semester, the online publication Chron reported.
In an essay in the student-run newspaper , The Cougar, last week, student journalist Malachi Key blasts the university for having one mental health counselor for every 2,122 students, a ratio higher than recommended by the International Accreditation of Counseling Services , which accredits higher education counseling services.
But adding staff to a campus counseling center won’t be enough to improve college student mental health and well-being, scholars and health care practitioners warn.
“Counseling centers cannot and should not be expected to solve these problems alone, given that the factors and forces affecting student well-being go well beyond the purview and resources that counseling centers can bring to bear,” a committee of the National Academies of Sciences, Engineering, and Medicine writes in a 2021 report examining the issue.
Advice from prominent scholars
The report is the culmination of an 18-month investigation the National Academies launched in 2019, at the request of the federal government, to better understand how campus culture affects college student mental health and well-being. Committee members examined data, studied research articles and met with higher education leaders, mental health practitioners, researchers and students.
The committee’s key recommendation: that schools take a more comprehensive approach to student mental health, implementing a wide range of policies and programs aimed at preventing mental health problems and improving the well-being of all students — in addition to providing services and treatment for students in distress and those with diagnosed mental illnesses.
Everyone on campus, including faculty and staff across departments, needs to pitch in to establish a new campus culture, the committee asserts.
“An ‘all hands’ approach, one that emphasizes shared responsibility and a holistic understanding of what it means in practice to support students, is needed if institutions of higher education are to intervene from anything more than a reactive standpoint,” committee members write. “Creating this systemic change requires that institutions examine the entire culture and environment of the institution and accept more responsibility for creating learning environments where a changing student population can thrive.”
In a more recent analysis , three leading scholars in the field also stress the need for a broader plan of action.
Sara Abelson , a research assistant professor at Temple University’s medical school; Sarah Lipson , an associate professor at the Boston University School of Public Health; and Daniel Eisenberg , a professor of health policy and management at the University of California, Los Angeles’ School of Public Health, have been studying college student mental health for years.
Lipson and Eisenberg also are principal investigators for the Healthy Minds Network , which administers the Healthy Minds Study , a national survey of U.S college students conducted annually to gather information about their mental health, whether and how they receive mental health care and related issues.
Abelson, Lipson and Eisenberg review the research to date on mental health interventions for college students in the 2022 edition of Higher Education: Handbook of Theory and Research . They note that while the evidence indicates a multi-pronged approach is best, it’s unclear which specific strategies are most effective.
Much more research needed
Abelson, Lipson and Eisenberg stress the need for more research. Many interventions in place at colleges and universities today — for instance, schoolwide initiatives aimed at reducing mental health stigma and encouraging students to seek help when in duress – should be evaluated to gauge their effectiveness, they write in their chapter, “ Mental Health in College Populations: A Multidisciplinary Review of What Works, Evidence Gaps, and Paths Forward .”
They add that researchers and higher education leaders also need to look at how campus operations, including hiring practices and budgetary decisions, affect college student mental health. It would be helpful to know, for example, how students are impacted by limits on the number of campus counseling sessions they can have during a given period, Abelson, Lipson and Eisenberg suggest.
Likewise, it would be useful to know whether students are more likely to seek counseling when they must pay for their sessions or when their school charges every member of the student body a mandatory health fee that provides free counseling for all students.
“These financially-based considerations likely influence help-seeking and treatment receipt, but they have not been evaluated within higher education,” they write.
Interventions that show promise
The report from the National Academies of Sciences, Engineering, and Medicine and the chapter by Abelson, Lipson and Eisenberg both spotlight programs and policies shown to prevent mental health problems or improve the mental health and well-being of young people. However, many intervention studies focus on high school students, specific groups of college students or specific institutions. Because of this, it can be tough to predict how well they would work across the higher education landscape.
Scientific evaluations of these types of interventions indicate they are effective:
- Building students’ behavior management skills and having them practice new skills under expert supervision . An example: A class that teaches students how to use mindfulness to improve their mental and physical health that includes instructor-led meditation exercises.
- Training some students to offer support to others , including sharing information and organizing peer counseling groups. “Peers may be ‘the single most potent source of influence’ on student affective and cognitive growth and development during college,” Abelson, Lipson and Eisenberg write.
- Reducing students’ access to things they can use to harm themselves , including guns and lethal doses of over-the-counter medication.
- Creating feelings of belonging through activities that connect students with similar interests or backgrounds.
- Making campuses more inclusive for racial and ethnic minorities, LGBTQ+ students and students who are the first in their families to go to college. One way to do that is by hiring mental health professionals trained to recognize, support and treat students from different backgrounds. “Research has shown that the presentation of [mental health] symptoms can differ based on racial and ethnic backgrounds, as can engaging in help-seeking behaviors that differ from those of cisgender, heteronormative white men,” explain members of National Academies of Sciences, Engineering, and Medicine committee.
Helping journalists sift through the evidence
We encourage journalists to read the full committee report and aforementioned chapter in Higher Education: Handbook of Theory and Research . We realize, though, that many journalists won’t have time to pour over the combined 304 pages of text to better understand this issue and the wide array of interventions colleges and universities have tried, with varying success.
To help, we’ve gathered and summarized meta-analyses that investigate some of the more common interventions. Researchers conduct meta-analyses — a top-tier form of scientific evidence — to systematically analyze all the numerical data that appear in academic studies on a given topic. The findings of a meta-analysis are statistically stronger than those reached in a single study, partly because pooling data from multiple, similar studies creates a larger sample to examine.
Keep reading to learn more. And please check back here occasionally because we’ll add to this list as new research on college student mental health is published.
Peer-led programs
Stigma and Peer-Led Interventions: A Systematic Review and Meta-Analysis Jing Sun; et al. Frontiers in Psychiatry, July 2022.
When people diagnosed with a mental illness received social or emotional support from peers with similar mental health conditions, they experienced less stress about the public stigma of mental illness, this analysis suggests.
The intervention worked for people from various age groups, including college students and middle-aged adults, researchers learned after analyzing seven studies on peer-led mental health programs written or published between 1975 and 2021.
Researchers found that participants also became less likely to identify with negative stereotypes associated with mental illness.
All seven studies they examined are randomized controlled trials conducted in the U.S., Germany or Switzerland. Together, the findings represent the experiences of a total of 763 people, 193 of whom were students at universities in the U.S.
Researchers focused on interventions designed for small groups of people, with the goal of reducing self-stigma and stress associated with the public stigma of mental illness. One or two trained peer counselors led each group for activities spanning three to 10 weeks.
Five of the seven studies tested the Honest, Open, Proud program, which features role-playing exercises, self-reflection and group discussion. It encourages participants to consider disclosing their mental health issues, instead of keeping them a secret, in hopes that will help them feel more confident and empowered. The two other programs studied are PhotoVoice , based in the United Kingdom, and
“By sharing their own experiences or recovery stories, peer moderators may bring a closer relationship, reduce stereotypes, and form a positive sense of identity and group identity, thereby reducing self-stigma,” the authors of the analysis write.
Expert-led instruction
The Effects of Meditation, Yoga, and Mindfulness on Depression, Anxiety, and Stress in Tertiary Education Students: A Meta-Analysis Josefien Breedvelt; et al. Frontiers in Psychiatry, April 2019.
Meditation-based programs help reduce symptoms of depression, anxiety and stress among college students, researchers find after analyzing the results of 24 research studies conducted in various parts of North America, Asia and Europe.
Reductions were “moderate,” researchers write. They warn, however, that the results of their meta-analysis should be interpreted with caution considering studies varied in quality.
A total of 1,373 college students participated in the 24 studies. Students practiced meditation, yoga or mindfulness an average of 153 minutes a week for about seven weeks. Most programs were provided in a group setting.
Although the researchers do not specify which types of mindfulness, yoga or meditation training students received, they note that the most commonly offered mindfulness program is Mindfulness-Based Stress Reduction and that a frequently practiced form of yoga is Hatha Yoga .
Meta-Analytic Evaluation of Stress Reduction Interventions for Undergraduate and Graduate Students Miryam Yusufov; et al. International Journal of Stress Management, May 2019.
After examining six types of stress-reduction programs common on college campuses, researchers determined all were effective at reducing stress or anxiety among students — and some helped with both stress and anxiety.
Programs focusing on cognitive-behavioral therapy , coping skills and building social support networks were more effective in reducing stress. Meanwhile, relaxation training, mindfulness-based stress reduction and psychoeducation were more effective in reducing anxiety.
The authors find that all six program types were equally effective for undergraduate and graduate students.
The findings are based on an analysis of 43 studies dated from 1980 to 2015, 30 of which were conducted in the U.S. The rest were conducted in Australia, China, India, Iran, Japan, Jordan, Kora, Malaysia or Thailand. A total of 4,400 students participated.
Building an inclusive environment
Cultural Adaptations and Therapist Multicultural Competence: Two Meta-Analytic Reviews Alberto Soto; et al. Journal of Clinical Psychology, August 2018.
If racial and ethnic minorities believe their therapist understands their background and culture, their treatment tends to be more successful, this analysis suggests.
“The more a treatment is tailored to match the precise characteristics of a client, the more likely that client will engage in treatment, remain in treatment, and experience improvement as a result of treatment,” the authors write.
Researchers analyzed the results of 15 journal articles and doctoral dissertations that examine therapists’ cultural competence . Nearly three-fourths of those studies were written or published in 2010 or later. Together, the findings represent the experiences of 2,640 therapy clients, many of whom were college students. Just over 40% of participants were African American and 32% were Hispanic or Latino.
The researchers note that they find no link between therapists’ ratings of their own level of cultural competence and client outcomes.
Internet-based interventions
Internet Interventions for Mental Health in University Students: A Systematic Review and Meta-Analysis Mathias Harrer; et al. International Journal of Methods in Psychiatric Research, June 2019.
Internet-based mental health programs can help reduce stress and symptoms of anxiety, depression and eating disorders among college students, according to an analysis of 48 research studies published or written before April 30, 2018 on the topic.
All 48 studies were randomized, controlled trials of mental health interventions that used the internet to engage with students across various platforms and devices, including mobile phones and apps. In total, 10,583 students participated in the trials.
“We found small effects on depression, anxiety, and stress symptoms, as well as moderate‐sized effects on eating disorder symptoms and students’ social and academic functioning,” write the authors, who conducted the meta-analysis as part of the World Mental Health International College Student Initiative .
The analysis indicates programs that focus on cognitive behavioral therapy “were superior to other types of interventions.” Also, programs “of moderate length” — one to two months – were more effective.
The researchers note that studies of programs targeting depression showed better results when students were not compensated for their participation, compared to studies in which no compensation was provided. The researchers do not offer possible explanations for the difference in results or details about the types of compensation offered to students.
About The Author

Denise-Marie Ordway
Library Resources for ACC Values & Theory of Change: Meet Basic Needs
- Start Strong
- Enroll Full Time
Meet Basic Needs
- Culture of Belonging & Connection
- Suggest Resources
It takes a lot of courage for a parent who is working and raising a family to decide to enroll in college for a better life. The vast majority of ACC students are working and attending college. Approximately 60 percent say they worry about paying for college, and 30 percent are parents. When we help our students meet their basic needs (food, housing, child care, transportation, and mental health), they can better focus on learning. Read more about ACC's Theory of Change .
Books and eBooks from ACC Libraries

Articles from ACC Library Services
- The Campus Housing Crisis
- A Decade of College Student Hunger: What We Know and Where We Need to Go
- A Surprising Reason Preventing Some Students From Finishing College: Lack of Transportation
- I Was a Low-Income College Student. Classes Weren't the Hard Part.
Videos from ACC Databases

Hiding in Plain Sight
Sign into Kanopy with your ACC eID and password

Autism Goes to College

The Graduates/Los Graduados

Other Videos
How this college inspires hope in single moms.
How Can We Solve the College Student Mental Health Crisis? | Dr. Tim Bono
What Happens When College Students Can't Afford to Eat?
The Invisible Battle: College Student Opens Up About Depression and Anxiety
Mental Health for College Students: Learning to Speak Up!
Many College Students are Hungry and Homeless
Other Resources

- << Previous: Enroll Full Time
- Next: Culture of Belonging & Connection >>
- Last Updated: Aug 30, 2024 11:39 AM
- URL: https://researchguides.austincc.edu/ToC-Values
Here’s how you know
- U.S. Department of Health and Human Services
- National Institutes of Health
Meditation and Mindfulness: Effectiveness and Safety

.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} What are meditation and mindfulness?
Meditation has a history that goes back thousands of years, and many meditative techniques began in Eastern traditions. The term “meditation” refers to a variety of practices that focus on mind and body integration and are used to calm the mind and enhance overall well-being. Some types of meditation involve maintaining mental focus on a particular sensation, such as breathing, a sound, a visual image, or a mantra, which is a repeated word or phrase. Other forms of meditation include the practice of mindfulness, which involves maintaining attention or awareness on the present moment without making judgments.
Programs that teach meditation or mindfulness may combine the practices with other activities. For example, mindfulness-based stress reduction is a program that teaches mindful meditation, but it also includes discussion sessions and other strategies to help people apply what they have learned to stressful experiences. Mindfulness-based cognitive therapy integrates mindfulness practices with aspects of cognitive behavioral therapy.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Are meditation and mindfulness practices safe?
Meditation and mindfulness practices usually are considered to have few risks. However, few studies have examined these practices for potentially harmful effects, so it isn’t possible to make definite statements about safety.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} More
A 2020 review examined 83 studies (a total of 6,703 participants) and found that 55 of those studies reported negative experiences related to meditation practices. The researchers concluded that about 8 percent of participants had a negative effect from practicing meditation, which is similar to the percentage reported for psychological therapies. The most commonly reported negative effects were anxiety and depression. In an analysis limited to 3 studies (521 participants) of mindfulness-based stress reduction programs, investigators found that the mindfulness practices were not more harmful than receiving no treatment.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} How popular are meditation and mindfulness?
According to the National Health Interview Survey, an annual nationally representative survey, the percentage of U.S. adults who practiced meditation more than doubled between 2002 and 2022, from 7.5 to 17.3 percent. Of seven complementary health approaches for which data were collected in the 2022 survey, meditation was the most popular, beating out yoga (used by 15.8 percent of adults), chiropractic care (11.0 percent), massage therapy (10.9 percent), guided imagery/progressive muscle relaxation (6.4 percent), acupuncture (2.2 percent), and naturopathy (1.3 percent).
For children aged 4 to 17 years, data are available for 2017; in that year, 5.4 percent of U.S. children used meditation.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Why do people practice mindfulness meditation?
In a 2012 U.S. survey, 1.9 percent of 34,525 adults reported that they had practiced mindfulness meditation in the past 12 months. Among those responders who practiced mindfulness meditation exclusively, 73 percent reported that they meditated for their general wellness and to prevent diseases, and most of them (approximately 92 percent) reported that they meditated to relax or reduce stress. In more than half of the responses, a desire for better sleep was a reason for practicing mindfulness meditation.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} What are the health benefits of meditation and mindfulness?
Meditation and mindfulness practices may have a variety of health benefits and may help people improve the quality of their lives. Recent studies have investigated if meditation or mindfulness helps people manage anxiety, stress, depression, pain, or symptoms related to withdrawal from nicotine, alcohol, or opioids.
Other studies have looked at the effects of meditation or mindfulness on weight control or sleep quality.
However, much of the research on these topics has been preliminary or not scientifically rigorous. Because the studies examined many different types of meditation and mindfulness practices, and the effects of those practices are hard to measure, results from the studies have been difficult to analyze and may have been interpreted too optimistically.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Stress, Anxiety, and Depression
- A 2018 NCCIH-supported analysis of 142 groups of participants with diagnosed psychiatric disorders such as anxiety or depression examined mindfulness meditation approaches compared with no treatment and with established evidence-based treatments such as cognitive behavioral therapy and antidepressant medications. The analysis included more than 12,000 participants, and the researchers found that for treating anxiety and depression, mindfulness-based approaches were better than no treatment at all, and they worked as well as the evidence-based therapies.
- A 2021 analysis of 23 studies (1,815 participants) examined mindfulness-based practices used as treatment for adults with diagnosed anxiety disorders. The studies included in the analysis compared the mindfulness-based interventions (alone or in combination with usual treatments) with other treatments such cognitive behavioral therapy, psychoeducation, and relaxation. The analysis showed mixed results for the short-term effectiveness of the different mindfulness-based approaches. Overall, they were more effective than the usual treatments at reducing the severity of anxiety and depression symptoms, but only some types of mindfulness approaches were as effective as cognitive behavioral therapy. However, these results should be interpreted with caution because the risk of bias for all of the studies was unclear. Also, the few studies that followed up with participants for periods longer than 2 months found no long-term effects of the mindfulness-based practices.
- A 2019 analysis of 23 studies that included a total of 1,373 college and university students looked at the effects of yoga, mindfulness, and meditation practices on symptoms of stress, anxiety, and depression. Although the results showed that all the practices had some effect, most of the studies included in the review were of poor quality and had a high risk of bias.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} High Blood Pressure
Few high-quality studies have examined the effects of meditation and mindfulness on blood pressure. According to a 2017 statement from the American Heart Association, the practice of meditation may have a possible benefit, but its specific effects on blood pressure have not been determined.
- A 2020 review of 14 studies (including more than 1,100 participants) examined the effects of mindfulness practices on the blood pressure of people who had health conditions such as hypertension, diabetes, or cancer. The analysis showed that for people with these health conditions, practicing mindfulness-based stress reduction was associated with a significant reduction in blood pressure.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Pain
Studies examining the effects of mindfulness or meditation on acute and chronic pain have produced mixed results.
- A 2020 report by the Agency for Healthcare Research and Quality concluded that mindfulness-based stress reduction was associated with short-term (less than 6 months) improvement in low-back pain but not fibromyalgia pain.
- A 2020 NCCIH-supported analysis of five studies of adults using opioids for acute or chronic pain (with a total of 514 participants) found that meditation practices were strongly associated with pain reduction.
- Acute pain, such as pain from surgery, traumatic injuries, or childbirth, occurs suddenly and lasts only a short time. A 2020 analysis of 19 studies examined the effects of mindfulness-based therapies for acute pain and found no evidence of reduced pain severity. However, the same analysis found some evidence that the therapies could improve a person’s tolerance for pain.
- A 2017 analysis of 30 studies (2,561 participants) found that mindfulness meditation was more effective at decreasing chronic pain than several other forms of treatment. However, the studies examined were of low quality.
- A 2019 comparison of treatments for chronic pain did an overall analysis of 11 studies (697 participants) that evaluated cognitive behavioral therapy, which is the usual psychological intervention for chronic pain; 4 studies (280 participants) that evaluated mindfulness-based stress reduction; and 1 study (341 participants) of both therapies. The comparison found that both approaches were more effective at reducing pain intensity than no treatment, but there was no evidence of any important difference between the two approaches.
- A 2019 review found that mindfulness-based approaches did not reduce the frequency, length, or pain intensity of headaches. However, the authors of this review noted that their results are likely imprecise because only five studies (a total of 185 participants) were included in the analysis, and any conclusions made from the analysis should be considered preliminary.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Insomnia and Sleep Quality
Mindfulness meditation practices may help reduce insomnia and improve sleep quality.
- A 2019 analysis of 18 studies (1,654 total participants) found that mindfulness meditation practices improved sleep quality more than education-based treatments. However, the effects of mindfulness meditation approaches on sleep quality were no different than those of evidence-based treatments such as cognitive behavioral therapy and exercise.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Substance Use Disorder
Several clinical trials have investigated if mindfulness-based approaches such as mindfulness-based relapse prevention (MBRP) might help people recover from substance use disorders. These approaches have been used to help people increase their awareness of the thoughts and feelings that trigger cravings and learn ways to reduce their automatic reactions to those cravings.
- A 2018 review of 37 studies (3,531 total participants) evaluated the effectiveness of several mindfulness-based approaches to substance use disorder treatment and found that they significantly decreased participants’ craving levels. The mindfulness-based practices were slightly better than other therapies at promoting abstinence from substance use.
- A 2017 analysis specifically focused on MBRP examined 9 studies (901 total participants) of this approach. The analysis concluded that MBRP was not more effective at preventing substance use relapses than other treatments such as health education and cognitive behavioral therapy. However, MBRP did slightly reduce cravings and symptoms of withdrawal associated with alcohol use disorders.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Post-Traumatic Stress Disorder
Studies have suggested that meditation and mindfulness may help reduce symptoms of post-traumatic stress disorder (PTSD).
- A 2018 review supported by NCCIH examined the effects of meditation (in 2 studies, 179 total participants) and other mindfulness-based practices (in 6 studies, 332 total participants) on symptoms of PTSD. Study participants included veterans, nurses, and people who experienced interpersonal violence. Six of the eight studies reported that participants had a reduction of PTSD symptoms after receiving some form of mindfulness-based treatment.
- A 2018 clinical trial funded by the U.S. Department of Defense compared the effectiveness of meditation, health education, and prolonged exposure therapy, a widely accepted treatment for PTSD recommended by the American Psychological Association. Prolonged exposure therapy helps people reduce their PTSD symptoms by teaching them to gradually remember traumatic memories, feelings, and situations. The study included 203 veterans with PTSD as a result of their active military service. The results of the study showed that meditation was as effective as prolonged exposure therapy at reducing PTSD symptoms and depression, and it was more effective than PTSD health education. The veterans who used meditation also showed improvement in mood and overall quality of life.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Cancer
Mindfulness-based approaches may improve the mental health of people with cancer.
- A 2019 analysis of 29 studies (3,274 total participants) of mindfulness-based practices showed that use of mindfulness practices among people with cancer significantly reduced psychological distress, fatigue, sleep disturbance, pain, and symptoms of anxiety and depression. However, most of the participants were women with breast cancer, so the effects may not be similar for other populations or other types of cancer.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Weight Control and Eating Behavior
Studies have suggested possible benefits of meditation and mindfulness programs for losing weight and managing eating behaviors.
- A 2017 review of 15 studies (560 total participants) looked at the effects of mindfulness-based practices on the mental and physical health of adults with obesity or who were overweight. The review found that these practices were very effective methods for managing eating behaviors but less effective at helping people lose weight. Mindfulness-based approaches also helped participants manage symptoms of anxiety and depression.
- A 2018 analysis of 19 studies (1,160 total participants) found that mindfulness programs helped people lose weight and manage eating-related behaviors such as binge, emotional, and restrained eating. The results of the analysis showed that treatment programs, such as mindfulness-based stress reduction and mindfulness-based cognitive therapy, that combine formal meditation and mindfulness practices with informal mindfulness exercises were especially effective methods for losing weight and managing eating.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Attention-Deficit Hyperactivity Disorder
Several studies have been done on using meditation and mindfulness practices to improve symptoms of attention-deficit hyperactivity disorder (ADHD). However, the studies have not been of high quality and the results have been mixed, so evidence that meditation or mindfulness approaches will help people manage symptoms of ADHD is not conclusive.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} How do meditation and mindfulness work?
Some research suggests that meditation and mindfulness practices may affect the functioning or structure of the brain. Studies have used various methods of measuring brain activity to look for measurable differences in the brains of people engaged in mindfulness-based practices. Other studies have theorized that training in meditation and mindfulness practices can change brain activity. However, the results of these studies are difficult to interpret, and the practical implications are not clear.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} NCCIH-Funded Research
NCCIH supports a variety of meditation and mindfulness studies, including:
- An evaluation of how the brain responds to the use of mindfulness meditation as part of a combined treatment for migraine pain.
- A study of the effectiveness of mindfulness therapy and medication (buprenorphine) as a treatment for opioid use disorder.
- A study of a mindfulness training program designed to help law enforcement officers improve their mental health by managing stress and increasing resilience.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Tips To Consider
- Don’t use meditation or mindfulness to replace conventional care or as a reason to postpone seeing a health care provider about a medical problem.
- Ask about the training and experience of the instructor of the meditation or mindfulness practice you are considering.
- Take charge of your health—talk with your health care providers about any complementary health approaches you use. Together, you can make shared, well-informed decisions
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} For More Information
Nccih clearinghouse.
The NCCIH Clearinghouse provides information on NCCIH and complementary and integrative health approaches, including publications and searches of Federal databases of scientific and medical literature. The Clearinghouse does not provide medical advice, treatment recommendations, or referrals to practitioners.
Toll-free in the U.S.: 1-888-644-6226
Telecommunications relay service (TRS): 7-1-1
Website: https://www.nccih.nih.gov
Email: [email protected] (link sends email)
Know the Science
NCCIH and the National Institutes of Health (NIH) provide tools to help you understand the basics and terminology of scientific research so you can make well-informed decisions about your health. Know the Science features a variety of materials, including interactive modules, quizzes, and videos, as well as links to informative content from Federal resources designed to help consumers make sense of health information.
Explaining How Research Works (NIH)
Know the Science: How To Make Sense of a Scientific Journal Article
Understanding Clinical Studies (NIH)
A service of the National Library of Medicine, PubMed® contains publication information and (in most cases) brief summaries of articles from scientific and medical journals. For guidance from NCCIH on using PubMed, see How To Find Information About Complementary Health Approaches on PubMed .
Website: https://pubmed.ncbi.nlm.nih.gov/
NIH Clinical Research Trials and You
The National Institutes of Health (NIH) has created a website, NIH Clinical Research Trials and You, to help people learn about clinical trials, why they matter, and how to participate. The site includes questions and answers about clinical trials, guidance on how to find clinical trials through ClinicalTrials.gov and other resources, and stories about the personal experiences of clinical trial participants. Clinical trials are necessary to find better ways to prevent, diagnose, and treat diseases.
Website: https://www.nih.gov/health-information/nih-clinical-research-trials-you
Research Portfolio Online Reporting Tools Expenditures & Results (RePORTER)
RePORTER is a database of information on federally funded scientific and medical research projects being conducted at research institutions.
Website: https://reporter.nih.gov
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Key References
- Anheyer D, Leach MJ, Klose P, et al. Mindfulness-based stress reduction for treating chronic headache: a systematic review and meta-analysis . Cephalalgia . 2019;39(4):544-555.
- Black LI, Barnes PM, Clarke TC, Stussman BA, Nahin RL. Use of yoga, meditation, and chiropractors among U.S. children aged 4–17 years . NCHS Data Brief, no 324. Hyattsville, MD: National Center for Health Statistics. 2018.
- Breedvelt JJF, Amanvermez Y, Harrer M, et al. The effects of meditation, yoga, and mindfulness on depression, anxiety, and stress in tertiary education students: a meta-analysis . Frontiers in Psychiatry . 2019;10:193.
- Burke A, Lam CN, Stussman B, et al. Prevalence and patterns of use of mantra, mindfulness and spiritual meditation among adults in the United States . BMC Complementary and Alternative Medicine. 2017;17(1):316.
- Carrière K, Khoury B, Günak MM, et al. Mindfulness‐based interventions for weight loss: a systematic review and meta‐analysis . Obesity Reviews . 2018;19(2):164-177.
- Cavicchioli M, Movalli M, Maffei C. The clinical efficacy of mindfulness-based treatments for alcohol and drugs use disorders: a meta-analytic review of randomized and nonrandomized controlled trials . European Addiction Research . 2018;24(3):137-162.
- Cillessen L, Johannsen M, Speckens AEM, et al. Mindfulness‐based interventions for psychological and physical health outcomes in cancer patients and survivors: a systematic review and meta‐analysis of randomized controlled trials . Psychooncology . 2019;28(12):2257-2269.
- Creswell JD. Mindfulness interventions . Annual Review of Psychology. 2017;68:491-516.
- Davidson RJ, Kaszniak AW. Conceptual and methodological issues in research on mindfulness and meditation . American Psychologist. 2015;70(7):581-592.
- Farias M, Maraldi E, Wallenkampf KC, et al. Adverse events in meditation practices and meditation-based therapies: a systematic review . Acta Psychiatrica Scandinavica. 2020;142(5):374-393.
- Garland EL, Brintz CE, Hanley AW, et al. Mind-body therapies for opioid-treated pain: a systematic review and meta-analysis . JAMA Internal Medicine . 2020;180(1):91-105.
- Goldberg SB, Tucker RP, Greene PA, et al. Mindfulness-based interventions for psychiatric disorders: a systematic review and meta-analysis . Clinical Psychology Review . 2018;59:52-60.
- Grant S, Colaiaco B, Motala A, et al. Mindfulness-based relapse prevention for substance use disorders: a systematic review and meta-analysis . Journal of Addiction Medicine . 2017;11(5):386-396.
- Haller H, Breilmann P, Schröter M et al. A systematic review and meta‑analysis of acceptance and mindfulness‑based interventions for DSM‑5 anxiety disorders . Scientific Reports . 2021;11(1):20385.
- Hilton L, Hempel S, Ewing BA, et al. Mindfulness meditation for chronic pain: systematic review and meta-analysis . Annals of Behavioral Medicine. 2017;51(2):199-213.
- Hirshberg MJ, Goldberg SB, Rosenkranz M, et al. Prevalence of harm in mindfulness-based stress reduction . Psychological Medicine. August 18, 2020. [Epub ahead of print].
- Intarakamhang U, Macaskill A, Prasittichok P. Mindfulness interventions reduce blood pressure in patients with non-communicable diseases: a systematic review and meta-analysis . Heliyon. 2020;6(4):e03834.
- Khoo E-L, Small R, Cheng W, et al. Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: a systematic review and network meta-analysis . Evidence-Based Mental Health. 2019;22(1):26-35.
- Levine GN, Lange RA, Bairey-Merz CN, et al. Meditation and cardiovascular risk reduction: a scientific statement from the American Heart Association . Journal of the American Heart Association. 2017;6(10):e002218.
- Nidich S, Mills PJ, Rainforth M, et al. Non-trauma-focused meditation versus exposure therapy in veterans with post-traumatic stress disorder: a randomised controlled trial . Lancet Psychiatry . 2018;5(12):975-986.
- Niles BL, Mori DL, Polizzi C, et al. A systematic review of randomized trials of mind-body interventions for PTSD . Journal of Clinical Psychology . 2018;74(9):1485-1508.
- Rogers JM, Ferrari M, Mosely K, et al. Mindfulness-based interventions for adults who are overweight or obese: a meta-analysis of physical and psychological health outcomes . Obesity Reviews . 2017;18(1):51-67.
- Rosenkranz MA, Dunne JD, Davidson RJ. The next generation of mindfulness-based intervention research: what have we learned and where are we headed? Current Opinion in Psychology. 2019;28:179-183.
- Rusch HL, Rosario M, Levison LM, et al. The effect of mindfulness meditation on sleep quality: a systematic review and meta-analysis of randomized controlled trials . Annals of the New York Academy of Sciences . 2019;1445(1):5-16.
- Schell LK, Monsef I, Wöckel A, et al. Mindfulness-based stress reduction for women diagnosed with breast cancer. Cochrane Database of Systematic Reviews. 2019;3(3):CD011518. Accessed at cochranelibrary.com on June 3, 2022.
- Semple RJ, Droutman V, Reid BA. Mindfulness goes to school: things learned (so far) from research and real-world experiences . Psychology in the Schools. 2017;54(1):29-52.
- Shires A, Sharpe L, Davies JN, et al. The efficacy of mindfulness-based interventions in acute pain: a systematic review and meta-analysis . Pain . 2020;161(8):1698-1707.
- Van Dam NT, van Vugt MK, Vago DR, et al. Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation . Perspectives on Psychological Science. 2018;13(1):36-61.
.header_greentext{color:green!important;font-size:24px!important;font-weight:500!important;}.header_bluetext{color:blue!important;font-size:18px!important;font-weight:500!important;}.header_redtext{color:red!important;font-size:28px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;font-size:28px!important;font-weight:500!important;}.header_purpletext{color:purple!important;font-size:31px!important;font-weight:500!important;}.header_yellowtext{color:yellow!important;font-size:20px!important;font-weight:500!important;}.header_blacktext{color:black!important;font-size:22px!important;font-weight:500!important;}.header_whitetext{color:white!important;font-size:22px!important;font-weight:500!important;}.header_darkred{color:#803d2f!important;}.Green_Header{color:green!important;font-size:24px!important;font-weight:500!important;}.Blue_Header{color:blue!important;font-size:18px!important;font-weight:500!important;}.Red_Header{color:red!important;font-size:28px!important;font-weight:500!important;}.Purple_Header{color:purple!important;font-size:31px!important;font-weight:500!important;}.Yellow_Header{color:yellow!important;font-size:20px!important;font-weight:500!important;}.Black_Header{color:black!important;font-size:22px!important;font-weight:500!important;}.White_Header{color:white!important;font-size:22px!important;font-weight:500!important;} Other References
- American Academy of Pediatrics Section on Integrative Medicine. Mind-body therapies in children and youth. Pediatrics . 2016;138(3):e20161896.
- Coronado-Montoya S, Levis AW, Kwakkenbos L, et al. Reporting of positive results in randomized controlled trials of mindfulness-based mental health interventions. PLoS One . 2016;11(4):e0153220.
- Dakwar E, Levin FR. The emerging role of meditation in addressing psychiatric illness, with a focus on substance use disorders. Harvard Review of Psychiatry . 2009;17(4):254-267.
- Goyal M, Singh S, Sibinga EMS, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Internal Medicine. 2014;174(3):357-368.
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research . Washington, DC: National Academies Press; 2011.
- Kabat-Zinn J, Massion AO, Kristeller J, et al. Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. American Journal of Psychiatry. 1992;149(7):936-943.
- Ludwig DS, Kabat-Zinn J. Mindfulness in medicine. JAMA. 2008;300(11):1350-1352.
- McKeering P, Hwang Y-S. A systematic review of mindfulness-based school interventions with early adolescents. Mindfulness . 2019;10:593-610.
- Muratori P, Conversano C, Levantini V, et al. Exploring the efficacy of a mindfulness program for boys with attention-deficit hyperactivity disorder and oppositional defiant disorder. Journal of Attention Disorders . 2021;25(11):1544-1553.
- Nahin RL, Rhee A, Stussman B. Use of complementary health approaches overall and for pain management by US adults. JAMA. 2024;331(7):613-615.
- Poissant H, Mendrek A, Talbot N, et al. Behavioral and cognitive impacts of mindfulness-based interventions on adults with attention-deficit hyperactivity disorder: a systematic review. Behavioural Neurology . 2019;2019:5682050.
- Skelly AC, Chou R, Dettori JR, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update. Comparative Effectiveness Review no. 227. Rockville, MD: Agency for Healthcare Research and Quality; 2020. AHRQ publication no. 20-EHC009.
- Stieger JR, Engel S, Jiang H, et al. Mindfulness improves brain–computer interface performance by increasing control over neural activity in the alpha band. Cerebral Cortex . 2021;31(1):426-438.
- Teasdale JD, Segal ZV, Williams JMG, et al. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and Clinical Psychology . 2000;68(4):615-623.
- Weng HY, Lewis-Peacock JA, Hecht FM, et al. Focus on the breath: brain decoding reveals internal states of attention during meditation. Frontiers in Human Neuroscience . 2020;14:336.
- Yoshida K, Takeda K, Kasai T, et al. Focused attention meditation training modifies neural activity and attention: longitudinal EEG data in non-meditators. Social Cognitive and Affective Neuroscience . 2020;15(2):215-223.
- Yuan JP, Connolly CG, Henje E, et al. Gray matter changes in adolescents participating in a meditation training. Frontiers in Human Neuroscience . 2020;14:319.
- Zhang J, Díaz-Román A, Cortese S. Meditation-based therapies for attention-deficit/hyperactivity disorder in children, adolescents and adults: a systematic review and meta-analysis. Evidence-Based Mental Health . 2018;21(3):87-94.
Acknowledgments
Thanks to Elizabeth Ginexi, Ph.D., Erin Burke Quinlan, Ph.D., and David Shurtleff, Ph.D., NCCIH, for their review of this 2022 publication.
This publication is not copyrighted and is in the public domain. Duplication is encouraged.
NCCIH has provided this material for your information. It is not intended to substitute for the medical expertise and advice of your health care provider(s). We encourage you to discuss any decisions about treatment or care with your health care provider. The mention of any product, service, or therapy is not an endorsement by NCCIH.
Related Topics
Pain: Considering Complementary Approaches (eBook)
For Consumers
8 Things to Know About Meditation and Mindfulness
For Health Care Providers
Use of Yoga, Meditation, and Chiropractic by Adults and Children
Mind and Body Approaches for Chronic Pain
Meditation - Systematic Reviews/Reviews/Meta-analyses (PubMed®)
Meditation - Randomized Controlled Trials (PubMed®)
Research Results
National Survey Reveals Increased Use of Yoga, Meditation, and Chiropractic Care Among U.S. Adults
National Survey Reveals Increased Use of Yoga and Meditation Among U.S. Children
Mindfulness-Based Stress Reduction, Cognitive-Behavioral Therapy Shown To Be Cost Effective for Chronic Low-Back Pain
News Details
Jacqueline Corcoran publishes “Your Child’s Mental Health Diagnosis”

Authored by: Carson Easterly
Faculty & Research
New book by SP2’s Doctorate in Clinical Social Work Program director described as “go-to guide for those raising children with mental disorders”
According to the National Institutes of Health, 20 percent of youth ages three to seventeen in the United States have a mental, emotional, developmental, or behavioral disorder, and mental health challenges were the leading cause of death and disability in the age group. Suicidal behaviors among high school students also increased more than 40 percent in the decade before 2019.
Responding to this troubling landscape, the book “ Your Child’s Mental Health Diagnosis: A Comprehensive and Compassionate Guide for Parents ” by Dr. Jacqueline Corcoran provides valuable information, support, and strategies for parents navigating their children’s mental health conditions and emotional well-being.
“I have clinical experience and lived experience with this subject, and I have worked with many children and their families,” says Corcoran, a professor at Penn’s School of Social Policy & Practice (SP2) who is also a private practice psychotherapist. “Not surprisingly, youth mental health evolved as a scholarship interest of mine, and I’ve done many systematic reviews on disorders and well-being.”
Rowman & Littlefield published the book in June 2024, describing it as “an empathetic guide backed by up-to-date research” with several facets:
- Draws back the curtain on how diagnoses are determined in the U.S. and both the limits and benefits of labels
- Addresses the overwhelming emotions parents may feel when witnessing their child suffer and emphasizes the importance of parents looking after their own mental health and relationships
- Provides comprehensive information about each condition’s symptoms, frequently co-occurring disorders, contributory factors, evidence-based treatments, medication options, working with your child’s school, and parents’ own insights
Corcoran hopes to address a gap between diagnosis and support. She says, “Fifty percent of youth with a disorder don’t get needed treatment, so my hope with this book is to reach parents who are struggling to help their children and provide them with information, support, and resources.”
Corcoran has been a master’s level social worker for over 33 years and has enjoyed 25 years of productive academic scholarship. She is director of the Doctorate in Clinical Social Work (DSW) Program at Penn’s School of Social Policy & Practice and has written 18 books and over 100 journal articles and book chapters. Corcoran was the first person in social work to publish a book on evidence-based practice, “Evidence-Based Social Work Practice with Families,” which she wrote in 2000 as an assistant professor. Her areas of scholarship include adult and youth mental health, and her methodological specialty involves systematic reviews. Corcoran is committed to continuing the compilation of knowledge to further the evidence basis of social work with the mission of bringing relevant services to oppressed and vulnerable people.

Jacqueline Corcoran, PhD
office: 703.405.3254
fax: 215.573.2099
cojacq@upenn.edu

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Health Research Alliance Author Manuscripts
School Mental Health Is Not Just for Students: Why Teacher and School Staff Wellness Matters
Workplace stress.
The term “school mental health” is typically used to discuss the mental health and wellness of students. However, school mental health also includes promoting the well-being of school-based educators, administrators, and mental health workers. Although the workplace wellness literature predominantly focuses on health-related programs to support well-being in more traditional business settings, it offers foundational knowledge for the emerging school staff wellness field. Experiencing significant levels of stress in the workplace is common not only in schools, but in a wide array of work settings. According to the American Psychological Association’s annual Stress in America survey, 60% of individuals residing in the United States in 2014 reported that work was a top source of stress in their lives ( APA, 2015 ). Further, the APA’s Center for Organization Excellence found that approximately 33% of Americans reported having chronic work stress ( APA, 2013 ). This is a concerning statistic, because stress-related disorders are costly for employers (e.g., through absenteeism and lost productivity; DHHS, 1999 ) and are associated with numerous negative mental and physical health outcomes for workers ( APA, 2015 ). Although all stress cannot be eliminated in the workplace, research has documented some best practices and strategies that can help reduce the extent and impact of stress.
Eighty-nine percent said they had been enthusiastic about teaching when they started the profession, but only 15% reported being enthusiastic at the time they completed the survey.
Work-Related Stress for Educators
Individuals working in school settings are particularly vulnerable to work-related stress. Data from the 2013 Gallup-Health-ways Well-Being Index found that 46% of teachers in K-12 settings report high levels of daily stress during the school year. This level of stress is similar to that of nurses (46%) and physicians (45%) and is the highest (along with nurses) among the 14 professional categories included in the study ( Gallup, 2014 ). Furthermore, the American Federation of Teachers (2015) found that 78% of teachers reported feeling physically and emotionally exhausted at the end of the day. The stress that educators experience affects their enthusiasm about the profession and longevity in the field. For example, a survey of 30,000 teachers revealed that 89% said they had been enthusiastic about teaching when they started the profession, but only 15% reported being enthusiastic at the time they completed the survey. The stress of the education field is further illustrated in the high rates of teacher turnover; 10% of teachers leave after one year, and 17% of teachers leave within five years ( Gray & Taie, 2015 ). Turnover rates are much higher in urban districts, where up to 70% of teachers leave within the first year ( Gray & Taie, 2015 ). This issue is not limited just to new teachers; many experienced teachers leave the profession because they feel unable to deal with the myriad challenges of modern teaching ( Byrne, 1998 ; Taylor et al., 2005 ).
There are a multitude of factors contributing to the high rates of stress and burnout in the education field. Studies suggest that some of the most common sources of teacher stress include:
- High-stakes testing;
- Large class sizes;
- Student behavioral challenges;
- Inadequate resources;
- Poor physical space;
- Bureaucracy;
- High responsibility for others;
- Perceived inadequate recognition or advancement; and
- The gap between preservice training expectations and actual work experiences ( Dworkin, 2001 ; Fisher, 2011 ; Kokkinos, 2007 ; Travers & Cooper, 1996 ).
Additionally, lack of autonomy is a significant contributor to teacher burnout and stress; teachers who do not feel that they have autonomy over their classroom or that they have a collective influence over school policy are more likely to experience job dissatisfaction ( Ingersoll, 1996 , 2001 ). Research from the 2012 Gallup Daily Tracking Poll ( Gallup, 2014 ) showed that when compared to 12 different occupational groups, teachers are the least likely to state that they agree with the statement: “At work, my opinions seem to count.”
Educators and other school-based staff can experience the stress of compassion fatigue and/or vicarious traumatization (also known as secondary traumatic stress; Hydon et al., 2015 ), which is defined as “the natural consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other—the stress resulting from helping or wanting to help a traumatized or suffering person” ( Figley, 1993 , as cited in Figley, 1995 , p. 7). Compassion fatigue can be the result of experiencing one traumatic case, or a cumulative impact over time ( Hydon et al., 2015 ). As explained by the National Child Traumatic Stress Network ( NCTSN, 2011 , pp. 2–3): “Any professional who works directly with traumatized children … is at risk of secondary traumatic stress.” Although compassion fatigue has traditionally been discussed as being a secondary effect for individuals providing clinical services to traumatized clients, it also has an impact on teachers and other school staff who work closely with youth who have experienced adverse experiences. The impact of compassion fatigue may be particularly acute for teachers working in poor, underresourced urban and rural communities, where students may have been exposed to community and family violence and traumatic experiences.
Teachers and other school staff who experience exhaustion and burnout related to their work are likely to have a number of negative physical and psychological symptoms and consequences, including:
- Emotional numbing;
- Feeling “shut down”;
- Loss of enjoyment;
- Lack of energy;
- A sense of cynicism or pessimism;
- Increased illness or fatigue;
- Aches and pains;
- Increased absenteeism and “sick days”;
- Greater problems with boundaries; and
- Difficulty making decisions or making poor decisions ( Saakvitne et al., 2000 ).
Educator and school staff stress and burnout affects not only the adult professionals but also the students with whom these professionals interact. For example, teacher burnout is predictive of student academic outcomes, including being correlated with lower levels of student effective learning and lower motivation ( Zhang & Sapp, 2008 ). Additionally, teacher burnout appears to affect the stress levels of the students they teach; a recent study found that teacher burnout level explained more than half of the variability in students’ levels of cortisol (a stress hormone) when evaluated in the morning ( Oberle & Schonert-Reichl, 2016 ).
Despite the strong evidence for the existence of work-related stress, only 36% of respondents from all fields to the APA (2015) Stress in America survey stated that their employers provide the resources they need to effectively manage their work-related stress. The numbers are even weaker in the education field, with only 25.5% of schools offering stress management education to staff ( DHHS, 2015 ). Although comprehensive programs are recommended to address staff wellness, many schools and school systems have limited programs, and school staff may have exposure only to professional development and basic resources. Thus, although school employees throughout the United States are clearly affected by work-related stress, they often lack the programs, resources, and tools needed to support their management of that stress and the promotion of overall wellness. This article demonstrates the value of school staff wellness and highlights unique aspects of the job that should be taken into consideration when addressing the well-being of school-based staff. It shares key findings from the literature and discusses how to best measure and implement effective staff wellness programs in schools. Finally, it summarizes best practices in the school staff wellness field and highlights exemplary programs.
Although school employees throughout the United States are clearly affected by work-related stress, they often lack the programs, resources, and tools needed to support their management of that stress and the promotion of overall wellness.
Employee Wellness Programs
Wellness is defined by the National Wellness Institute as “an active process through which people become aware of, and make choices toward, a more successful existence” ( NWI, n.d. ). Thus, wellness is not merely the absence of illness. NWI explains that among professionals and researchers in the wellness field, there is general agreement that wellness is an evolving and self-directed process in which an individual is working to achieve his/her fullest potential and which may include mental, physical, and/or spiritual well-being. The multidimensional components of wellness vary across different theories of wellness and wellness programs but often include medical, emotional, environmental, occupational, physical, intellectual, spiritual, social, and financial components ( NWI, n.d. ). Despite this multidimensional understanding of wellness, wellness programs in the workplace often focus on only the physical and medical dimensions ( Parks & Steelman, 2008 ).
About 50% of all employers with 50 or more employees in the United States have wellness promotion initiatives ( Mattke et al., 2013 ). Among employers offering a wellness program, the majority focus on nutrition/weight (79%), smoking (77%), or fitness (72%), with about one-half focusing on alcohol/drug abuse (52%) and stress management (52%), and about one-third focusing on health education (36%). Workplace wellness programs generally fall into three categories: (1) screening activities, (2) preventive interventions, and (3) health promotion activities.
Screening activities focus on identifying health risks in employees and may include measuring weight, completing a health risk questionnaire, and taking other biometrics (e.g., cholesterol level). The RAND Employer Survey found that about 65% of employers with wellness programs conduct health risk questionnaires with their employees.
Preventive interventions are programs that are implemented to help employees make positive changes in their health behaviors, such as health education classes, individual health counseling, or step-counting programs. Approximately 77% of employers with a wellness program offer prevention interventions.
Health promotion activities are those that promote healthy lifestyles for all employees, such as offering healthy meals in the cafeteria or providing subsidized gym memberships. These types of activities are present in about 40% of workplaces (including those without a formal employee wellness program). Most employee wellness programs tend to be a combination of these three types of approaches to wellness, with combined screening and intervention approaches being the most common ( Mattke et al., 2013 ).
Impact of Wellness Programs on Employee Outcomes
Although there has been some criticism of wellness programs in the workplace, suggesting that they are ineffective and/or too expensive, a meta-analysis conducted by Parks and Steelman (2008) , found that participation in wellness programs is related to several positive outcomes. Specifically, participation in organizational wellness programs is associated with higher job satisfaction and lower absenteeism. Results of the RAND Employer Survey found that participation in wellness programs was related to greater gains in weight loss, smoking cessation, and exercise, but not to lowered cholesterol levels ( Mattke et al., 2013 ). However, the sample size in the RAND study was small and may have been affected by the specific types of wellness activities employed. Nonetheless, a meta-analysis of occupational stress management programs finds that there is an overall medium to large effect for participation in each individual intervention on a variety of outcomes. Outcomes include improved mental and physical health, decreased anxiety and stress, and an increase in mindfulness ( Richardson & Rothstein, 2008 ).
The model theorizes that by promoting staff health behaviors, employees will improve their health and cognitive performance, which will then affect student health and educational outcomes.
In addition to the physical, social, emotional, and behavioral impacts of wellness programs, there are also economic benefits. Research suggests that participation in a wellness program over five years leads to lower health care costs and decreasing health care use ( Mattke et al., 2013 ). This is relevant because healthcare expenditures are nearly 50% greater for workers who report high levels of stress ( DHHS, 1999 ). A meta-analysis conducted in 2010 found that workplace wellness programs affect medical costs and absenteeism substantially. More specifically, for every $1.00 spent on wellness programs, medical costs fall $3.27 and absenteeism costs fall $2.73 ( Baicker et al., 2010 ). Findings corroborate an earlier meta-analysis that found that employee wellness programs are cost-effective; on average, they achieve a $5.81 to $1.00 return on investment ( Chapman, 2005 ). Chapman’s (2003) review of 42 published worksite health promotion programs showed that companies with effective wellness programs had, on average, a 28% reduction in sick days, a 26% reduction in health costs, and a 30% reduction in workers’ compensation and disability management claims. Results of these comprehensive studies suggest that employee wellness programs are not only helpful for employee wellness and morale, but are also smart financial decisions.
Employee Wellness in Schools
The research literature clearly points to the benefits of quality employee wellness programs. Additionally, educators are in a profession with a uniquely high level of stress and burnout, suggesting that they would benefit from wellness programming. Nonetheless, implementation and evaluation of such programs is low and could benefit from additional studies. To better understand the current state of research on teacher wellness, the current authors conducted a search on PsycINFO for “wellness” and “teacher.” The search found 64 peer-reviewed results published between 1984 and 2015. Although there has been a significant increase in publications recently, especially in the last five years, the school staff wellness topic is still a fairly new area within the mental health literature. The trend in publication numbers suggests that the topic of teacher wellness is only beginning to receive more intensive research attention. The research that has been published to date has focused on a range of subjects, including the relation between teacher wellness and child outcomes (e.g., academic achievement), the role of teacher wellness in promoting child-school connectedness, teacher burnout, teacher efficacy, and the measurement of wellness.
In an effort to better understand the number and types of evidence-based wellness programs for school staff, a search of SAMH-SA’s National Registry of Evidence-based Programs and Practices was conducted using the key word “wellness.” The search yielded 17 programs. Three programs focused on students in grades K through 12, two programs focused on college students, one program focused on students in grades 3 through 12, and the rest focused on other populations, but none specifically targeted school staff. Although there are school wellness programs that target school staff (see MSBR, CARE, and CALM programs discussed below), they do not currently have the number of trials and results needed to be included in the registry, although they are likely to be added in time. Taken together, the results of this literature search suggest that evidence-based teacher and school staff wellness programs have not been widely developed or studied and that there are significant opportunities to expand this field in the future.
Core Wellness Components/Recommended Wellness Standards
Although the research related to evidence-based school staff wellness programs is in its early stages, there are a number of core wellness components and standards that have been established specifically for educator wellness initiatives.
The Coordinated School Health Model.
In 1987, Allensworth and Kolbe greatly influenced the field of school health ( Lohrmann, 2008 ) by creating a comprehensive model of school health called the Coordinated School Health Model. In Allensworth and Kolbe’s (1987) model, there are eight components to school health, which include content areas such as physical education and school health services for students but that go beyond previous models by also emphasizing “school site health promotion of faculty and staff.” The model theorizes that by promoting staff health behaviors, employees will improve their health and cognitive performance, which will then affect student health and educational outcomes ( Lohrmann, 2008 ). The eight-component Coordinated School Health Model has since been adopted and adapted by the Centers for Disease Control and Prevention (CDC).
The Whole School, Whole Community, Whole Child Model.
Currently, the CDC promotes the Whole School, Whole Community, Whole Child (WSCC) Model, which focuses on a 10-component health model with associated student learning objectives. Under this program, the CDC (2014b) states that school employee wellness should include “a coordinated set of programs, policies, benefits, and environmental supports designed to address multiple risk factors [e.g., lack of physical activity, tobacco use] and health conditions [e.g., diabetes, depression] to meet the health and safety needs of all employees.” However, the CDC does not give guidelines about what specifically should be included in school employee wellness programming.
The Healthy Schools Program Framework.
The Alliance for a Healthier Generation, an organization focused on promoting health and wellness for children and adolescents, has created the Healthy Schools Program Framework (HSPF). The HSPF outlines best practices for creating and sustaining a healthy school environment, organizing these practices into bronze, silver, and gold standard tiers ( Alliance for a Healthier Generation, 2016 ). One aspect of this framework focuses on health promotion for school staff. The framework highlights the types of activities and standards that should be implemented in schools to promote staff health at each level (i.e., bronze, silver, gold; see Table 1 for a summary of the HSPF school staff standards). Whereas these HSPF standards provide more specific information about the types of activities to include in employee wellness programming, they are exclusively focused on physical health, including nutrition, exercise, and modeling of healthy behaviors for students rather than a more comprehensive model of employee wellness ( Alliance for a Healthier Generation, 2016 ).
HSPF Standards for Health Promotion for Staff
| Bronze | Silver | Gold |
|---|---|---|
| Health assessments for staff, once per year; Physical activity programs for staff; Modeling of healthy eating and physical activity behaviors through five or more strategies (e.g., encourage staff to eat healthy foods at school, provide information about using physical activity in the classroom) | Meets bronze standards, plus: Uses three or more methods to encourage staff to participate in health promotion programs; Provides staff with free or low-cost healthy eating/weight management programs or classes | Meets silver standards, plus: Follows USDA’s Smart Snacks in School nutrition standards, including at staff meetings and lounge areas |
The DHPE Standard.
The Directors of Health Promotion and Education ( DHPE, 2005 ) created a more comprehensive standard for school employee wellness that is focused solely on staff members. This school employee wellness guide is a comprehensive resource that discusses the need for school employee wellness programs, key principles, steps for establishing a program, funding for programs, as well as useful tools and resources (e.g., Employee Wellness Interest Survey, sample letter of invitation). The DHPE identifies eight different components that should be included in a comprehensive school employee wellness program:
- Health education and health-promoting activities tailored to the needs of employees;
- Safe, supportive social and physical environments;
- Integration of program into the school/district structure;
- Linkage to other related programs (e.g., employee assistance programs);
- Worksite screening programs and follow-up care as needed;
- Individualized interventions to support employee behavior change;
- Education focused on helping employees make health care decisions; and
- An evaluation and improvement process to help the programs improve their effectiveness ( DHPE, 2005 ).
This eight-component model focuses on more than just increasing nutrition and exercise in employees and emphasizes the importance of creating safe environments, promoting education, individualizing interventions, and evaluating programming to ensure that it is working. See Table 2 for a review of these eight components and examples of programs/activities that address each component. A model that fulfills these DHPE guidelines is a gold standard of programming, but implementing such a comprehensive model requires an effective implementation process; it is recommended that individuals and organizations that hope to begin this type of program follow the nine-step implementation process outlined by DHPE (2005) .
Components of a Comprehensive School Employee Wellness Program
| Component | Sample Activities |
|---|---|
| 1. Health education and health-promoting activities tailored to the needs of employees | Workshops or school-sponsored activities focused on employee-desired skill development or lifestyle behavior change |
| 2. Safe, supportive social and physical environments | School sets expectations for healthy behaviors and implements policies to promote health and reduce risk of disease |
| 3. Integration of program into the school/district structure | Provide time for employees to attend workshops and activities; provide incentives to participate in wellness programs |
| 4. Linkage to other related programs | Linkages to employee assistance programs or programs aimed at helping employees balance work and family life |
| 5. Worksite screening programs and follow-up care as needed | Screening programs linked to employee’s medical care so participation and follow-up treatments are seamless |
| 6. Individualized interventions to support employee behavior change | Individual health counseling or step-counting programs |
| 7. Education focused on helping employees make health care decisions | Health education classes related to topics such as weight loss, diabetes, and healthy heart management |
| 8. Evaluation and improvement process | Collect data before, during, and after program implementation. Data collection can include cost, compliance, and outcome measures. |
Source: Adapted from DHPE (2005) and Partnership for Prevention (2010) .
Validated Wellness Measures
In order to develop and implement teacher and school staff wellness programs, it is important to gather data on staff wellness before, during, and after program implementation. Validated measures of wellness can help to assess staff needs, determine target populations for programs, and measure change in wellness following program participation.
The Interpersonal Mindfulness in Teaching Questionnaire.
The only measure in the literature that was specifically designed to measure wellness in teachers is the Interpersonal Mindfulness in Teaching Questionnaire (IMT; Frank et al., 2016 ). The measure focuses on two distinct factors: (1) teacher intrapersonal mindfulness and (2) teacher interpersonal mindfulness. The measure has been validated through confirmatory factor analysis and has good test-retest reliability for both scales in the medium-large range ( Frank et al., 2016 ).
The Teachers’ Sense of Efficacy Scale.
The Teachers’ Sense of Efficacy Scale (TSES; Tschannen-Moran & Woolfolk-Hoy, 2001 ) is a measure of what teachers view as the most difficult aspects of their teaching activities and how much power they think they have in resolving those challenges. Items ask teachers to indicate “how much they can do” in response to various classrooms and instructional challenges. The questionnaire measures three dimensions: instructional strategies, classroom management, and student engagement.
Results of the study suggested that teacher participants had improvements in self-regulation, self-compassion, mindfulness, and sleep quality.
The Professional Quality of Life Scale.
One validated measure of employee wellness more generally (not specifically for school employees) is the Professional Quality of Life Scale (ProQOL; Hudnall Stamm, 2009 ). Although this measure is not specifically for school staff, it is particularly appropriate for employees in the helping professions because the measure focuses on compassion satisfaction (the positive emotional effect of helping others) and compassion fatigue (burnout and secondary traumatic stress). It is a well-validated, self-report measure of the positive and negative aspects of caring and can be given individually or in groups.
The Worksite Health Score Card.
In addition, the Centers for Disease Control and Prevention ( CDC, 2014a ) offer a Worksite Health Score Card that allows employers to assess their evidence-based health promotion interventions. The program helps to identify gaps in health promotion programs as well as to prioritize high-impact strategies in the program. It is available at no cost to employers.
Exemplary Programs
The curriculums provided as part of wellness programs in many schools are often not evidence based. Little is known about how the stress management education provided in the schools affects teacher or student outcomes. However, evidence indicates that change is possible even in programs of relatively short duration. For example, in a 10-week health promotion program for employees in the Dallas Independent School District, with a focus on exercise and physical fitness, the following impressive improvements were found: 44% of teachers changed their overall lifestyle, 68% changed their diet, 26% who had not exercised began vigorous programs, and 18% quit smoking. Overall, this program led to 1.25 days less of absenteeism for those teachers who were exercising. This is equal to a savings of $149,578 for the district ( DHPE, 2005 ).
There are several comprehensive teacher wellness programs that are setting the foundation for school staff wellness research. The following programs have been studied for evidence of effectiveness and have shown some promising results.
Washoe County School District (Nevada) Wellness Program.
The Washoe County School District started an optional wellness program for its 6,246 employees, which was evaluated over a two-year period ( Aldana et al., 2005 ). The program was aimed at reducing two-year health care costs and absenteeism. When considering (as covariates in statistical analyses) baseline health claims, absenteeism in three years prior, age, gender, job classification, and years in school district, the program found no significant differences in direct health care costs. However, there were significant differences in absenteeism. Participants had an average of three fewer missed days than non-participants, which equals a cost saving of $15.60 for every dollar spent on the program.
Mindfulness-Based Stress Reduction (MBSR).
MBSR is a mindfulness training that is shown to reduce stress, depression, and anxiety. It was created to address chronic pain but is useful for a variety of physical and mental health problems. MBSR is included in SAMSHA’s National Registry of Evidence-based Programs and Practices. Two different research groups have adapted MBSR for teachers. Flook and colleagues (2013) studied the use of MBSR with 18 elementary school teachers. They incorporated MBSR with specific school-related activities and practices. The program took place over eight weeks for 2.5 hours per week and one day-long immersion program (six hours). Results of the study showed that teachers who participated had reductions in psychological symptoms and burnout, improvements in observer-rated classroom organization, and an increase in self-compassion. In a second study, Frank and colleagues (2015) conducted an MBSR training with 36 high school teachers. The program involved group discussions on the application of mindfulness in daily life, including in the classroom. Teachers were taught how to introduce mindfulness practice to their students. The sessions were for two hours a week for eight weeks and also included home practice. Results of the study suggested that teacher participants had improvements in self-regulation, self-compassion, mindfulness, and sleep quality.
Cultivating Awareness and Resilience in Education (CARE).
CARE is an evidence-based professional development program designed to reduce stress and improve teachers’ performance. The program focuses on three main content areas: (1) emotion skills instruction, (2) mindfulness/stress reduction practices, and (3) caring and listening practices ( Jennings et al. 2011 ). In a randomized control trial of CARE, with a waitlist control group, 53 teachers in urban and suburban schools participated in five full-day sessions over eight weeks and three 20-minute phone coaching sessions. Results showed improvements in well-being, teacher efficacy, burnout, and mindfulness ( Jennings et al., 2013 ). Future research is still needed to assess CARE’s effect on classroom and student outcomes.
Community Approach to Learning Mindfully (CALM).
CALM is a daily school-based intervention designed to promote and improve social-emotional competencies, stress management, well-being, teaching, and health. The intervention included yoga and mindfulness practices. Participants practiced skills four days a week for 16 weeks (64 sessions total). Study results showed that CALM was related to significant improvements in mindfulness, emotional functioning, positive affect, distress tolerance, efficacy in classroom management, as well as to decreases in physical symptoms, blood pressure, and cortisol levels ( Harris et al., 2016 ).
Recommendations and Next Steps
Wellness programs that focus on a broad array of wellness components such as nutrition, physical activity, and stress management have been shown to increase teacher morale, improve perceptions of being able to handle job stress, reduce absenteeism, and result in higher levels of overall well-being. Furthermore, in addition to the positive benefits of improved teacher job satisfaction, health, and well-being, there are documented cost savings and impacts on student outcomes related to having healthy teachers and school staff. Based on a review of the literature in workplace wellness and the evolving school staff wellness fields, the following recommendations are suggested for schools that intend to implement school staff wellness promotion programs:
- Tailor the program to the needs and interests of employees to promote motivation to participate;
- Target multiple components of wellness rather than just one or two components (e.g., physical health, mindfulness and stress reduction, positive behavior change, health education trainings);
- Incorporate the wellness program into the structure and the culture of the work environment by allowing employees time to participate in the wellness program (e.g., have wellness activity as part of already scheduled faculty meetings, integrate stress management practice into morning announcements that can be heard by students and staff);
- Incorporate and foster open and frequent communication between teachers and administrative staff to problem solve how to address and help reduce the stress experienced by school staff;
- Be mindful of the periods of increased stress for teachers (e.g., time leading up to standardized testing, the weeks leading up to a school vacation) when wellness program activities may be particularly needed;
- Leverage technology (e.g., mobile apps, virtual groups) to reach a broader audience and to increase participation;
- Integrate staff, student, family, and community wellness strategies and supports, when possible, to promote overall well-being in the school setting;
- Provide no-cost or low-cost wellness programming options for school staff; and
- Include screening and ongoing measurement opportunities to help document individual and group needs and progress.
In summary, the workplace wellness literature, when combined with the growing research literature in school staff wellness supports the idea that school employee wellness programs can promote improved physical, social, and emotional well-being in school staff while having a positive impact on student success and school climate, particularly as it relates to improved teacher attendance and, thus, improved academic continuity for students. The research also supports the economics of encouraging staff wellness and offers justification for the investment in wellness programs. Although there is much promise for the future of school staff wellness research, it is imperative that funders and school administrators recognize the importance of, and dedicate time and resources to, supporting school staff wellness. The field would benefit from an increased number of randomized controlled trials and from targeted funding opportunities to specifically support the well-being of school-based staff. As the research advances, it will be important to translate the research into effective frontline application and to be able to identify evidence-based programs as well as essential core elements of wellness program so as to maximize their impact and fiscal investment.
In addition to the positive benefits of improved teacher job satisfaction, health, and well-being, there are documented cost savings and impacts on student outcomes related to having healthy teachers and school staff.
- Aldana SG, Merrill RM, Price K, Hardy A, & Hager R (2005). Financial impact of a comprehensive multisite workplace health promotion program . Prevention Medicine , 40 , 131–137. [ PubMed ] [ Google Scholar ]
- Allensworth DD, & Kolbe LJ (1987). The comprehensive school health program: Exploring an expanded concept . Journal of School Health , 57 , 409–412. [ PubMed ] [ Google Scholar ]
- Alliance for a Healthier Generation (2016). Healthy Schools Program: Framework of Best Practices . Available at https://www.healthiergeneration.org/_asset/l062yk/07-278_HSPFramework.pdf .
- American Federation of Teachers (2015). Quality of Worklife Survey . Available at http://www.aft.org/sites/default/files/worklifesurveyresults2015.pdf [ Google Scholar ]
- American Psychological Association, Center for Organizational Excellence (APA, 2013). APA survey finds US employers unresponsive to employee needs [press release, March 5]. Available at http://www.apa.org/news/press/releases/2013/03/employee-needs.aspx .
- American Psychological Association (APA, 2015). Stress in America: Paying with Our Health . Available at https://www.apa.org/news/press/releases/stress/2014/stress-report.pdf .
- Baicker K, Cutler D, & Song Z (2010). Workplace wellness programs can generate savings . Health Affairs , 29 ( 2 ), 304–311. [ PubMed ] [ Google Scholar ]
- Byrne JJ (1998). Teacher as hunger artist: Burnout: Its causes, effects and remedies . Contemporary Education , 69 , 86–91. [ Google Scholar ]
- Centers for Disease Control and Prevention (CDC, 2014a). The CDC Worksite Health ScoreCard: An Assessment Tool for Employers to Prevent Heart Disease, Stroke, and Related Health Conditions . Atlanta, GA: U.S. Department of Health and Human Services. [ Google Scholar ]
- Centers for Disease Control and Prevention (CDC, 2014b). Whole School, Whole Community, Whole Child: A Collaborative Approach to Learning and Health . Alexandria, VA: ASCD; Available at https://www.cdc.gov/healthyschools/wscc/wsccmodel_update_508tagged.pdf . [ Google Scholar ]
- Chapman LS (2003). Meta-evaluation of worksite health promotion economic return studies . The Art of Health Promotion , 6 ( 6 ), 1–16. [ PubMed ] [ Google Scholar ]
- Chapman LS (2005). Meta-evaluation of worksite health promotion economic return studies: 2005 update . American Journal of Health Promotion , 19 ( 6 ), 1–11. [ PubMed ] [ Google Scholar ]
- Directors of Health Promotion and Education (DHPE, 2005). School Employee Wellness: A Guide for Protecting the Assets of Our Nation’s Schools . Washington, DC: Author; Available at http://c.ymcdn.com/sites/www.dhpe.org/resource/group/75a95e00-448d-41c5-8226-0d20f29787de/Downloadable_Materials/EntireGuide.pdf . [ Google Scholar ]
- Dworkin AG (2001). Perspectives on teacher burnout and school reform . International Education Journal , 2 , 69–78. Available at http://ehlt.flinders.edu.au/education/iej/articles/v2n2/dworkin/paper.pdf . [ Google Scholar ]
- Figley CR (1993). Compassion stress and the family therapist . Family Therapy News (February 1993), 1–8. [ Google Scholar ]
- Figley CR (1995) Compassion fatigue as secondary traumatic stress disorder: An overview In Figley CR (Ed.). Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized (pp. 1–20). New York: Brunner-Routledge. [ Google Scholar ]
- Fisher MH (2011). Factors influencing stress, burnout, and retention of secondary teachers . Current Issues in Education , 14 , 1–36. Available at http://cie.asu.edu/ . [ Google Scholar ]
- Flook L, Goldberg SB, Pinger L, Bonus K, & Davidson RJ (2013). Mindfulness for teachers: A pilot study to assess effects on stress, burnout, and teaching efficacy . Mind, Brain, and Education , 7 , 182–195. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Frank JL, Jennings PA, & Greenberg MT (2016). Validation of the Mindfulness in Teaching Scale . Mindfulness , 7 , 155–163. [ Google Scholar ]
- Frank JL, Reibel D, Broderick P, Cantrell T, & Metz S (2015). The effectiveness of Mindfulness-Based Stress Reduction on educator stress and well-being: Results from a pilot study . Mindfulness , 6 , 208–216. [ Google Scholar ]
- Gallup (2014). State of America’s Schools: The Path to Winning Again in Education . Available at http://www.gallup.com/services/178709/state-americaschools-report.aspx .
- Gray L, & Taie S (2015). Public School Teacher Attrition and Mobility in the First Five Years: Results from the First through Fifth Waves of the 2007-08 Beginning Teacher Longitudinal Study (NCES 2015-337) . U.S. Department of Education; Washington, DC: National Center for Education Statistics. Available at http://nces.ed.gov/pubs2015/2015337.pdf . [ Google Scholar ]
- Harris AR, Jennings PA, Katz DA, Abenavoli RM, & Greenberg MT (2016). Promoting stress management and well-being in educators: Outcomes of the CALM intervention . Mindfulness , 7 , 143–154. [ Google Scholar ]
- Hudnall Stamm B (2009). Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL) . Available at www.isu.edu/~bhstamm or www.proqol.org .
- Hydon S, Wong M, Langley AK, Stein BD, & Kataoka SH (2015). Preventing secondary traumatic stress in educators . Child and Adolescent Psychiatric Clinics of North America , 24 , 319–333. [ PubMed ] [ Google Scholar ]
- Ingersoll RM (1996). Teachers’ decision-making power and school conflict . The Sociological Quarterly , 69 , 159–176. [ Google Scholar ]
- Ingersoll RM (2001). Teacher turnover and teacher shortages: An organizational analysis . American Educational Research Journal , 38 , 499–534. [ Google Scholar ]
- Jennings PA, Frank JL, Snowberg KE, Coccia MA, & Greenberg MT (2013). Improving classroom learning environments by Cultivating Awareness and Resilience in Education (CARE): Results of a randomized controlled trial . School Psychology Quarterly , 28 , 374–390. [ PubMed ] [ Google Scholar ]
- Jennings PA, Snowberg KE, Coccia MA, & Greenberg MT (2011). Improving classroom learning environments by Cultivating Awareness and Resilience in Education (CARE): Results of two pilot studies . Journal of Classroom Interactions , 46 , 27–48. [ PubMed ] [ Google Scholar ]
- Kokkinos CM (2007). Job stressors, personality and burnout in primary school teachers . British Journal of Educational Psychology , 77 , 229–243. [ PubMed ] [ Google Scholar ]
- Lohrmann DK (2008). A complementary ecological model of the coordinated school health program . Public Health Reports , 123 , 695–703. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Mattke S, Liu H, Caloyeras JP, Huang CY, Van Busum KR, Khodyakov D, & Shier V (2013). Workplace Wellness Programs Study: Final Report . Santa Monica, CA: RAND Corporation; Available at http://www.rand.org/pubs/research_reports/RR254.html . [ PMC free article ] [ PubMed ] [ Google Scholar ]
- National Child Traumatic Stress Network, Secondary Traumatic Stress Committee (NCTSN, 2011). Secondary Traumatic Stress: A Fact Sheet for Child-Serving Professionals . Los Angeles, CA; Durham, NC: Author; Available at http://www.nctsn.org/sites/default/files/assets/pdfs/secondary_traumatic_tress.pdf . [ Google Scholar ]
- National Wellness Institute (NWI, n.d.). The Six Dimensions of Wellness . Available at http://www.nationalwellness.org/?page=Six_Dimensions .
- Oberle E, & Schonert-Reichl KA (2016). Stress contagion in the classroom? The link between classroom teacher burnout and morning cortisol in elementary school students . Social Science & Medicine , 159 , 30–37. [ PubMed ] [ Google Scholar ]
- Parks KM, & Steelman LA (2008). Organizational wellness programs: A meta-analysis . Journal of Occupational Health Psychology , 13 , 58–68. [ PubMed ] [ Google Scholar ]
- Partnership for Prevention (2010). Healthy Workforce 2010 and Beyond . Available at https://www.uschamber.com/sites/default/files/documents/files/HealthyWorkforce2010FINALElectronicVersion111709.pdf .
- Richardson KM, & Rothstein HR (2008). Effects of occupational stress management intervention programs: A meta-analysis . Journal of Occupational Health Psychology , 13 , 69–93. [ PubMed ] [ Google Scholar ]
- Saakvitne K, Gamble S, Pearlman LA, & Tabor Lev B (2000). Risking Connection: A Training Manual for Working with Survivors of Childhood Abuse . Baltimore, MD: Sidran. [ Google Scholar ]
- Taylor B, Zimmer C, & Womack SD (2005). Strategies to prevent teacher stress and burnout . ERIC Document Reproduction Service , ED490663 Available at http://files.eric.ed.gov/fulltext/ED490663.pdf . [ Google Scholar ]
- Travers CJ, & Cooper CL (1996). Teachers Under Stress: Stress in the Teaching Profession . London: Routledge. [ Google Scholar ]
- Tschannen-Moran M, & Woolfolk-Hoy A (2001). Teacher-efficacy: Capturing an elusive construct . Teaching and Teacher Education , 17 , 783–805. [ Google Scholar ]
- U.S. Department of Health and Human Services, Center for Disease Control and Prevention (DHHS, 2015). Results from the School Health Policies and Practices Study 2014 . Available at http://www.cdc.gov/healthyyouth/data/shpps/pdf/shpps-508-final_101315.pdf .
- U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health (DHHS, 1999). Stress … at Work (Publication No. 99-101). Available at https://www.cdc.gov/niosh/docs/99-101/pdfs/99-101.pdf .
- Zhang Q, & Sapp DA (2008). A burning issue in teaching: The impact of perceived teacher burnout and nonverbal immediacy on student motivation and affective learning . Journal of Communication Studies , 1 , 152–168. [ Google Scholar ]
Kia ora - welcome to our new website. We've tried to ensure old links will redirect to the correct pages, but some links may no longer work. Find out more .
About us Mō mātou
About the Ministry of Health and the New Zealand health system.
Quick links
- Consultations
New Zealand’s health system
- Government Policy Statement
- Health system roles and organisations
- Overview and statutory framework
- Vote Health
Organisation and leadership
- Chief clinical officers
- Executive Governance Team
- Ministry directorates
- Public Health Agency
- Statutory roles
Corporate publications
- Annual reports
- Briefings to incoming Ministers
- Health and Independence reports
- Mental health annual reports
- Strategic intentions
- Current vacancies
- Employee benefits
- Information for job applicants
Regulation & legislation Ngā here me ngā ture
Health providers and products we regulate, and laws we administer.
- Legislation we administer
- Rest home audit reports
Assisted dying
Certification of health care services, drug checking, health practitioners competence assurance act, medicinal cannabis, medicines control, mental health and addiction, notifiable diseases, pharmacy licensing, psychoactive substances, smoked tobacco, vaping, herbal smoking and smokeless tobacco, strategies & initiatives he rautaki, he tūmahi hou.
How we’re working to improve health outcomes for all New Zealanders.
Health strategies
- New Zealand Health Strategy
- Health of Disabled People Strategy
- Pae Tū: Hauora Māori Strategy
- Rural Health Strategy
- Te Mana Ola: The Pacific Health Strategy
- Women’s Health Strategy
Programmes and initiatives
- Gambling harm
- Health workforce
- Mental health, addiction and suicide prevention
- Pacific health
- Smokefree 2025
Māori health Hauora Māori
Increasing access to health services, achieving equity and improving outcomes for Māori.
- Subscribe for Māori health updates
Ao Mai te Rā anti-racism initiative
Māori health models, te tiriti o waitangi framework, wai 2575 health services and outcomes inquiry, whakamaua: māori health action plan, statistics & research he tatauranga, he rangahau.
Data and insights from our health surveys, research and monitoring.
- New Zealand Health Survey
- Health targets
System monitoring
- Mental health and addiction targets
- Planning and performance data
- New Zealand Gambling Survey
- Past surveys
Statistics and data sets
- Māori health data and statistics
- Mental health data and statistics
- Obesity data and statistics
- Suicide data and statistics
- Tobacco data and statistics
- COVID-19 and immunisation research projects
- Gambling harm research and evaluation
- Our role in health research
Mental health and addiction services data
A guide to data and information about the performance of mental health and addiction services.
- Mental health legislation and regulation
- Mental health initiatives
On this page
About this page.
This page contains data and information about the performance of mental health and addiction services.
Following the health and disability system reforms in July 2022, many of the data and information reporting functions have transferred to Health New Zealand – Te Whatu Ora. The Ministry of Health and Health New Zealand are committed to transparency and sharing available information publicly. There are 3 key areas that data falls into:
- Mental health and addiction service use – this information helps us understand the demand for services, how many people are accessing new and existing services, and how services are performing against expectations.
- Suicide statistics – this information helps us understand the rate of suicide within Aotearoa New Zealand, as well as the number of suspected intentionally self-inflicted deaths.
- Regulatory reporting – this information helps us understand how existing legislation is being used to assess and treat people with mental health and addiction needs.
Service use data are the responsibility of Health New Zealand, suicide statistics and related data are the responsibility of Health New Zealand and the Office of the Chief Coroner, and regulatory reporting remains a Ministry of Health responsibility.
There are also other mental health and addiction system monitors , independent of the Ministry of Health and Health New Zealand.
Mental health and addiction service use
Information on the performance of Aotearoa New Zealand’s mental health and addiction services helps us understand how long people have had to wait to be seen by mental health and/or addiction services, and the demographic breakdown of people accessing services.
- National Service Framework
One of the main sources for mental health and addiction data up until 2023 has been the National Service Framework Library. This site provided data on specialist mental health and addiction services, including:
- number of people and population percentages engaging with specialist services
- consumer experience and service quality rates (up to 2014)
- transition (discharge) planning
- waiting times.
The National Service Framework Library site has now been decommissioned. The National Service Framework is now the responsibility of Health New Zealand.
- Previous performance monitoring data published by the Ministry of Health
Specialist service use
Every year, approximately 175,000 people access specialist and non-government organisation (NGO) services for mental health and/or addiction support.
Using figures like these helps us understand trends about who is accessing services (for example, by age and ethnicity) and which types of services people are accessing (for example, former district health board/Health New Zealand or NGO).
Health New Zealand publishes information on service use using the Mental Health and Addiction: Service Use web tool .
Expanding Access and Choice of Primary Mental Health and Addiction supports
A key component of the Wellbeing Budget 2019 was investment in a programme of work to ‘expand access and choice of primary mental health and addiction supports’ across Aotearoa New Zealand (known as Access and Choice). The establishment of services started in late 2019 with national rollout phased over a 5-year period. There are no criteria to access these services, no cost, and support is immediate and rapid. There are 4 main workstreams:
- Integrated Primary Mental Health and Addiction (IPMHA) services accessed through general practice
- Kaupapa Māori primary mental health and addiction services accessed primarily through kaupapa Māori NGOs and community providers
- Pacific primary mental health and addiction services accessed primarily through Pacific-led community-based organisations
- Youth primary mental health and addiction services accessed through NGOs, community-based organisations, and youth one-stop shops.
Data from these Access and Choice services can be found on the Access and Choice programme website .
Suicide statistics
The Office of the Chief Coroner and Health New Zealand publish confirmed and provisional suicide statistics, or suspected intentionally self-inflicted deaths, annually. Provisional suicide statistics relate to deaths where suicide is suspected but has not yet been confirmed by a coroner; some cases recorded as provisional may eventually be found not to be suicides. Confirmed suicide statistics are based on the number of suicides confirmed by coroners, or where there is sufficient other evidence to conclude the death was a suicide.
- Suicide web tool by Health New Zealand and the Office of the Chief Coroner
- Coronial Services of New Zealand
Regulatory reporting
There are two main pieces of legislation relating to mental health and addiction: the Mental Health (Compulsory Assessment and Treatment) Act 1992 (the Mental Health Act) and the Substance Addiction (Compulsory Assessment and Treatment) Act 2017 (SACAT). The Director of Mental Health and the Director of Addiction Services are statutory roles under these Acts respectively.
Each year, approximately 11,000 people in Aotearoa New Zealand are subject to treatment or assessment under either of those Acts.
The Ministry of Health reports on the use of SACAT legislation in our annual report. The use of the Mental Health Act, and other provisions related to mental health and addiction treatment, are reported annually in the Office of the Director of Mental Health and Addiction Services’ Regulatory Report.
- Ministry of Health Annual Report
- Office of the Director of Mental Health and Addiction Services’ Regulatory Report
More reports related to the use of legislation, including guidelines and earlier reports, can be found on the publications webpage.
- Mental health and addictions publications
- Mental Health Act guidelines
Due to the time it takes to quality check the data, these reports can take a while to be published. However, the Ministry of Health and Health New Zealand are committed to working together to improve this process.
- Mental Health Review Tribunal Annual Reports
The Mental Health Review Tribunal is an independent body appointed by the Minister of Health under the Mental Health Act to help support and protect the rights and interests of people subject to that Act.
The Tribunal’s Annual Reports cover the types of applications they received, and the outcomes of these applications.
Other mental health and addiction system monitors
Before 9 February 2021, responsibility for monitoring and advocacy for improvement to mental health and addiction services was held by the Health and Disability Commissioner.
Now, Te Hiringa Mahara – the Mental Health and Wellbeing Commission has responsibility of providing independent system-level oversight of mental health and wellbeing, and holding the government of the day and other decision-makers to account for the mental health and wellbeing of people in Aotearoa New Zealand. The commission publishes monitoring reports on mental health and addiction service provision.
- Health and Disability Commission
- Te Hiringa Mahara – Mental Health and Wellbeing Commission
Te Tāhū Hauora Health Quality & Safety Commission also plays an important role in working with clinicians, providers and consumers to improve health services. They maintain a national quality improvement programme and support mental health and addiction services with data and coaching.
- Health Quality & Safety Commission
Mental health
Related areas.
- email Email
- print Print
- chat Feedback
© Ministry of Health – Manatū Hauora
Putting science to work for the health of women
Driving Change in Women’s Health: Innovations in Funding, Research, and Policy
By dr. janine a. clayton, transforming women’s behavioral health services.

In a significant move to bolster women’s behavioral health services, the Biden administration has announced a series of funding opportunities totaling $27.5 million. This announcement underscores a steadfast commitment to addressing the distinct mental health and substance use treatment needs of women across the United States. The funds, provided by the U.S. Department of Health and Human Services (HHS) through the Substance Abuse and Mental Health Services Administration, include $15 million for the Community-Based Maternal Behavioral Health Services Program , which aims to improve access and ensure smooth care transitions of culturally relevant, evidence-based treatment for pregnant and postpartum women. Additionally, $12.5 million will support the Women’s Behavioral Health Technical Assistance Center , designed to enhance health care providers’ ability to address women’s behavioral health needs through training and technical assistance.
These efforts are particularly critical in light of recent research highlighting mental health disparities among racially and ethnically minoritized (REM) women in the U.S. A scoping review on mental health during the menopause transition revealed that REM women experience a higher burden of depressive symptoms, influenced by a range of social, structural, and biological factors. The review also emphasized the need for culturally relevant care and enhanced provider training to effectively address these disparities. The Biden administration’s funding directly targets these needs, ensuring that REM women have access to comprehensive and tailored mental health care.
The funding investments are aligned with the goals of the White House Initiative on Women’s Health Research , which has committed to prioritizing investments in women’s health research, integrating women’s health across the federal research portfolio, and galvanizing new research on midlife health of women. These funding announcements signify more than just financial support; they represent a pivotal shift in how women’s health is prioritized on the national agenda and lay the groundwork for sustained improvements in women’s health care infrastructure. Allocating resources to targeted programs ensures that women receive the care and support necessary to lead healthier, more fulfilling lives.
NIH Women’s Health Roundtable: Endometriosis
On August 19, 2024, the Office of Research on Women’s Health (ORWH), in collaboration with the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), co-hosted the second NIH Women’s Health Research Roundtable on endometriosis, titled “ Beyond the Lesion: Charting New Paths .” This Roundtable Series was developed in response to a Presidential Memorandum aimed at highlighting priority topics within HHS and disseminating information on federally supported research areas.
This significant event centered on endometriosis, a chronic and often misunderstood condition in which tissue similar to the uterine lining grows outside the uterus. Endometriosis affects approximately 10% of women of reproductive age and often results in severe pain, heavy menstrual periods, and infertility, yet remains underdiagnosed and inadequately treated. The roundtable brought together experts, advocates, and individuals affected by the condition to explore the latest research, address challenges, and discuss future directions for research on this debilitating disease.
The event featured distinguished speakers, starting with opening remarks by NICHD Director Diana W. Bianchi, M.D. Attendees then engaged in a series of insightful presentations covering diverse aspects of endometriosis, from patient experiences and holistic health approaches to cutting-edge research. This roundtable underscored our commitment to advancing knowledge, improving care, and fostering collaboration to enhance understanding and treatment of endometriosis, with the ultimate goal of improving the quality of life for the women affected.
In Focus 7.2: Women and Mental Health Across the Lifespan
I am thrilled to share with you the latest advancements and initiatives showcased in our most recent issue of Women’s Health In Focus at NIH . A key feature of this issue is the groundbreaking work conducted by Jill Goldstein, Ph.D., M.P.H., at the Innovation Center on Sex Differences in Medicine (ICON-✘) . Dr. Goldstein is a Specialized Centers of Research Excellence (SCORE) on Sex Differences investigator and is leading the charge in examining how sex differences impact brain function, psychiatric disorders, and related comorbidities such as cardiovascular disease. Her team is pioneering the development of sex-specific tools and therapies, a crucial advancement with the potential to lead to improved diagnosis and treatment for women. This shift is consistent with increased awareness of the importance of women’s mental health research. ORWH is supporting Dr. Goldstein in her collaboration with Stuart Tobet, Ph.D., and other experts to create an innovative biomedical pipeline curriculum centered on sex differences, known as the Translational Workforce Innovation Network (TWIN) .
This issue also highlights the impressive achievements of the University of Minnesota’s Center for Women in Medicine and Science (CWIMS) . Since its inception in 2018, CWIMS has been instrumental in promoting gender equity within its medical school. CWIMS’ innovative approaches include conducting salary equity studies, developing a metrics dashboard for tracking progress, and implementing programs such as the Distinguished Visiting Scholar mechanism and the Early Pathways to Success Program. Recently, CWIMS hosted a Mid-Career Summit, addressing this crucial stage of faculty development. These initiatives have led to increased representation and advancement of women and underrepresented minorities in academic medicine. Be sure to check out the full publication to stay informed and inspired by the groundbreaking work and initiatives in women’s health research.
Advancing Autoimmune Disease Research
I am excited to share with you the significant strides we are making in the field of autoimmune disease research through the Office of Autoimmune Disease Research (OADR-ORWH) . OADR-ORWH is dedicated to promoting research that elucidates sex differences in autoimmune conditions, ultimately leading to more effective and personalized treatments for both women and men. Our goal is to foster research to address critical gaps in understanding of how sex differences influence the onset, progression, and treatment of autoimmune diseases. Autoimmune diseases disproportionately affect women, accounting for nearly 80% of all cases. This disparity underscores the urgent need for research that considers sex as a fundamental variable in understanding these complex diseases.
A key event highlighting our commitment to this mission was the recent ScienceTALKS event titled “ Going Viral: Exploring Viral Triggers of Autoimmune Diseases .” This event brought together leading experts to delve into the intricate relationship between viral infections and the onset of autoimmune diseases. Presentations explored how viruses can trigger autoimmune responses, which is crucial for developing preventive and therapeutic strategies.
Additionally, OADR-ORWH announced the publication of a new article titled “ Coordination and Collaboration to Support Exposome Research in Autoimmune Diseases ” in Arthritis Care & Research . I am honored to have collaborated on this article with OADR-ORWH Director Victoria Shanmugam, MBBS, MRCP, FACR, CCD, and ORWH Associate Director of Clinical Research Sarah Temkin, M.D., alongside partners in the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute of Environmental Health Sciences. The exposome is a concept that measures all exposures (internal and external) of an individual in their lifetime and how those exposures relate to health. The publication examines the critical role of the exposome in shaping current and future autoimmune disease research at NIH, the impact of environmental exposures on autoimmune diseases, and NIH’s ongoing efforts to interpret these complex interactions.
The insights shared through these events and publications will shape the future of autoimmune disease research. I extend my gratitude to all speakers, participants, and organizers for their invaluable contributions. For those who missed it, visit our event page for the recording and materials. Together, we can continue to advance research that makes a difference.
Women’s Equality Day
As we reflect on August, a month rich with significant milestones in women’s health and equity, we are reminded of the strides made and the work ahead. Women’s Equality Day, celebrated on August 26, underscores our ongoing commitment to gender equality, commemorating the anniversary of the certification of the 19th Amendment. This day serves as a powerful reminder of the ongoing pursuit of gender equality and the importance of ensuring women’s voices are heard in all aspects of society, including health research and policy.
Historically, reliance on male models in research has created significant knowledge gaps, and we have been working diligently to address these disparities. Data reveal that while women are more likely to donate organs, they are less likely to receive them for transplantation and are less frequently given CPR compared to men. At ORWH, we emphasize that women’s health equity and inclusion are not just goals but central to achieving healthy communities and a just society. Through rigorous research, we strive to support the generation and application of evidence to ensure that all women can attain their highest level of health.
A cornerstone of our efforts is the Health of Women of Understudied, Underrepresented, and Underreported populations (U3) Populations Data Book . This comprehensive resource provides critical data and insights into the health disparities faced by these populations. By highlighting these disparities, the Data Book underscores our commitment to addressing the specific health needs of diverse groups of women, including those in rural locations and other underserved communities.
Our website offers a variety of programs, tools, and resources. Key among these is the NIH Inclusion Outreach Toolkit , a vital resource for researchers. This toolkit provides comprehensive guidance on the importance of including women in clinical research, offering tools and best practices to support inclusion. In addition, ORWH collaborates with NIH ICs on research programs aimed at addressing women’s health disparities . For instance, the U3 Interdisciplinary Research Program , focuses on advancing health outcomes for populations highlighted in the Data Book. ORWH also supports initiatives such as our partnership with the National Institute of General Medical Sciences (NIGMS) and other NIH institutes to advance women’s health research and equity, particularly in Institutional Development Awards (IDeA) states . These states and territories benefit from targeted funding aimed at expanding research capacity and addressing health disparities.
As we continue to enhance women’s health research, I invite you to explore our resources and join us in our mission to foster a future where every woman receives evidence-based health care.
Looking Ahead: Upcoming Events in Women’s Health Research
As we continue to drive progress in women’s health, I am excited to highlight two key upcoming events that promise to advance our understanding and impact. On September 30, 2024, the Specialized Centers of Research Excellence (SCORE) on Sex Differences will host its 2024 annual meeting, featuring a keynote address that emphasizes crucial advancements in research on sex differences and a capstone address that maps out contemporary challenges within the health enterprise. This initiative is pivotal to bridging gaps in understanding sex influences in health and disease. Following this event, on October 1, 2024, the Building Interdisciplinary Research Careers in Women’s Health (BIRCWH) 2024 Annual Meeting will take place. This event will provide a comprehensive platform for discussing and fostering interdisciplinary research careers in women’s health. I encourage everyone to engage in these important events as we continue to advance research, career development, and policy in women’s health. They will not only showcase ongoing research, but also set the stage for future breakthroughs.
Thank you for your ongoing support and dedication to improving women’s health and well-being. I look forward to sharing more updates and breakthroughs with you in the coming months.
- Previous Message
- Back to Top
Director’s Messages
August 29, 2024
June 28, 2024
May 31, 2024
April 30, 2024
IMAGES
VIDEO
COMMENTS
Research shows that students who work more than 20 h a week have lower grades and difficulty completing their academic work (Benner and Curl, 2018). Schaufeli and Enzmann (1998) considered that burnout is a conflict that occurs between the different roles that an individual must play and his perception of time pressure.
Ready, & Astani, 2014). Consequently, research has found students' work hours had an inverse . WORK, ... strain on mental health in working students is the additional pressures from employers and ...
Student mental health and well-being: ... adults navigate societal challenges, and they are essential for preparing students to succeed in school, work, and civic life. When schools closed, students' relationships were disrupted, as ... A 2017 Pew Research survey of drug use and health
Our study aimed to shed light on the work-related mental health issues affecting graduate students, providing a comprehensive research work including psychological and biological assessment. Our findings showed that a sizeable number of graduate student present anxiety, depression, or high burnout and that the time spent in academia plays an ...
UK university students (N = 385) submitted 991 questions, categorised into seven themes: epidemiology, causes and risk factors, academic factors and work-life balance, sense of belonging, intervention and services, mental health literacy and consequences. Across themes, respondents highlighted the importance of understanding the experience of ...
Poor mental health of students in further and higher education is an increasing concern for public health and policy [1,2,3,4].A 2020 Insight Network survey of students from 10 universities suggests that "1 in 5 students has a current mental health diagnosis" and that "almost half have experienced a serious psychological issue for which they felt they needed professional help"—an ...
The majority of college students work, and there are well-documented findings about the impacts of student work on academic performance. ... it can cause students' social lives and mental health to suffer; and, despite these negative impacts, students find work to be fulfilling. With these understandings, we propose ways that university ...
As with youth mental health (Wilson, 2020 ), research into student mental health (and well-being) is influenced by the differing priorities of individual research teams, as well as cultural context, and policy. Moving forward, research should also represent the priorities of students and universities, including a pragmatic focus on factors ...
Graduate students are faced with an array of responsibilities in their personal and professional lives, yet little research has explored how working students maintain a sense of well-being while managing work, school, and personal-life. Drawing on conservation of resources theory and work-family enrichment theory, we explored personal, psychological resources that increase enrichment and ...
Professional studies and relevance of job for future career was cited least (Table 3). According to the majority of students, part-time work affected their academic performance (44%, n =88) and some had to work a night shift 3-4 times a week ( n =144, 72%). Only 32% of students studied more than 3 hours in a day ( n =64).
The number of students seeking help at campus counseling centers increased almost 40% between 2009 and 2015 and continued to rise until the pandemic began, according to data from Penn State University's Center for Collegiate Mental Health (CCMH), a research-practice network of more than 700 college and university counseling centers (CCMH Annual Report, 2015).
Gair S, Baglow L (2018a) 'We barely survived': social work students' mental health vulnerabilities and implications for educators, universities and the workforce. ... et al. (2016) Reducing the mental health-related stigma of social work students: a cluster RCT. Research on Social Work Practice 28(2): 164-172. Crossref. Google Scholar ...
Previous research has linked working for pay while attending university with negative academic and health outcomes; yet, working students are often resilient when experiencing such adverse circumstances. This makes it crucial to explore potential psychological mechanisms that transform adverse experiences into sources of motivation and persistence for working students. We explore one mechanism ...
The substantial demands on women likely exacerbate the pandemic's impacts, suggesting a gender-related influence on susceptibility to mental health challenges. face time limitations, emphasizing ...
Mental health inventory. The third research instrument will measure the students' health status using the mental health inventory (MHI-38) by the Australian Mental Health Outcomes and Classification Network (AMHOCN). MHI-38 is composed of 38 questions which require an answer from five to six-point scale.
The majority of working students in our sample work off campus: 72.3%. work off campus, including virtual work, while 41.7% work on campus, including virtual work. (some students hold on- and off-campus jobs simultaneously). 68.7% of students work 20 hours. or less per week, while 31.2% work over 20 hours per week.
Given the increase in mental health problems among students and the surge in demand for formal support [1, 20, 21], reactive services alone cannot effectively support student mental health and wellbeing . Educational institutions have recognised the need to move beyond traditional forms of support and provide alternative, more accessible ...
Our study aimed to shed light on the work-related mental health issues affecting graduate students, providing a comprehensive research work including psychological and biological assessment. Our findings showed that a sizeable number of graduate student present anxiety, depression, or high burnout and that the time spent in academia plays an ...
Second, as most PhD students are part of larger research teams, whose composition determines scientific impact (Lee et al., 2015), PhD students with mental health issues may pose a considerable cost to research institutions and teams. To date, research policy efforts seemed to have focused more on 'hard outcomes' such as publications ...
The intervention worked for people from various age groups, including college students and middle-aged adults, researchers learned after analyzing seven studies on peer-led mental health programs written or published between 1975 and 2021. Researchers found that participants also became less likely to identify with negative stereotypes ...
Organizational policies that are linked to mental health problems will lead indi-viduals to quit their PhD studies or leave the research industry altogether (Podsakoff et al., 2007). Several studies of PhD students suggest that the dropout numbers range from 30 to 50 percent, depending on the scientific discipline and country (Stubb et al., 2012).
One study showed that 70% of college students are stressed about finances. [1] With work, school, activities, and friends all demanding attention, many students struggle with balancing and prioritizing the different areas of their lives. We know that high levels of stress hurt our mental health. With the growing rates of anxiety, depression ...
The link between physical activity and mental health has been widely accepted for many years. In recent years though, an increasing body of university-led evidence has demonstrated how critical this link is to the success of university students around the world. Peer-reviewed studies out of the UK, Malaysia, Hong Kong and Norway show remarkable similarities across the student cohorts studied ...
The vast majority of ACC students are working and attending college. Approximately 60 percent say they worry about paying for college, and 30 percent are parents. When we help our students meet their basic needs (food, housing, child care, transportation, and mental health), they can better focus on learning. Read more about ACC's Theory of Change.
In a 2012 U.S. survey, 1.9 percent of 34,525 adults reported that they had practiced mindfulness meditation in the past 12 months. Among those responders who practiced mindfulness meditation exclusively, 73 percent reported that they meditated for their general wellness and to prevent diseases, and most of them (approximately 92 percent) reported that they meditated to relax or reduce stress.
The focus was to investigate how first-year undergraduate students transition into the unknown university environment as they come from various backgrounds. A case study research design was employed in the study. The population included first-year students across all schools in various areas of specialisation at the South African University.
Visiting Students and Scholars; Research. ... Corcoran was the first person in social work to publish a book on evidence-based practice, "Evidence-Based Social Work Practice with Families," which she wrote in 2000 as an assistant professor. Her areas of scholarship include adult and youth mental health, and her methodological specialty ...
Work-Related Stress for Educators. Individuals working in school settings are particularly vulnerable to work-related stress. Data from the 2013 Gallup-Health-ways Well-Being Index found that 46% of teachers in K-12 settings report high levels of daily stress during the school year. This level of stress is similar to that of nurses (46%) and physicians (45%) and is the highest (along with ...
The Ministry of Health reports on the use of SACAT legislation in our annual report. The use of the Mental Health Act, and other provisions related to mental health and addiction treatment, are reported annually in the Office of the Director of Mental Health and Addiction Services' Regulatory Report. Ministry of Health Annual Report
These efforts are particularly critical in light of recent research highlighting mental health disparities among racially and ethnically minoritized (REM) women in the U.S. A scoping review on mental health during the menopause transition revealed that REM women experience a higher burden of depressive symptoms, influenced by a range of social ...